
Abstract
To establish a new method for the diagnosis of dengue secondary infection, 187 serum samples from the patients with dengue secondary infection, 40 serum samples from the patients with dengue primary infection, and 44 serum samples from the healthy volunteers were tested using the dengue IgG indirect enzyme-linked immunosorbent assay (DEN IgG ELISA). The results of the test were compared with those from the dengue hemagglutination inhibition (DEN HI) test, which has been recommended as the gold standard by the World Health Organization (WHO, 1997). Japanese encephalitis IgG indirect ELISA (JE IgG ELISA) was also performed to measure anti-flavivirus IgG, which cross-reacts with the Japanese encephalitis virus, to test the possibility of an alternative to DEN IgG ELISA. The results of DEN IgG and JE IgG ELISAs were highly correlated with those of the DEN HI test. In the DEN IgG ELISA, a titer of 1:29,000 was the cut-off value for the diagnosis of dengue secondary infection (91.5% accuracy [95% confidence interval, CI], 90.9% sensitivity [95%CI], and 92.9% specificity [95%CI]). A titer of 1:52,000 was the cut-off value for dengue secondary infection using JE IgG ELISA (95.6% accuracy [95%CI], 98.9% sensitivity [95%CI], and 88.1% specificity [95%CI]). In conclusion, this study confirmed that the results of both DEN IgG and JE IgG ELISAs were highly correlated with the results of DEN HI test. Thus, these ELISAs are simple, rapid, sensitive, and quantitative tests that can be used in the determination of dengue secondary infection.
Introduction
Because the diagnosis of secondary dengue infection is of critical importance, various techniques for the detection of secondary infections have been reported: the dengue hemagglutination (HA) inhibition (DEN HI) test, a combination of the DEN IgM-capture enzyme-linked immunosorbent assay (DEN IgM ELISA) and the DEN IgG-capture ELISA (Innis et al. 1989, Shu et al. 2003, A-nuegoonpipat et al. 2006, Falconar et al. 2006), the immunochromatography (Vaughn et al. 1998, Cuzzubbo et al. 2001), and the dengue antigen-capture IgG ELISA (Chungue et al. 1989, Miagostovich et al. 1999). The WHO (1997) recommends the DEN HI test as the gold standard for the diagnosis of secondary dengue infection. However, the DEN HI test is time-consuming because of the multiple steps required for serum sample processing (Chungue et al. 1989, Lam and Devine 1998, Miagostovich et al. 1999). The dengue IgG indirect ELISA (DEN IgG ELISA) is a reliable and rapid technique that permits the determination of anti-dengue IgG antibodies (Bundo-Morita et al. 1986) in a large number of samples. The IgG indirect ELISA and the HI test give highly consistent results for the diagnosis of flaviviruses, such as dengue virus (Lam and Devine 1998, Sang et al. 1998) and Japanese encephalitis virus (Xinglin et al. 2005, Yang et al. 2006).
The purpose of this study was to evaluate the DEN IgG ELISA as an easy and rapid alternative method for the determination of secondary dengue infection that might ultimately replace the conventional DEN HI test. Anti-dengue IgG antibodies exhibit high cross-reactivity with other flaviviruses, including Japanese encephalitis virus (Bundo-Morita et al. 1986, Figueiredo et al. 1989, Vaughn et al. 1998, Martin et al. 2002, Yamada et al. 2003). Therefore, we also aimed to evaluate the applicability of the Japanese encephalitis IgG indirect ELISA (JE IgG ELISA) for the diagnosis of secondary dengue infection by determination of cross-reactivity of anti-flavivirus IgG with Japanese encephalitis antigen.
Materials and Methods
Patients and study design
In total, 271 serum samples were used for this study. Most (197) of these samples were from patients who had been found to have dengue virus infections based on clinical symptoms and on a positive DEN HI test at either San Lazaro Hospital or St. Luke's Medical Center between 1999 and 2002. First serum samples were taken 3–7 days after the onset of illness. Twenty-one cases showed ≥1:2560 in the first extracted samples; thus, no more sampling was done. However, second serum samples were taken from the remaining 176 cases after 7 days from the first sample taken because of no or low anti-DEN HI titer (<1:2560).
Of these 197 samples, 187 were classified using the DEN HI test as secondary dengue infections and 10 were classified as primary infections. An additional 30 samples were from patients who had been found to have primary dengue infections and were kindly provided by the National Institute of Infectious Diseases (Tokyo, Japan). Primary and secondary dengue infections were differentiated using the WHO criteria (WHO 1997). Age-matched healthy volunteers (a total of 44), who were enrolled at St. Luke's Medical Center during the same period, served as dengue-negative controls. The study protocol was approved by the Bioethics Committees of both San Lazaro Hospital and St. Luke's Medical Center. Parents or guardians of all patients and healthy volunteers provided written informed consent.
HI test
The HI test was performed according to the method of Clarke and Casals (1958) modified for microtiter equipment. Four HA units of dengue-1 (Hawaii), dengue-2 (00St-22A), dengue-3 (SLMC50), and dengue-4 (SLMC318) acetone-extracted antigens were prepared and used as four unique monovalent DEN HI test antigens.
Dengue virus-infected culture fluid (ICF) was mixed with 3% bovine serum albumin in phosphate-buffered saline (PBS) and 8.5% sucrose in H2O at a ratio of 1:1:8 to stabilize HA antigenicity. The virus solution was mixed gently with cold acetone and then incubated on ice for 10 min to both precipitate and inactivate the virus. The centrifuged and dried precipitate was resuspended with normal saline and used as the HI test antigens.
To inactivate hemolysin, 100 μL of serum was heat-treated at 56°C for 30 min. Next, the sera were mixed vigorously with 2.5 mL of cold acetone, followed by incubation on ice for 5 min to remove nonspecific HA inhibitors. The resulting precipitate was dried and resuspended in borate saline (pH 9.0) and then mixed with 20% goose red blood cells (GRBCs) in an ice bath for 20 min to absorb natural hemagglutinins. The supernatant was collected and used as 10-fold diluted serum samples.
For the HI test, 25 μL of pretreated and 10-fold diluted serum samples were further twofold diluted serially in 0.4% bovine serum albumin in borate saline ranging from 1:10 to 1:10,240. To each well of a microtiter plate were added 25 μL of HI test antigen (4 HA units), which was then incubated overnight at 4°C. The following day, 50 μL of 0.33% GRBCs was added and the plate was incubated at 37°C for 1 h. The HI titer was expressed as the reciprocal of the highest dilution that showed complete inhibition of HA. The HI test antigens were prepared and used as four serotypes of a monovalent antigen and not as a mixed tetravalent antigen. Based on WHO (1997) criteria, a serum HI antibody titer of 1:2560, or greater, in samples collected at any time during illness was indicative of a secondary dengue infection. A primary dengue infection was defined as at least a fourfold increase in the HI titer in samples collected during the convalescent phase of the illness relative to the acute phase sample.
IgG indirect ELISA
An in-house DEN IgG ELISA and an in-house JE IgG ELISA were performed according to the methods described by Bundo-Morita et al. (1986). DEN viruses (D1: Hawaii, D2: ThNH07/93, D3: PhMH4/84, D4: CT93/158) purified from an ICF of C6/36 cells were used as the DEN tetravalent antigen for the DEN IgG ELISA to minimize the nonspecific reactions. Japanese encephalitis viruses (JaOArS982) purified from an ICF were used as the JE antigen for the JE IgG ELISA. Each virus serotype was concentrated using polyethylene glycol 6000 and NaCl. The concentrated viruses were purified by sucrose-gradient ultracentrifugation at 50,000 g for 14 h at 4°C (Bundo and Igarashi 1983). The tetravalent purified DEN antigen and the monovalent purified JEV antigen were diluted at 250 ng/100 μL with coating buffer (0.05 M carbonate–bicarbonate buffer, pH 9.6). High-protein–binding 96-well microplates (Maxisorp; NalgeNunc International, Roskilde, Denmark) were coated with antigen (250 ng/100 μL/well) and were then incubated either at 37°C for 1 h or at 4°C overnight. Blockace (SnowBrand, Sapporo, Japan) was added to all the wells and incubated for 1 h at room temperature. The plate was washed three times with PBS containing 0.05% Tween 20 (PBS-T), and then test sera was diluted at 1:1000 in PBS-T + 10% Blockace and added in duplicate to the plates. Control serum known to contain the antibody to test antigen was run on each plate as a positive control. After incubation at 37°C for 1 h, the plate was washed and 100 μL/well of 1:30,000-diluted horseradish peroxidase-conjugated anti-human IgG goat IgG (American Qualex, San Clemente, CA) in PBS-T + 10% Blockace was added to the plate. The plate was incubated at 37°C for 1 h, followed by washing and initiation of the peroxidase reaction by addition of 100 μL/well of substrate solution. The substrate solution consisted of 5 mg of O-phenylenediamine dihydrochloride (Sigma Chemical, St. Louis, MO) and 0.03% hydrogen peroxide in 10 mL of 0.05 M citrate–phosphate buffer at pH 5.0. The plate was incubated at room temperature for 15–30 min in the dark and then the reaction was stopped by addition of 100 μL/well of 1 N hydrochloric acid. A standard curve was prepared using the OD492 values of the dengue-positive control serum starting with a 1000-fold dilution, followed by serial twofold dilutions up to 1:212 in PBS-T + 10% Blockace. To simplify the calculation of IgG titer in patient serum samples, the dilution of dengue-positive control serum that showed the OD492 most similar to that of the 1000-fold diluted dengue-negative standard serum was arbitrarily designated as 1:1000 because all of the serum samples were diluted at 1:1000. The lesser dilutions of the dengue-positive control serum were designated as 1:2000, 1:4000, and 1:8000 up to the initial 1000-fold dilution (Bundo et al. 1981). Then, the IgG titers of patient sera were determined from the positive standard curve. A sample titer equal to, or greater than, 1:3000 (cut-off value of positive IgG was at 1:1000 + 3 standard deviations) was considered IgG-positive for dengue virus.
Statistical analysis
Pearson's correlation coefficient was used to examine the significance of correlations between results of the DEN HI test and the IgG ELISAs. Receiver operating characteristic (ROC) curve analysis was used to evaluate the ability of the IgG ELISAs to distinguish between secondary and primary dengue infections. The area under the ROC curve (AUC) was used to quantify the accuracy of the IgG ELISAs. The sensitivity and specificity of the IgG ELISAs were determined at each cut-off point. The optimal cutoff point for the IgG ELISAs was defined as the maximal sum of the sensitivity and specificity estimates. A 95% confidence interval (95% CI) was calculated using the Fleiss quadratic method. All statistical tests were performed using SPSS 14.0, Epi Info ver. 6.04d, and Systat 11 software.
Results
Serum samples were obtained from 227 patients who were confirmed to be dengue-positive, and 44 serum samples were collected from healthy volunteers for comparison of the DEN HI test, DEN IgG ELISA, and JE IgG ELISA. Use of the JE IgG ELISA as an alternative to the DEN IgG ELISA was evaluated by measurement of cross-reactivity with anti-flavivirus IgG.
Comparison of the DEN IgG ELISA with the DEN HI test
The titers determined using the DEN HI test and DEN IgG ELISA were highly correlated (Fig. 1). The ROC of DEN IgG ELISA titer by DEN HI titer is shown in Figure 4. The optimal cut-off value for secondary dengue infection using the DEN IgG ELISA titer was obtained at 1:29,000 with 91.5% accuracy (95% CI: 87.4–94.4), 90.9% sensitivity (95% CI: 85.6–94.5), and 92.9% specificity (95% CI: 84.5–97.1) (Table 1).

Correlation between the DEN HI test and DEN IgG ELISA titers. The vertical line represents a DEN HI test result of 2560. The horizontal line represents a DEN IgG ELISA result of 29,000. DEN IgG ELISA, dengue IgG indirect enzyme-linked immunosorbent assay; DEN HI test, dengue hemagglutination inhibition test.
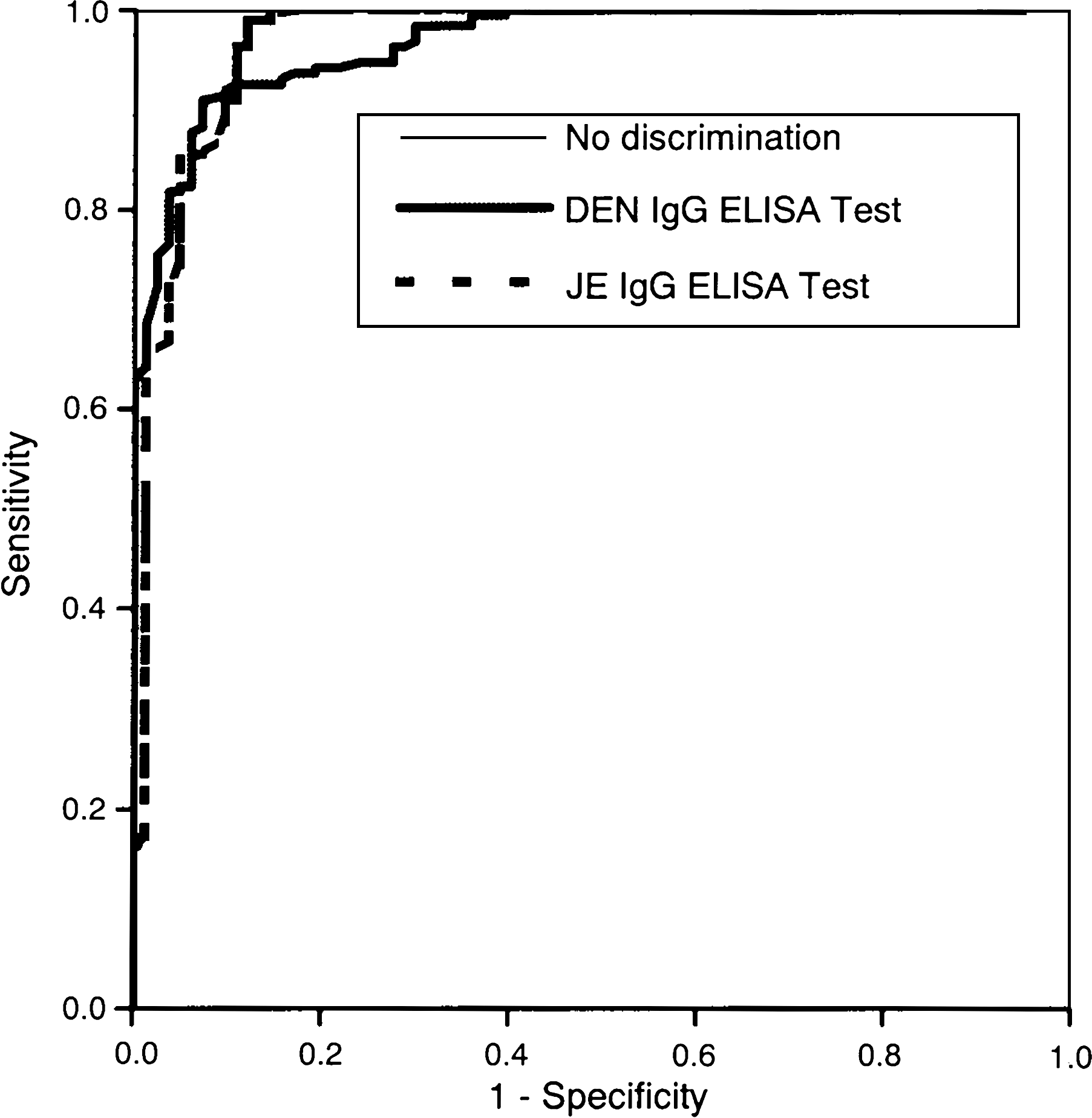
Receiver operating characteristic curves of the DEN IgG ELISA and JE IgG ELISA titers by DEN HI test titers (secondary dengue infection vs. primary dengue infection and negative dengue infection).
DEN IgG ELISA, dengue IgG indirect enzyme-linked immunosorbent assay; JE IgG ELISA, Japanese encephalitis IgG indirect ELISA; CI, confidence interval; ppv, positive predictive value; NPV, negative predictive value.
Comparison of the JE IgG ELISA with the DEN HI test
Similarly, the titers determined using the DEN HI test and JE IgG ELISA also were highly correlated (Fig. 2). The ROC of JE IgG ELISA titer by DEN HI test titer is shown in Figure 4. The optimal cut-off value for secondary dengue infection using the JE IgG ELISA titer was 1:52,000 with 95.6% accuracy (95% CI: 92.2–97.6), 98.9% sensitivity (95% CI: 95.8–99.8), and 88.1% specificity (95% CI: 78.8–93.8) (Table 1).
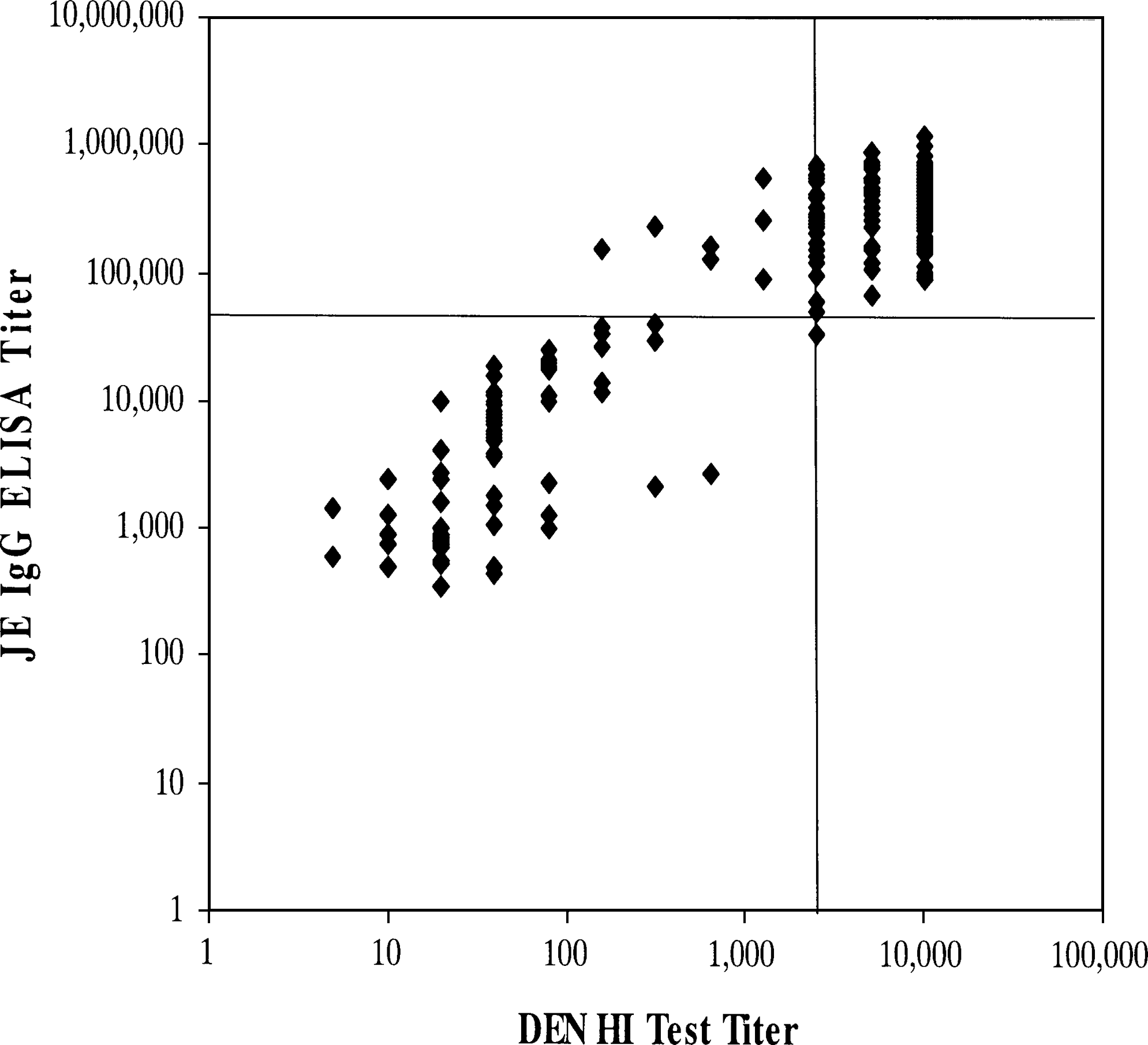
Correlation between the DEN HI test and JE IgG ELISA titers. The vertical line represents a DEN HI test result of 2560. The horizontal line represents a JE IgG ELISA result of 52,000. JE IgG ELISA, Japanese encephalitis IgG indirect ELISA.
Comparison of the DEN IgG and JE IgG ELISAs
The results of both the DEN IgG and JE IgG ELISAs were linearly and positively correlated with those obtained using the DEN HI test (r = 0.528 and r = 0.565, respectively), and the observed correlations were highly significant (p < 0.001) (Table 2). The difference in the correlation coefficients between the two IgG ELISA titers 0.037 was not significant (p = 0.534). Likewise, the titers obtained using the DEN IgG and JE IgG ELISAs were significantly correlated (r = 0.665, p < 0.001) (Table 2), as shown in Figure 3 (JE IgG ELISA titer = 111,142.67 + 1.40 × DEN IgG ELISA titer). The correlation coefficients for the DEN IgG ELISA and JE IgG ELISA titers were evaluated by comparison of the numbers of negative, primary, and secondary dengue infections obtained using each of the three tests (Table 3A–C).
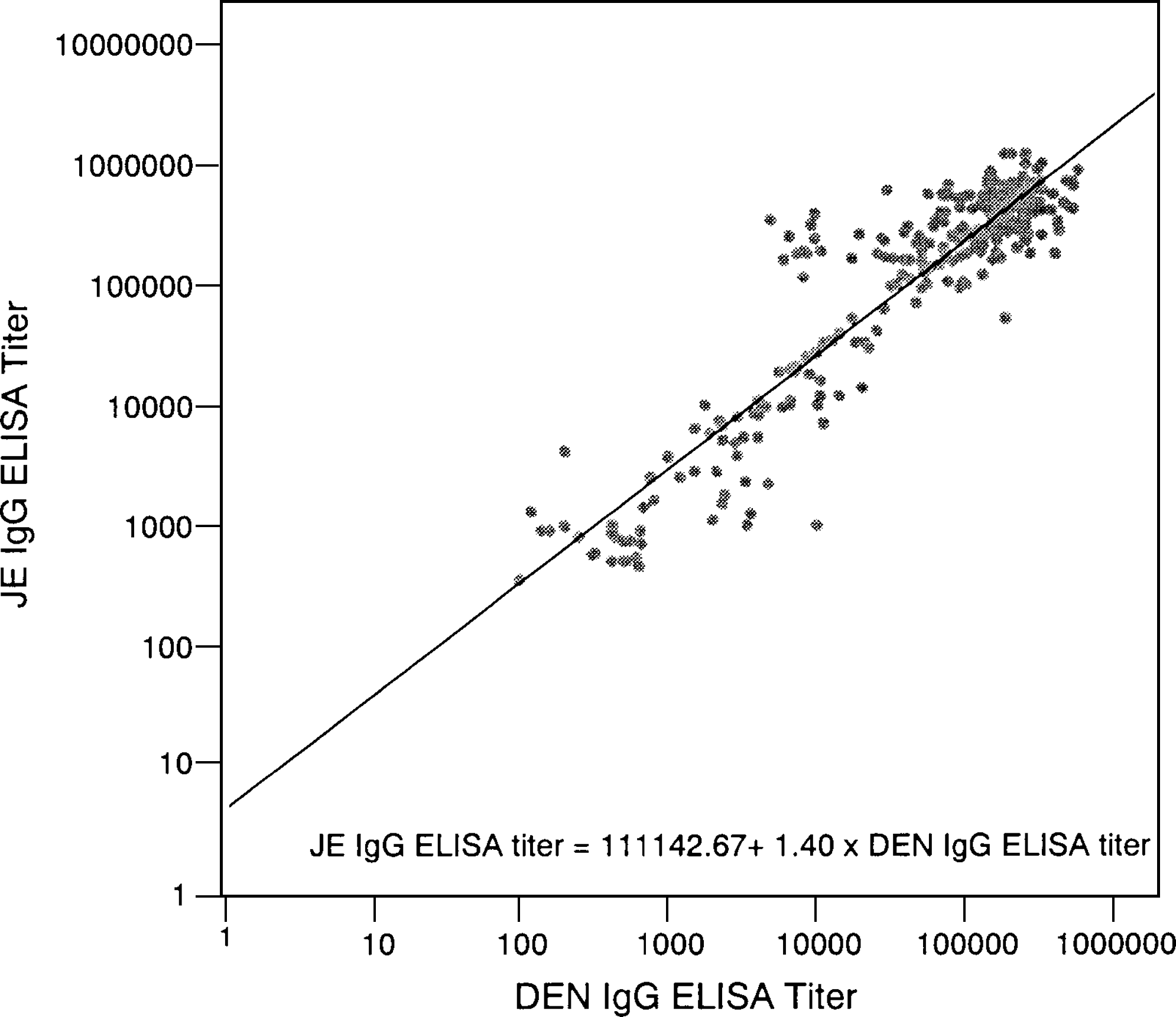
Correlation between the DEN IgG ELISA and JE IgG ELISA titers. JE IgG ELISA titer = 1,11,142.67 +1.40 × DEN IgG ELISA titer.
DEN HI, dengue hemagglutination inhibition.
Statistical Analyses of the Three Tests
The AUCs for both the DEN IgG ELISA titer and the JE IgG ELISA titer by the DEN HI test titers were analyzed (Table 4). Based on the AUC, the ability of the IgG ELISA titers to discriminate secondary dengue infection from both primary infection and dengue-negative sera was excellent. The AUCs ranged from 0.955 to 0.980 for the DEN IgG ELISA titer and from 0.940 to 0.998 for the JE IgG ELISA titer. Although the AUCs for the JE IgG ELISA were greater than those obtained for the DEN IgG ELISA, the difference between the two methods was not statistically significant (p > 0.50).
AUC, area under the ROC curve.
Discussion
This study compared the DEN IgG and JE IgG ELISAs with the DEN HI test. Currently, secondary dengue infections are diagnosed using the DEN HI test, as recommended by the WHO (1997). Although the DEN HI test gives reliable results at a lower cost, this technique has several disadvantages: serum must be collected during both the acute and convalescent phases with at least a 7-day interval between collections; pretreatment of sera with cold acetone, GRBC, and heat (56°C, 30 min) is required; preparation of antigen for each serotype and performance of separate DEN serotype-specific HI tests for each of the four serotypes is time-consuming; and serum samples must be serially diluted from 1:10 to 1:10,240. An advantage of IgG ELISA over the DEN HI test is that collection of paired serum samples and pretreatment and serial dilution of sera are not required. Moreover, at least 30 serum samples can be examined in duplicate in one 96-well microplate, whereas only 11 samples per plate can be examined with the DEN HI test for a monovalent antigen. An additional advantage of the JE IgG ELISA is that only one serotype antigen is needed, unlike the DEN IgG ELISA and the DEN HI test, which require a tetravalent antigen and four monovalent antigens, respectively. The monovalent antigen of the Japanese encephalitis virus reacts equally with IgG specific for the four dengue serotypes. By contrast, the reaction of the DEN monovalent antigen with the IgG specific for the four dengue serotypes varies among the serotypes—the reactivity with the homologous serotype is stronger than the reaction with the heterologous serotypes. Further, the Japanese encephalitis virus grows more rapidly and to greater virus titers than the dengue virus. Therefore, preparation of JE monovalent antigen is less laborious than preparation of the DEN tetravalent antigen that is required for the DEN IgG ELISA.
The results of both the DEN IgG and the JE IgG ELISAs were highly correlated with the results of the DEN HI test, which is consistent with previous reports (Lam and Devine 1998, Sang et al. 1998, Miagostovich et al. 1999, Yang et al. 2006). Both the DEN IgG and the JE IgG ELISAs may be effective for rapid evaluation of large numbers of patient serum samples, thereby increasing appropriate treatment and prevention of DHF. Titers of 1:29,000 and 1:52,000 were the cut-off values for secondary dengue infection for the DEN IgG and the JE IgG ELISAs, respectively. The slight difference in cut-off values could be due to the differences in reactivity of the two antigens (DEN and JE antigens) with anti-dengue antibodies in patient sera. Chanyasanha et al. (1984) reported that the IgG titer against the JE antigen was slightly greater than the IgG anti-DEN-1 using IgG ELISA. Yamada et al. (2003) also reported that the HI titer in the sera of dengue-infected patients was greater with use of the JE HI antigen compared with the DEN HI antigen.
However, 23 samples that were determined to be from patients with primary infections using the DEN HI test were classified as dengue-negative using the IgG ELISAs (Table 3A and B). The difference might be because the DEN HI test measures both IgM and IgG antibodies, whereas the ELISAs measure only IgG. In addition, the samples that were classified as dengue-negative based on the DEN HI test were determined to be from patients with primary infections when the IgG ELISAs were used (Table 3A and B). The discrepancies might be due to the slight difference between the empirically determined positive/negative cut-off value (1:3000) and the ideal cutoff in each ELISA. These results suggest that the ability of the IgG ELISAs to differentiate between primary dengue infection and uninfected sera might be limited. In addition, Kuno et al. (1991) reported that the DEN IgG ELISA has limited sensitivity to distinguish dengue virus infection from various flavivirus infections because of the high cross-reactivity of anti-dengue IgG with other flaviviruses. By contrast, the serological tests that selectively detect IgM, such as IgM-capture ELISAs and IgM-capture radioimmunoassays, have already been recognized as type-specific tests that can be used for the diagnosis of specific flavivirus infections, as these methods clearly differentiate various flavivirus infections (Burke and Nisalak 1982, Tardei et al. 2000, Martin et al. 2002). Therefore, the combination of a DEN IgM ELISA for the identification of dengue-positive versus dengue-negative sera and a DEN IgG ELISA (or JE IgG ELISA) for the diagnosis of secondary/primary dengue infection is recommended.
Innis et al. (1989) reported that the combination of a DEN IgM ELISA and a DEN IgG-capture ELISA effectively differentiates between primary and secondary infections, using the ratio of the results obtained with the two ELISAs. However, for the purpose of epidemiological surveillance of secondary dengue infection among confirmed dengue cases, simpler and less time-consuming tests, such as the DEN IgG ELISA or the JE IgG ELISA, are attractive alternatives.
Among dengue patients who had been vaccinated for either Japanese encephalitis and/or yellow fever, there was no cross-reactivity in the DEN IgM ELISA; however, the DEN IgG ELISA showed high cross-reactivity in these individuals (Schwartz et al. 2000, Allwinn et al. 2002, Vâzquez et al. 2003, Houghton-Triviño et al. 2008). Therefore, information regarding the patients' vaccination history is important for the diagnosis of secondary dengue infection.
In summary, the results of this study showed that the DEN IgG ELISA gives results that are highly correlated with those obtained using the DEN HI test. In particular, diagnosis of secondary dengue infection using the two methods was highly consistent. Moreover, the JE IgG ELISA could be used as an alternative to the DEN IgG ELISA for diagnosis of secondary dengue infection.
Footnotes
Acknowledgments
The authors thank Dr. I. Kurane and Dr. T. Takasaki of the Department of Virology I, National Institute of Infectious Diseases, Tokyo, Japan, for kindly providing part of the sera from the patients with primary dengue infections. The authors are very grateful to the members of the Research and Biotechnology Division, St. Luke's Medical Center, Quezon City, Philippines, to the doctors and staff at San Lazaro Hospital, Manila, Philippines, and to the members of the Department of Virology, Institute of Tropical Medicine, Nagasaki University, Nagasaki City, Japan, for their technical assistance. This study was supported by a grant-in-aid for scientific research (no. 07459098, 16406029, 18406017, B:1440619 and 21256004) from the Ministry of Education, Culture, Sports, Science, and Technology of Japan, the 21st Century Centers of Excellence Program on Global Strategies for Control of Tropical and Emerging Infectious Diseases (no. 18659131) at the Nagasaki University and a research grant from the St. Luke's Medical Center (project no. 95-001, 01-017, and 01-018).
Disclosure Statement
The authors have no competing financial interests.