
Abstract
Background:
Eastern equine encephalitis (EEE) is one of the most severe arboviral encephalitides in North America. Before 2009, limited nonhuman EEE virus activity had been reported in Maine, all from the southernmost area of the state. No human case has been reported in a Maine resident.
Methods:
We review all EEE virus activity reported to Maine Centers for Disease Control in 2009 and describe current testing practices for possible human EEE cases.
Results:
In 2009, fatal cases of EEE were identified in 15 horses, 1 llama, and 3 flocks of pheasants in Maine, with activity extending into the central part of the state. Although no human EEE cases were identified, diagnostic testing practices of most meningitis and encephalitis cases were inadequate to exclude EEE.
Conclusions:
Work to better define the expanding range of EEE virus in Maine is warranted, along with education of healthcare providers regarding appropriate testing for this serious disease.
Introduction
Maine is a large, predominantly rural state with ecosystems that could sustain EEEV transmission. To date, no human EEE cases have been reported in a Maine resident, although in 2008, a visitor to Maine died from EEE. From 2001 to 2008, 3 EEE equine cases, 13 EEEV-infected birds, and 2 EEEV-positive mosquito pools were reported in Maine; all occurred in York and Cumberland Counties. We summarize the increased and expanded EEEV activity that occurred in Maine in 2009, describe current testing practices for possible human EEE cases, and make recommendations for identifying future EEE cases.
We identified all EEE activity reported to Maine CDC in 2009, and conducted active surveillance for human disease. Human arboviral encephalitis is a nationally notifiable condition and is reportable in Maine. Reporting of nonhuman EEEV activity is passive and voluntary. Suspected animal cases are reported to the state veterinarian and are tested for rabies before being tested for EEEV. Routine mosquito-based surveillance occurs in York and Cumberland counties from June to September.
A possible human EEE case was defined as a patient hospitalized in Maine from July–September 2009 with unexplained acute meningitis or encephalitis (i.e., acute onset of fever with meningismus, mental status changes, seizures, or cerebrospinal fluid [CSF] white blood cells ≥6 cells/mm3). We identified possible cases by searching international classification of diseases (ICD)-9 discharge codes * at Maine's four largest hospitals and CSF specimens submitted to five laboratories for diagnostic testing for herpes simplex virus, enterovirus, West Nile virus, or EEEV. The study hospitals have a statewide catchment area. Patients <1 month of age were excluded. We reviewed medical records to confirm the clinical syndrome and excluded patients with defined etiologies. Negative test results for anti-EEEV immunoglobulin M (IgM) antibodies were considered adequate to exclude EEEV infection if the sample was collected >7 days after illness onset. This investigation was determined to be a public health response activity and did not require review by the state or CDC institutional review boards.
From August–October 2009, fatal cases of EEE were identified among 15 horses, 1 llama, and 3 pheasant flocks in Maine. Five counties were affected, extending into central Maine (Fig. 1). In addition, EEEV was detected in two pools of Cs. melanura collected in York County. None of the horses had completed the recommended vaccination course (Wilson et al. 1995).
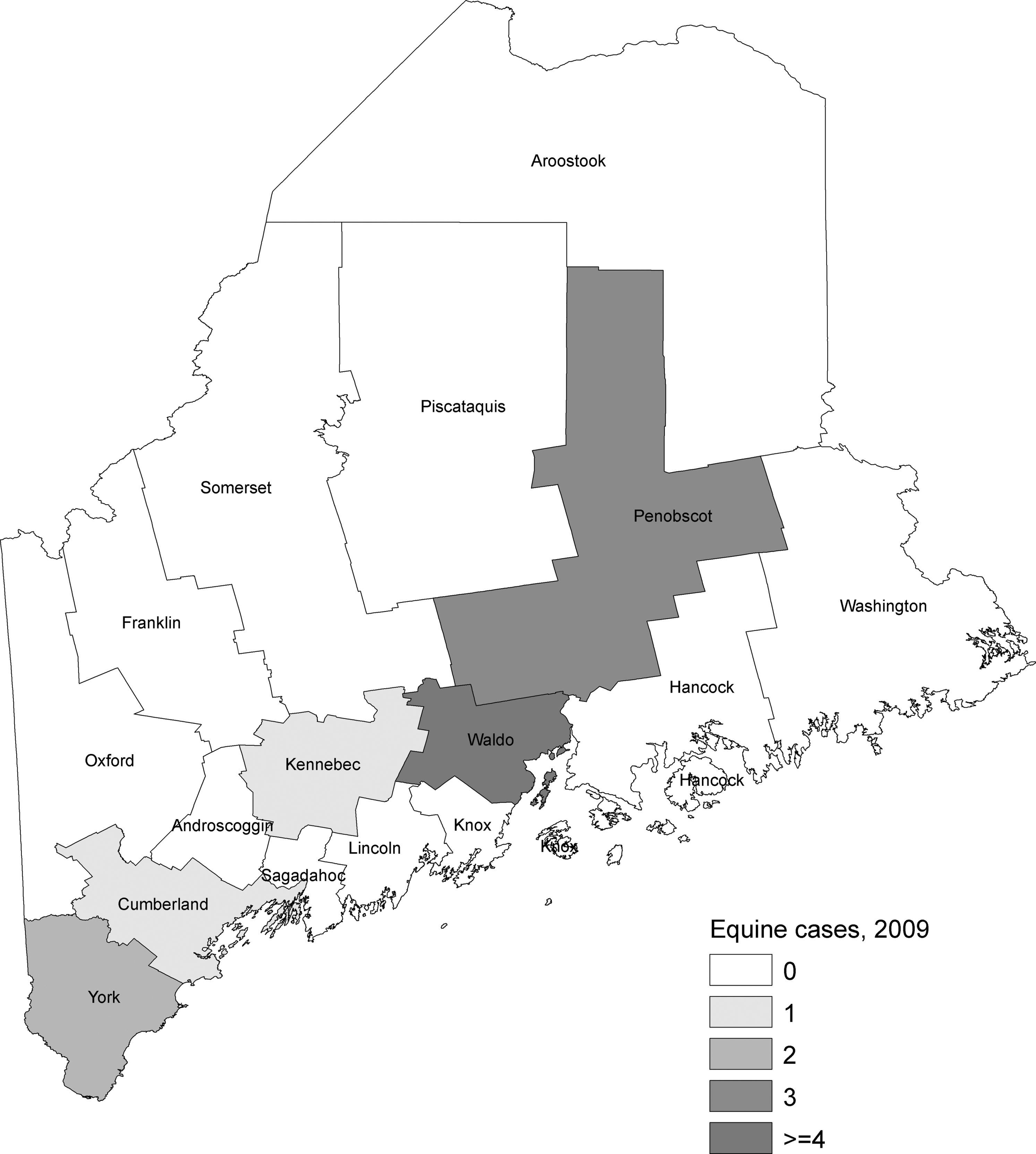
Eastern equine encephalitis cases in horses, Maine, 2009. In 2009, eastern equine encephalitis virus infection also was detected in three pheasant flocks, one llama, and two mosquito pools, all in York County.
No human cases of EEE were reported in Maine in 2009. We identified 30 possible EEE cases admitted to four Maine hospitals from July 1 to September 30; 26 (87%) were identified through laboratory records, 1 (3%) by ICD-9 code search, and 3 (10%) by both methods. Anti-EEEV IgM testing was performed on 7 (23%) possible EEE cases, and only 3 (10%) had specimens that were adequate to exclude EEEV infection. All EEEV tests were negative.
Of the 27 patients for whom EEE could not be ruled out, 14 (52%) were women and the median age was 37 years (range: 1 month–80 years). Seventeen (63%) patients resided in a county that reported nonhuman EEEV activity in 2009. The median hospital stay was 4 days (range: 1–35 days). Five (19%) were admitted to the intensive care unit; one (4%) patient died. Only 5 (19%) of the 27 patients were tested for West Nile virus; all specimens were collected ≤7 days after symptom onset and all tested negative.
Increased and more widespread EEEV activity was reported in Maine in 2009, possibly indicating expansion of the range of this virus. Human EEE cases have been reported in the neighboring states of New Hampshire and Massachusetts. EEEV activity also has been detected in eastern Canada, suggesting that the EEEV enzootic cycle can likely be sustained throughout Maine (Calisher 1994).
While no human EEE cases were identified, nonhuman EEEV activity indicates potential risk to humans. In addition to the high case fatality rate, the neurologic sequelae associated with EEE disease has been estimated to cost $3 million per patient (Villari et al. 1995). Therefore, even a small number of EEE cases could have a substantial economic and public health impact.
Our investigation identified that diagnostic testing practices were inadequate to exclude EEEV infection in 90% of possible EEE cases either because testing was not requested or it was conducted too early in the illness. EEE disease should be considered in all patients hospitalized with unexplained meningitis or encephalitis in an endemic area during the arboviral season. EEEV is rarely isolated from blood or CSF, and anti-EEEV IgM may not be detectable during the first week of illness (Feemster 1938, Morse et al. 1992). Submission of a convalescent serum specimen for EEEV testing should be considered if the initial sample was collected ≤7 days after illness onset and the diagnosis remains uncertain.
Our investigation was subject to several limitations. We did not survey all hospitals and laboratories in Maine or investigate unexplained deaths; therefore, we likely missed some possible EEE cases. In addition, patients with alternate clinical diagnoses made after hospital discharge may have been misclassified as possible EEE. Compared to published descriptions of confirmed EEE cases, the 27 possible cases identified in Maine had shorter hospital admissions and a lower case fatality rate (Feemster 1938, Ayres and Feemster 1949, Deresiewicz et al. 1997), suggesting that most of these patients likely did not have EEE. However, convalescent serum specimens, which could have been tested to determine if any of the possible cases had EEE, were not obtained.
Activities to further define the geographic range and extent of EEEV activity in Maine could include expanded surveillance of mosquitoes or sentinel animals. To prevent equine cases, horses in Maine should receive EEE vaccine (Wilson et al. 1995). When EEEV activity is identified, active surveillance for human cases should be considered, including appropriate collection and testing of convalescent samples. Finally, efforts should be made to improve testing practices among healthcare providers and increase public awareness regarding EEE.
Footnotes
Acknowledgments
The authors thank the following people for assistance with data collection: Betty Wagner at Maine Medical Center, Portland; Don Piper at NorDx laboratory, Portland; Daniela Skalina, Peggy Noddin, and Matt Twomey at Central Maine Medical Center, Lewiston; Anne Paradis and Judy Clukey at MaineGeneral Medical Center, Waterville; Donna Dunton at Eastern Maine Medical Center, Bangor; and Liz Stevens and Kirk Doing at ALI laboratory, Bangor. We thank Andrew Pelletier and Erin Staples for assistance with study organization and manuscript preparation; Nicole Lindsey for assistance with mapping; and Peggy Collins for database assistance.
Disclosure Statement
No competing financial interests exist.
*
The following ICD-9 discharge diagnosis codes were used in the search: 062, mosquite-borne viral encephalitis; 063, tick-borne viral encephalitis; 064, viral encephalitis transmitted by other and unspecified arthropods; 066, other arthropod-borne viral diseases; 088.1, arthropod-borne disease unspecified; 321.2, meningitis due to viruses not elsewhere classified; 321.8, meningitis due to other nonbacterial organisms classified elsewhere; 322, meningitis of unspecified cause; 323.0, encephalitis in virus diseases classified elsewhere; 323.4, other encephalitis due to infection classified elsewhere; 323.8, other causes of encephalitis, myelitis, and encephalomyelitis; 323.9, unspecified cause of encephalitis.