
Abstract
Cat scratch disease, caused by Bartonella henselae, is a worldwide zoonosis that is most frequently associated with the bite or scratch of a kitten under 6 months of age, as well as from a fleabite. Toxoplsma gondii is also another important zoonotic agent in cats and humans, which is mainly acquired by ingestion of food or water that is contaminated with oocytes shed by cats or by eating undercooked or raw meat containing tissue cysts. Here, we report a first case of young patient with cervical lymphadenitis, which shows serological and histological evidence of B. henselae and T. gondii coinfection in Korea with literature review.
Introduction
Case Report
A 25-year-old healthy woman presented with a 10-day history of painful mass in the left neck. The physical examination showed warm, tender, and slight erythematous lymph nodes in the left submental and submandibular area of the neck, the largest measuring 2.5 cm in diameter. The lymph nodes waxed and waned twice a year for the past 3 years, being the worst event at present time. She had no history of contact with a cat, and did not recall any bite or scratch. She only had a history of working in a convenience store and eating food frequently without washing her hands. The results of routine laboratory tests, including complete blood count, blood chemistry, and liver enzyme tests, were normal. The results of the serologic evaluations for syphilis and human immunodeficiency virus and the pregnancy tests were negative. Computed tomography of the patient's neck showed multiple lymph node enlargements (maximum, 21 × 22 mm) with increased enhancement. The aforementioned largest node was sampled by excisional biopsy.
Histological evaluation of the lymph node revealed a typical triad of toxoplasmic lymphadenitis: a reactive follicular hyperplasia, clusters of epithelioid histiocytes, and reactive monocytoid B-cell proliferation (Fig. 1). The immunoglobulin M (IgM) and IgG antibodies to T. gondii were detected by microparticle enzyme immunoassay (Abbott); Toxoplasma IgM enzyme immunosorbent assay (EIA) was 5.64 index (cut-off ≥ 0.6), and IgG EIA was 292 IU/mL (cut-off ≥ 3.0).
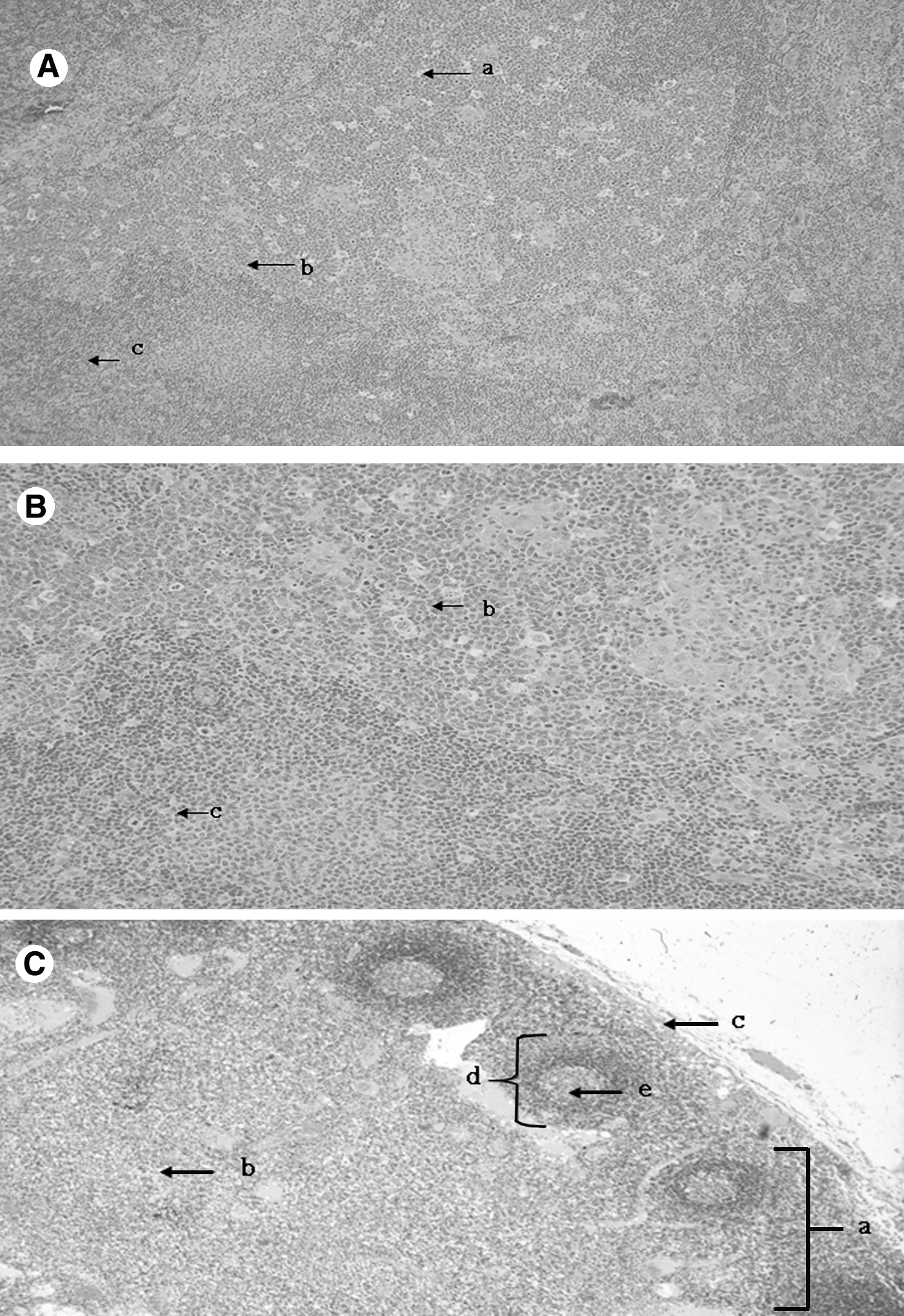
Histopathological findings in the submental lymph node. Hematoxylin and eosin stain, × 100 (
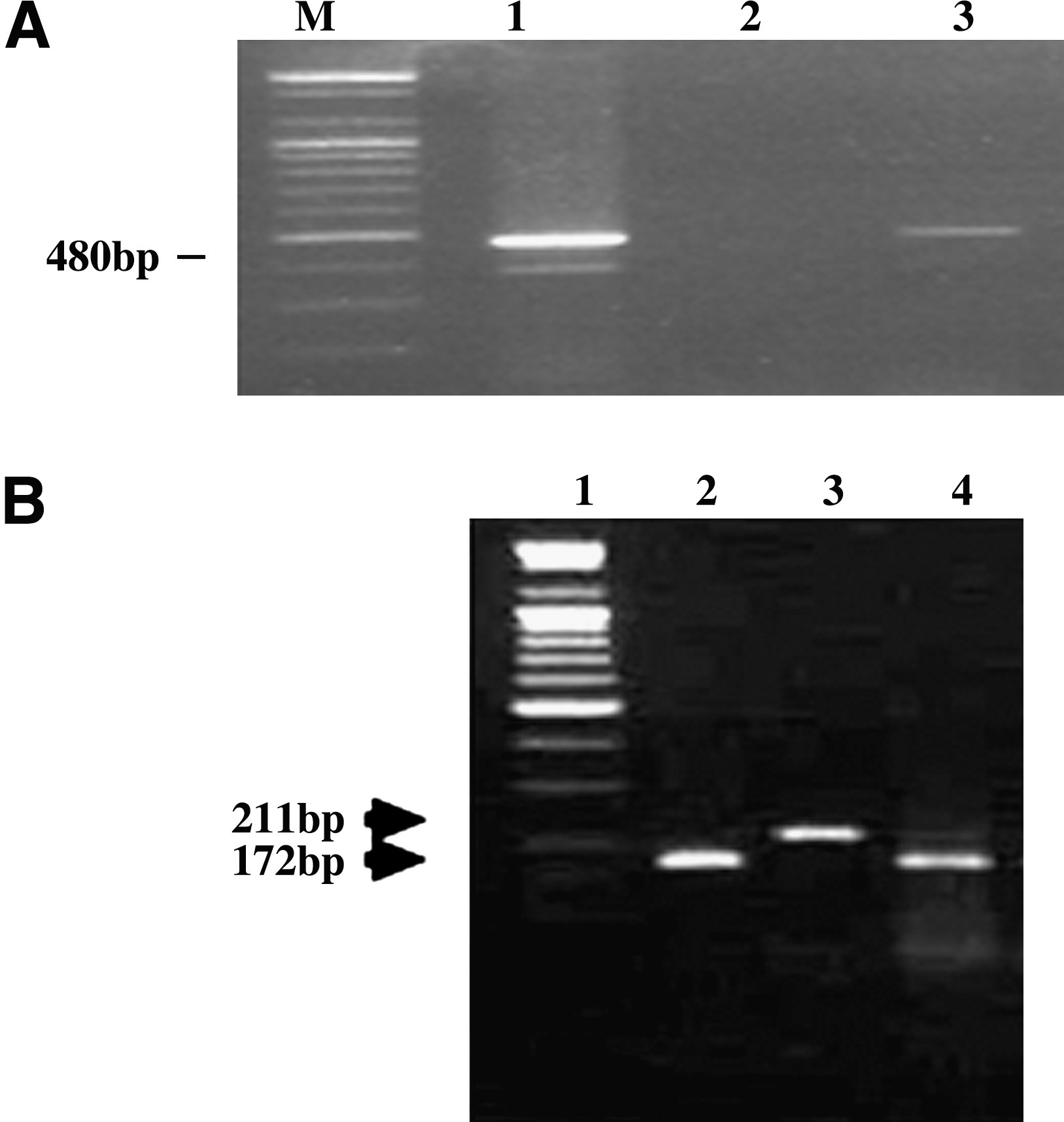
We performed the indirect immunofluorescence assay (IFA) and PCR for B. henselae, because the B. henselae and T. gondii are transmitted by a cat. The serological test was carried out with a B. henselae commercial kit (commercial Bartonella—IFA [Focus], cut-off ≥ 1:16).9 The IgM and IgG titer at first outpatient clinic visit was 1:32 and 1:128, respectively, changed to 1:16 and 1:128, one month later without treatment, suggesting acute lymphadenitis by B. henselae. We performed the examination for the serological cross-reaction, because several microbes (Mycoplasma spp. [particle agglutination test (PA); GenBio], Legionella spp. [IFA, in house], Chlamydia spp. [IFA; Focus], Borrelia spp. [IFA; Focus], Coxiella burnetii [IFA; Focus], Brucella spp. [(standard tube agglutination) STA; BD], and Francisella tularensis [(Microstandard tube agglutination test) MAT; BD]) could show cross-reaction to B. henselae. The results showed no cross-reaction. Further, we examined the citrate synthase coding gene (gltA, 480 bp) for Bartonella genus common gene PCR, and we used 16S-23S rRNA gene intergenic transcribed spacer region–based PCR for the detection of Bartonella species (B. henselae, 172 bp; B. bacilliformis, 211 bp). Genomic DNA was extracted from her serum on day 1 using the Gentra blood/tissue kit. For amplification, total 50 μL volume, including genomic DNA (2–5 μL) as a template, 0.25 U i-star Taq DNA polymerase (Intron, Seoul, Korea), 1.5 mM 10 × reaction buffer 5 μL, PCR nucleotide mix (10 mM each) 4 μL, and 10 pmol primer 1 μL, was prepared. B. henselae (ATCC49882) and B. bacilliformis (ATCC35685) DNA was used as positive controls. We selected the primer sets (BarCS-218F and BarCS-698R) for the gltA gene and the primer sets (Bar1623IF and Bar1623IR) for Bartonella species detection and subtyping (Table 1; Jensen et al. 2000). The patient's PCR product for gltA had a consistent sequence of B. hensele gltA (480 bp) (Fig. 2a). We compared the sequence of gltA with B. henselae (ACCESSION AJ439406) of GenBank. We could confirm the DNA homology (99∼100%; Fig. 3). PCR amplification of intergenic transcribed spacer region from B. henselae (ATCC49882), B. bacilliformis (ATCC35685), and patient's sample with primers Bar1623IF and Bar1623IR resulted in a single amplicon for each Bartonella species (Fig. 2b). The patient's PCR product size was identical to that of B. henselae (172 bp). However, the culture of B. henselae showed no growth. She was treated with azithromycin (500 mg/day for 1 day and 250 mg/day for 5 days) for B. henselae. Then, her lymph nodes waned, and she follows up our OPD (outpatient clinic) for 2 months with no recurrence of cervical lymphadenitis and complication after treatment.
(
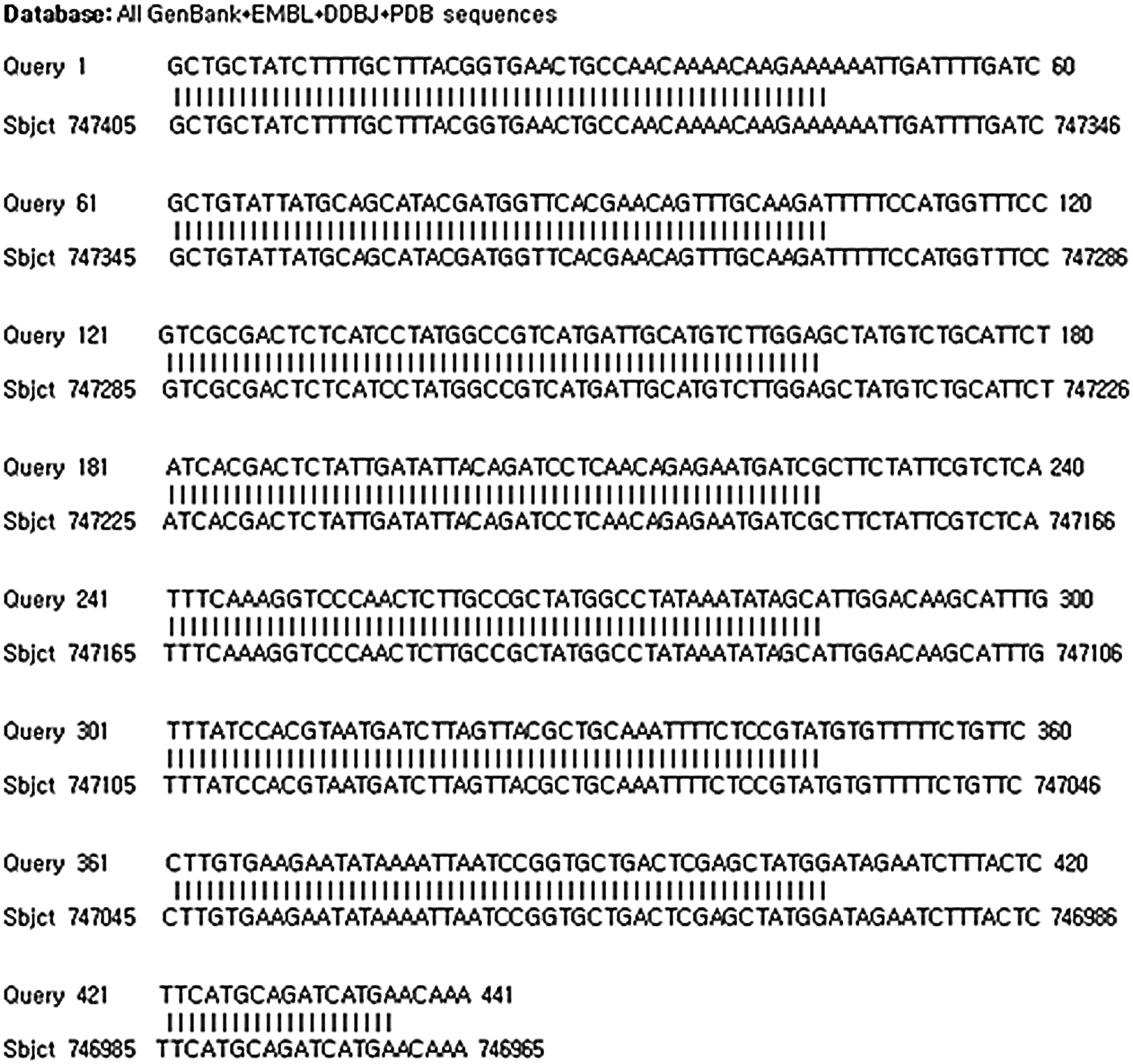
The result of GenBank DNA BLAST of B. henselae citrate synthase (gltA) gene (480 bp), partial cds (accession no. AJ439406). Features in this part of subject sequence: citrate synthase score = 815 bits (441); expect = 0.0; identities = 441/441 (100%); gaps = 0/441 (0%).
DNA
Discussion
In healthy people, infection with T. gondii leads to the production of cysts in various tissues and immunity to additional infections (Mandell et al. 2005). There is a typical triad of findings in Toxoplasma lymphadenitis: (1) a reactive follicular hyperplasia, (2) irregular clusters of epithelioid histiocytes encroaching on and blurring the margins of the germinal center, and (3) focal distension of sinuses with monocytoid cells (Negri gualdi and Negriaagualdi 1974), which were shown in our case. The tachyzoites or tissue cysts are rarely shown in Toxoplasma lymphadenitis (Negri gualdi and Negriaagualdi 1974), and our case revealed no T. gondii cysts. As the slides were already stained, we could not do the immunocytochemical staining with T. gondii antibody. There is no single serologic test that can be used to support the diagnosis of acute or chronic infection by T. gondii, but a battery of tests is required for the distinction. At present, IgG avidity test is used to differentiate the phase of infection (Jackson et al. 1993), but this test has not been commercialized yet. In our case, it is likely a more recent complication that compounded the ongoing lymphadenopathy from the result that would be more consistent with the IgM and IgG titers and the general observation that T. gondii is eventually cleared in most lymphoid sites, and is not particularly inflammatory. In addition, the patient was nonpregnant and nonimmunocompromised, so we did not treat her toxoplasmosis.
CSD generally occurs in young immunocompetent individuals like our patient. In one study, using a U.S. national database, the incidence of CSD was approximately 9 to 10 cases per 100,000 persons per year (22,000 cases per year); most cases occurred in persons less than 21 years of age (Jackson et al. 1993). The positive result of Toxoplasma infection led to the possibility of coinfection with Bartonella. In addition, the patients with no known exposure to cats will occasionally develop this disease. In this case, fleas may have also been implicated in the transmission of CSD. In a study of B. henselae antibodies in catteries, flea infestation was the risk factor most associated with high seroprevalence (Foley et al. 1998). There are no guidelines or criteria for the diagnosis of CSD. The diagnosis of CSD is based on typical clinical findings associated with probable exposure to cats. A laboratory diagnosis of CSD is most often made on the basis of a positive serologic test (IFA or EIA). Serologic testing, however, has serious shortcomings and should be used as an adjunctive test in the appropriate clinical setting. Additional laboratory testing that provides supportive data for a diagnosis of CSD includes a PCR on a tissue specimen or blood. Evaluation of peripheral blood for Bartonella DNA represents an additional, noninvasive diagnostic tool that could be useful in cases with equivocal serological results (Karim et al. 1994). Although isolation of B. henselae by culture provides a definitive diagnosis, B. henselae remains very difficult to isolate from tissue specimens. This patient, who had no history of definitely known exposure to cat, could be diagnosed by IFA and PCR. This patient was within the cut-off values for positive serology, which were ≥128 for the IgG and ≥16 for the IgM (Bergmans et al. 1997). The anti–B. henselae IgM response disappears within approximately 100 days after the onset of the symptoms (Bergmans et al. 1997), explaining the IgM serology change of this patient, whose IgM titer was decreased from 1:32 to 1:16 one month later. However, there is a possibility that this change in IgM IFA titer is within the variability of the assay. The IgG response, if present, generally appears later and remains elevated during a longer period (Bergmans et al. 1997). It is speculated that because she was in early infection period, the IgG remained unchanged (1:128). Unfortunately, since this patient refused to have more blood test anymore, we could not follow-up a change of titer. The culture of B. henselae showed no growth. It may be because that she had taken Clarithromycin before our outpatient clinic visit. CSD is rare for more serious signs to develop in healthy people and mostly recover without treatment over a 3-week period. Doxycycline, erythromycin, or rifampicin are the antibiotics of choice in humans, but the course of the disease can also be shortened using azithromycin, ciprofloxacin, trimethoprim/sulfamethoxazole, or clarithromycin (Karim et al. 1994). We used azithromycin, and the result was successful. To our knowledge, this is the third case report on a patient with a regional lymphadenitis with serologic and histologic evidence of toxoplasmosis and CSD, in the world, and the first case in Korea. The two cases, which were acute coinfection, were from Germany in 1974 and 2002, respectively (Arvand et al. 2002). The study of seroprevalence of B. henselae and T. gondii among 163 healthy individuals in Thailand was conducted between 1997 and 1998, showing B. henselae IgG 9 (5.5%), B. henselae IgM 5 (3.1%), and T. gondii antibody 5 (3.1%), but there was no report of overlapping infection by T. gondii and B. henselae (Maruyama et al. 2000). Unfortunately, there is no epidemiologic study of CSD or Toxoplasmosis in Korea as yet. This case described here raises an important issue with regard to the diagnostic approach of patients with cervical lymphadenitis. As the cat owners are increased nowadays, also in Korea, when a patient is presented with lymphadenitis, the physicians should inquire recent cat contact and/or scratch, and should consider routine evaluation of T. gondii irrespective of whether the patient had a contact with a cat or not, because the patient can catch a disease accidentally. Then, if the result of IgG and/or IgM of T. gondii is positive and acute symptom is revealed, physicians have to consider overlapping infection of B. henselae. Additional researches of epidemiology and clinical studies are required to find out the prevalence of Toxoplasma and Bartonella infection, and to construct a proper diagnostic diagram of cervical lymphadenitis.
Footnotes
Disclosure Statement
No competing financial interests exist.