
Abstract
Thirteen Trypanosoma cruzi isolates from different geographic regions of Mexico and Guatemala belonging to discrete typing unit (DTU) I and a reference CL-Brener (DTU VI) strain were used to perform enzyme-linked immunosorbent assay (ELISA) and polymerase chain reaction (PCR). A panel of 57 Mexican serum samples of patients with chronic chagasic cardiopathy and asymptomatic infected subjects (blood bank donors) were used in this study. DNA from the above 14 T. cruzi strains were extracted and analyzed by PCR using different sets of primers designed from minicircle and satellite T. cruzi DNA. The chronic chagasic cardiopathy serum samples were easily recognized with ELISA regardless of the source of antigenic extract used, even with the CL-Brener TcVI, but positive serum samples from blood bank donors in some cases were not recognized by some Mexican antigenic extracts. On the other hand, PCR showed an excellent performance despite the set of primers used, since all Mexican and Guatemalan T. cruzi strains were correctly amplified. In general terms, Mexican, Guatemalan, and CL-Brener T. cruzi strains are equally good sources of antigen when using the ELISA test to detect Mexican serum samples. However, there are some strains with poor performance. The DTU I strains are easily detected using either kinetoplast or satellite DNA target designed from DTU VI strains.
Introduction
T. cruzi has been genotypically divided into six intra-species lineages (discrete typing unit [DTU]), recently renamed TcI–VI (Zingales et al. 2009). The geographical distribution of the DTUs is complex. TcI is found as far north as the United States; in contrast, TcII, V, and VI predominate in the southern cone countries. In addition, this genetic heterogeneity has a consequence on the biologic features of the parasite, influencing the clinical outcome and immune responses (Souto et al. 1996, Briones et al. 1999, Zambrano et al. 2002). Likely, these factors may contribute to inconclusive results obtained in serodiagnosis, even with standardized tests (Modolo et al. 2007, Furuchu et al. 2008).
Since, there is no gold standard for diagnosis of the chronic stage of Chagas disease, an alternative method, such as the highly specific polymerase chain reaction (PCR) technique, has been introduced. However, a large variation in sensitivity has also been reported in patients with chronic disease (Moser et al. 1989, Britto et al. 1995, Junqueira et al. 1996, Monteón et al. 1996). As mentioned above, genetic strain differences may influence biological characteristics, such as parasitemia, and consequently PCR sensitivity, but other factors may contribute to the overall performance of PCR assays: the epidemiological characteristics of the study populations, the collected blood volume, the method used to isolate DNA, and parasite target-sequence (Carvalho 2009).
With regard to parasite target-sequence, the most used currently are those designed from nuclear DNA satellite (a highly repeat sequence) and from conserved domains of minicircle kinetoplast DNA. However, it has been shown that nucleotide polymorphism does exist among clones and strains of T. cruzi for these targets (Moser et al. 1989). This reason opened doubts about the performance of primers and their targets. In the work published by Virreira et al. (2003), a comparison of PCR using different set of primers was performed. They compared primers set S35/S36 and 121/122 for conserved domains of kinetoplast minicircle and set primers Tcz1/Tcz2 and Dias1/Dias2 for the 195-bp satellite repeat. They found that primer set Tcz1/Tcz2 showed the best sensitivity even with diverse DTU strains.
Mexico is the most northern country in America in which T. cruzi infection is endemic and there is not vector control program. The main DTU identified in infected people is TcI (Bosseno et al. 2002, Ruíz-Sánchez et al. 2005). Here we compared a collection of Mexican and Guatemalan DTU TcI strains of T. cruzi as a source of antigen in the performance of serological ELISA; we also evaluated the most common set of primers used in PCR assays designed from satellite and kinetoplast minicircle DNA sequences of T. cruzi. It is known that the currently used sets of primers for the PCR technique are usually derived from strains or clones isolated in the southern-cone countries of America; these isolates belong to DTU TcII–TcVI. To our knowledge, this is the first report in which Mexican and Guatemalan strains have been evaluated in the performance of ELISA and PCR assay.
Materials and Methods
Serum samples
We used 17 serum samples from chronic chagasic cardiopathy (CCC) patients, who are medically cared for at the Instittuto Nacional de Cardiología “I. Chávez.” This group of CCC patients had clinical evaluation, ECG, chest X-ray, echocardiogram tests, and two serological positive tests; 40 sera from seropositive blood donors with two serologically positive samples from the Blood Bank of the same institution were also included.
Antigen preparation for ELISA
Thirteen T. cruzi isolated from diverse geographic zones of Mexico and Guatemala (Table 1) and the reference CL-Brener strain were cultured in liquid infusion tryptose (LIT) medium.
Trypanosoma cruzi was isolated and maintained in liquid infusion tryptose (LIT) medium, and the genotyping was performed with miniexon method.
CCC, chronic chagasic cardiopathy; DTU, discrete typing unit.
At the logarithmic growth phase, parasites were harvested by centrifugation at 1500 g for 20 min. Pellets were washed three times with PBS. After the last washing, each pellet was added with 5 mL of PBS in the presence of protease inhibitors (5 mM PMSF, 2 mM EDTA, and 1 mM TLCK). The suspension was sonicated for six to eight cycles at 100 W/10 s with 1 min intervals. After that, the sonicated material was centrifuged at 15,000 g for 30 min at 4°C. Protein concentration was determined in the recovered supernatant and kept at −70°C until used.
Serological test
A homemade ELISA-standardized technique was used. In brief, a polystyrene plate (Nunc Polysorb Plates) was coated with 10 μg/mL of crude extract protein of each T. cruzi isolate or strain in alkaline-buffered solution. Human serum diluted at 1:400 and anti-human IgG-peroxidase conjugate at 1:15,000 dilution were used (Zymed Lab). The reaction was revealed by addition of O-phenilen-diamine and read at 490 nm in an automatic ELISA reader (Biorad).
The cut-off value was set as follows: sera from 30 healthy volunteers previously tested as negatives for anti–T. cruzi antibodies were analyzed for their distribution. The mean optical density (OD) of seronegative healthy individuals plus three standard deviations (SD) was fixed to set the cut-off. All healthy seronegative individuals had values classified as negative after the cut-off value was set (mean+3SD).
DNA extraction for PCR
Culture of the 14 strains of T. cruzi was carried out as mentioned above. The pellet obtained after the last washing was diluted in 500 μL of PBS, and the DNA was extracted twice with a mixture of phenol, chloroform, and isoamylic alcohol (25:24:1). The nucleic acids were precipitated by the addition of 1/10 of a volume of 3 M sodium acetate (pH 5.5) and 2 volumes of ethanol. After centrifugation for 15 min, the pellet was rinsed with 70% ethanol, air-dried, and suspended in 50 μL of water and kept at −70°C until use.
PCR for T. cruzi
Amplification reaction was performed in 50 μL volume containing 1 μL of DNA sample (10 ng) and 10 μM of each primer. We compared two sets of primers designed from minicircle kinetoplast DNA: one set of primers 121 (5′-AAATAATGTACGGGTGAGATGCATGA-3′) and 122 (5′-GGTTCGATTGGGGTTGGTGTAATATA-3′) (Degrave et al. 1988) that generates an amplicon of 330 bp, and the other set of KNS1 (5′-GGGGTTCGATTGGGGTTGGTGTA-3′) and KNS2 (5′-AAA(G/T)TTGAACGCCCCTCCCAA-3′) (Monteón et al. 1994) that produces an amplicon of 300 bp.
One set of primers was designed from satellite DNA, TCZ1 (5′-CGAGCTCTTGCCCACACGGGTGCT-3′) and TCZ2 (5′-CCTCCAAGCAGCGGATAGTTCAGG-3′) (Moser et al. 1989), that produces an amplicon of 188 bp.
To each reaction, we added 0.2 mM of each dNTPs, and 2.5 U of Taq polymerase (Invitrogen), 10 mM Tris-HCl, pH 8.8, 50 mM KCl, and 1.5 mM MgCl. The reaction was subjected to 35 cycles: 94°C for 1 min, annealing temperature was 64°C for primers 121/122, 56°C for primers KNS1/KNS2, and 55°C for TCZ1/TCZ2 for 45 s, and 72°C for 1 min. The amplified product was subjected to a 2% agarose gel electrophoresis and observed after ethidium bromide staining under UV exposure. Positive and negative controls were always included.
Positive samples generated a 330 bp product for 121/122; 300 bp for KNS1/KNS2; and 188 bp for TCZ1/TCZ2.
Statistical analysis
The descriptive section consisted of determination of the mean, SD, and percentage. The analysis of variance test was used for comparison purposes among groups (p<0.05 for statistical significance). GraphPad Prism 4 software was used for these analyses.
Results
The Mexican T. cruzi were isolates from western, central, and southern Mexico; those from Guatemala were from the central and eastern part of the country. All of them were isolated from human cases and classified as TcI using miniexon genotyping method (Ruíz-Sánchez et al. 2005) (Table 1).
In the ELISA analysis, two main groups could be distinguished. One included serum samples of CCC patients that were easily recognized as positive with any T. cruzi-TcI extract used; even with CL-Brener-TcVI extract. However, the intensity of the reaction (OD) depended on which T. cruzi antigen was used. For example, in one of the Guatemalan isolates (H038) the intensity of the reaction was stronger, an intermediate intensity reaction was observed with INC-5 from Mexico and lower intensity with CL-Brener from Brazil (Figs. 1 and 2), but there was no clear association according to the geographical origin of the strains.
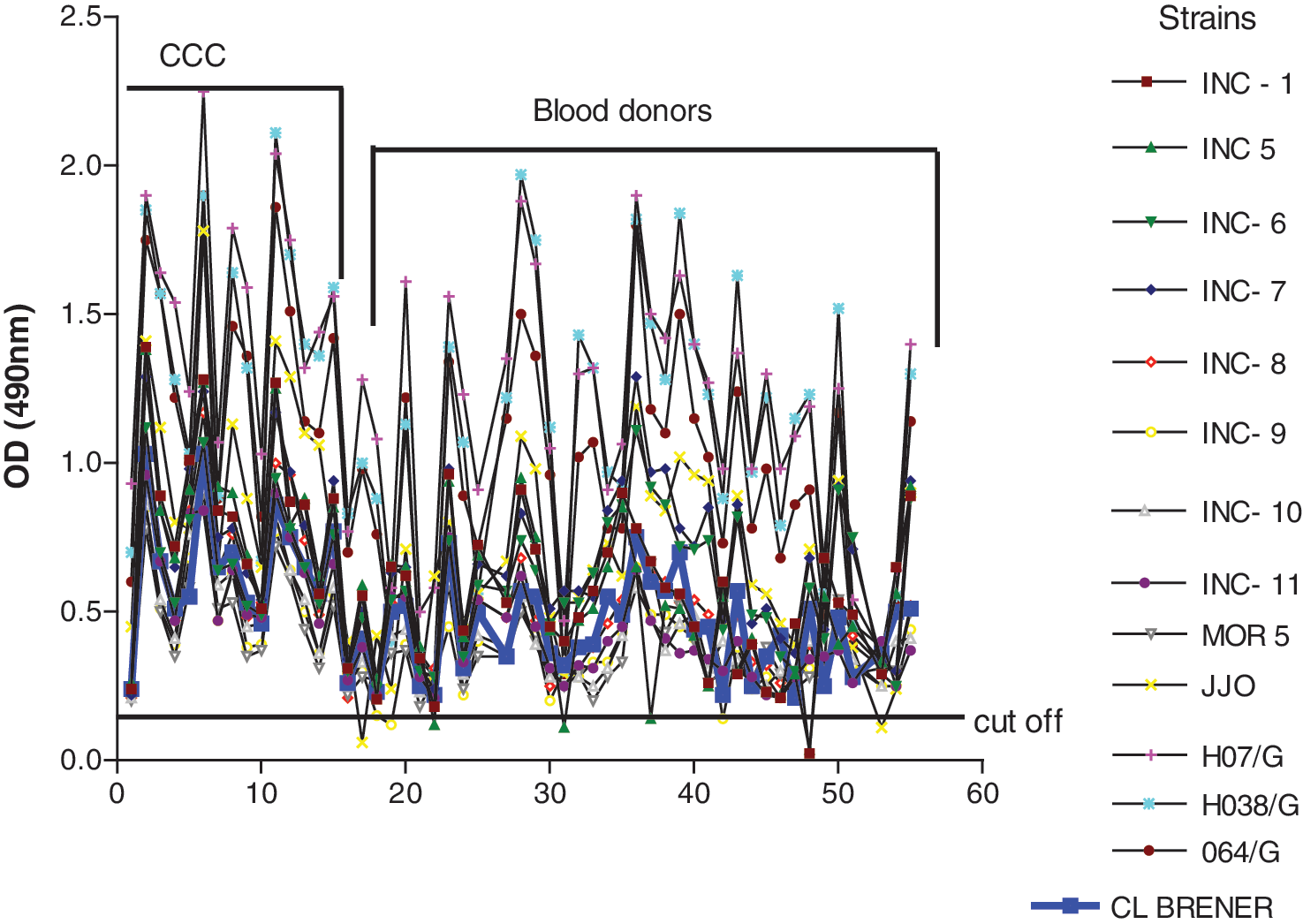
Thirteen antigenic extracts of Trypanosoma cruzi isolated from diverse geographic zones of Mexico and Guatemala were evaluated in enzyme-linked immunosorbent assay (ELISA) with Mexican sera sample of chronic chagasic patients (sample number 1–17) and seropositive and blood donor (sample number 18–57). Extract CL-Brener is depicted in blue. Cut-off is the mean optical density (OD) of 30 seronegative healthy individuals plus three standard deviations. (X axis: sample number.)
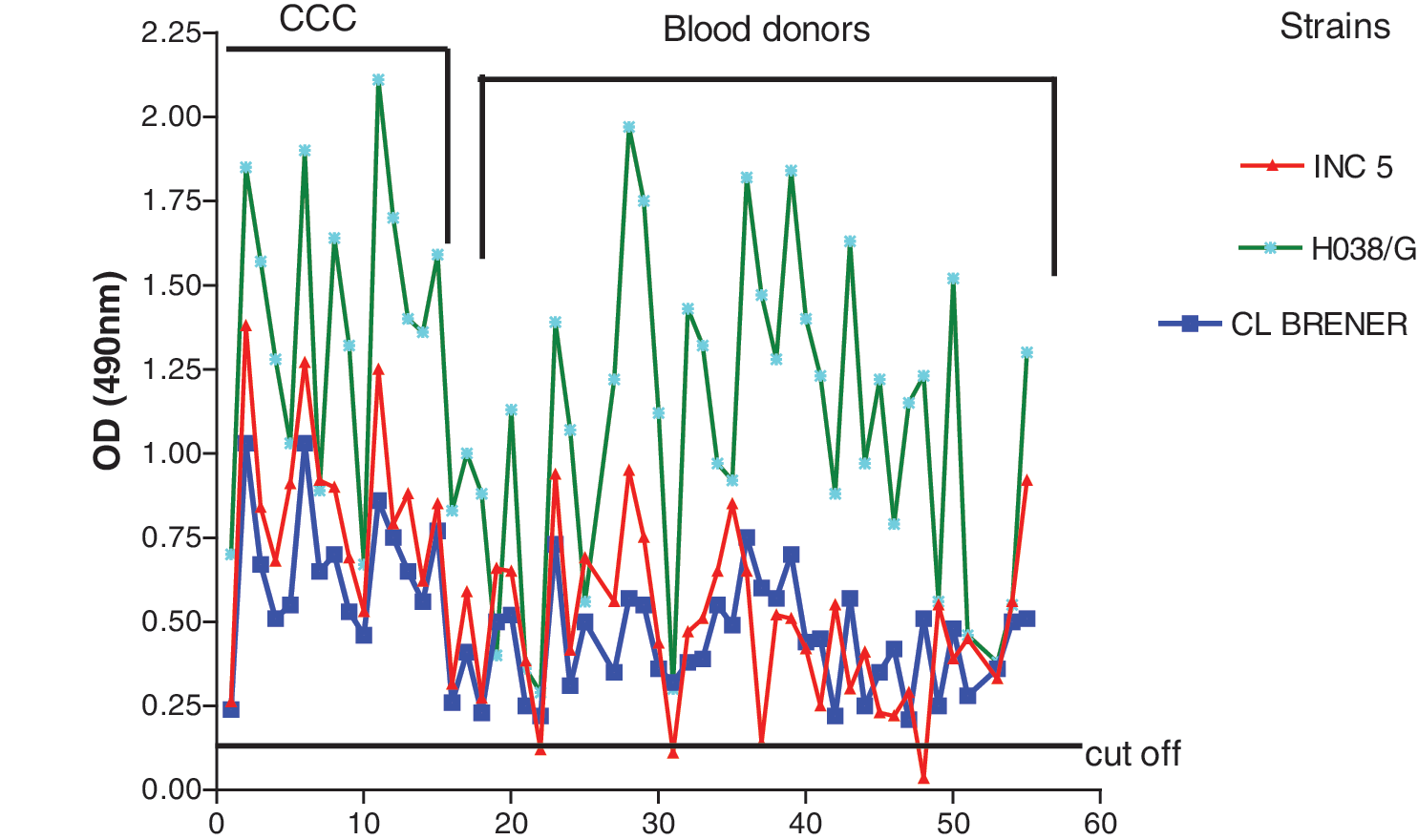
Three representative antigenic extracts of T. cruzi. The INC-5 extract with the worst performance, H038/G with the best performance, and the CL-Brener were evaluated in ELISA with Mexican sera sample of chronic chagasic patients (sample numbers 1–17) and seropositive and blood donor (sample numbers 18–57). Cut-off is the mean OD of 30 seronegative healthy individuals plus 3 standard deviations.
The second group (sera from blood donors) had a different reactivity pattern.
Some antigenic extracts were unable to recognize several samples as positive as done by the rest of extracts. This was the case for INC-1 (from Oaxaca, Mexico), INC-5 (from Guanajuato, Mexico), INC-11 (from Hidalgo, Mexico), JJO (form Jalisco, Mexico), and H07 (from Guatemala) antigenic extracts, which failed to identify between 1 or 2 of the positive sera out of the forty in the panel, that represents 2.5% to 5% (Fig. 1). The worst extract corresponded to INC-5 from Guanajuato, Mexico, which failed to identify four positive sera that represent 10%. In contrast, there were some antigenic extracts that presented higher OD values, such as H07, H038, and H064 from Guatemala, than the rest (Fig. 1). In the case of CL-Brener TcVI extract in spite of lower intensity reaction in comparison to other TcI extracts, it was able to recognize all positive sera correctly.
In Figure 2, we present the results of three representative strains. Two of them belong to TcI and the other to TcVI. The H038 from Guatemala showed the stronger intensity of reaction with both serum panels in contrast to INC-5 from central part of Mexico that showed erratic behavior, in view of the fact that this extract fail to detect four positive sera. However, the CL-Brener strain that belong to TcVI was able to recognize all samples as positive as done the rest of extracts that belong to TcI.
In the panel of blood bank donors, there were samples from diverse geographic origin. The 69% came from central part of Mexico, 7% from States localized at the Gulf of Mexico, and 24% from States localized at the Pacific coast.
The performance of the PCR assay was evaluated using DNA of T. cruzi that belonged to DTU I from Mexico and Guatemala; in addition, we evaluated different sets of primers designed from kinetoplast or satellite DNA. As shown in Figure 3A–C, the PCR assay was positive independently from the T. cruzi strain or set of primers used. In the case of primers 121/122, an extra band (>900 bp) was observed, but this set of primers produced a clear specific band corresponding to 330 bp. The TCZ primers produced a very clear specific band, but some smears appeared in many cases. The primers KNS1/KNS2 generated less intense band amplification; however, all T. cruzi DNA samples were identified as positive.
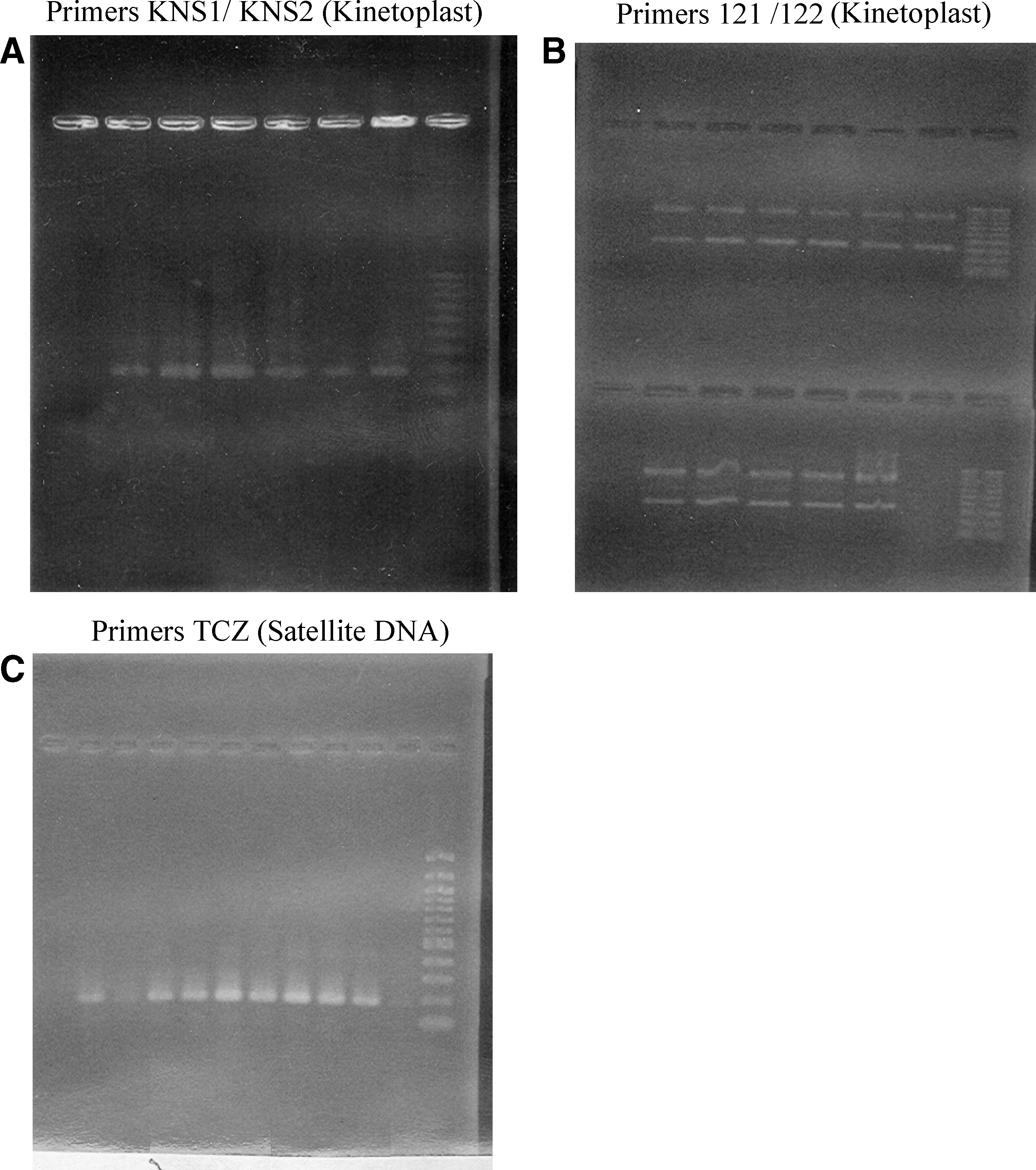
Representative images of polymerase chain reaction products using different sets of primers with DNA samples of discrete typing unit (DTU) 1 of T. cruzi. Primers KNS1/KNS2 (Kinetoplast)
Discussion
Diagnosis of chronic Chagas disease is based on serological tests, given that parasitemia is very scarce at this stage of the infection. In addition, variability among T. cruzi isolates in conjunction with the immunogenetic features of the human host may influence the performance of serological tests (Gomes et al. 2009).
Variability in the performance of serological tests has been observed using crude extracts, or even recombinant proteins using sera from South and Central America (Umezawa et al. 1999). Mexico is the most northern country in the American continent in which T. cruzi infection is endemic; there is limited information on this issue, but a recently published work reported an excellent performance of serodiagnosis using Mexican serum samples in four laboratories in South and Central America and Mexico (Luquetti et al. 2009).
In this work, we extended previous observations, evaluating now different antigen extracts from Mexican and Guatemalan T. cruzi isolates, all of them classified as DTU I (Ruíz-Sánchez et al. 2005).
Our data show that, in ELISA, independently from the T. cruzi extract used as source of antigen, samples from CCC patients are always identified correctly as positive, which suggests that CCC serum samples react to immunodominant antigens present in all T. cruzi organisms, although with some extracts, specially from Guatemala, the intensity of the reaction was stronger (OD above 1.0). This finding could suggest that Guatemalan strains are richer in these immunodominant antigens, but this assumption needs to be evaluated.
Another finding was the heterogeneous reaction of particular serum samples against different antigenic extracts; this feature could be because antigenic extracts are complex in nature with qualitative and quantitative differences in components among T. cruzi isolates (Figs. 1 and 2).
A very important issue in our data is differences between TcVI extract from CL-Brener strain and TcI extracts. Many commercial antibody tests use antigen, recombinant or crude, from TcVI; these commercial tests are used in Northern Latin America countries such as Mexico and Guatemala, where this lineage is largely absent. However, CL-Brener extract was able to recognize all positive sera as done the rest of extracts that belong to TcI, but the intensity of reaction was lower.
When we tested blood bank seropositive donors, some antigenic extracts failed to detect some positive samples. Among bad extracts we found INC-1, INC-11, and JJO isolated from Oaxaca (Pacific coast), Hidalgo (central part of Mexico), and Jalisco (western part of Mexico), respectively, but the worst extract was INC-5 isolated from Guanajuato State. This may suggest that to reach the highest sensitivity in the screening test, such as ELISA, it is necessary to have the most complex antigenic extract as possible. Although in our panel there were sera from different geographic origin (Central part of Mexico, Pacific coast and Gulf of Mexico). It might be of interest to analyze a number of serum samples from blood bank donors representative of each region, with the intention of suggest the best antigenic extract, even so from our data we may suggest that in general terms any strain may be useful to prepare antigen for serological test. However, it would be recommended to include at least one autochthonous strain to improve the antigenic extract.
Other factor that may influence the results obtained from blood bank donors is quality sample, sample storage, and sample age. To minimize the influence of these factors, we made several aliquots for each one serum samples with the intention of avoid repeated thawed and freeze. However, we cannot rule out that in a given serum with low antibody titer, the reactivity could be lost. But even in this case, we could expect that the reactivity could be lost to more extracts, but this did not happen.
In the PCR assay, the use of kinetoplast minicircle primers and satellite DNA primers were convenient tools to recognize Mexican and Guatemalan T. cruzi parasites, although the above primers were originally designed from T. cruzi DTU different from the Mexican and Guatemalan DTU. Recently, several articles have been published on molecular identification of T. cruzi in human specimens using PCR; for example, del Puerto et al. in 2010 found differences when they used kDNA and satellite DNA set primers to detect parasite DNA in biological Bolivian sample: lower sensitivity was obtained with kDNA set primer. Colombia Ramirez et al. in 2009 found that in biological samples using different set of primers, similar results were obtained, where kDNA set of primers showed lower sensitivity than nuclear repetitive region. These data suggest that behavior of performance of PCR depend on nature of biological sample and set of primers used; however, when we use parasite DNA such as in our work, these factors do not influence the performance of PCR.
In conclusion, Mexican and Guatemalan T. cruzi strains may be excellent choices to prepare or obtain antigenic extracts to detect CCC patients, but especially care should be taken when using blood bank samples, since some antigenic extracts fail to recognize 100% of positive donors. Set of primers designed from conserved sequences of T. cruzi are convenient to recognize diverse DTU T. cruzi.
Footnotes
Disclosure Statement
No competing financial interests exist.