
Abstract
Tularemia is a rare zoonosis. The most common way is ingestion of contaminated meat or water, but the infection may also be acquired by insect bite. The clinical picture of the disease may be nonspecific. Due to polymorphisms of clinical picture, specific treatment is often delayed. In the last 50 years, in Poland, the most infections were acquired by handling hares. In our article, we present the case of a patient who was infected with Francisella tularensis due to arthropod bite. In the presented case, the diagnosis was difficult, because of the nonspecific clinical picture. Information of the epidemiology and the clinical picture changes of tularemia may have great clinical significance. Tularemia requires the special attention of physicians. All patients with lymphadenopathy and arthropod bite history should be screened for tularemia in the outpatient department and, if necessary, treated in hospital.
Introduction
Tularemia occurs in the Northern Hemisphere. In the United States, there are about 200 human cases of tularemia reported annually. In 2006, in European Union countries, the incidence of tularemia was 0.17 per 100,000 population (ECDC 2010). In Poland, in 2007–2008, only five new cases were reported (ECDC 2010, NIH 2010). Endemic foci have existed for a long time in the Russian Federation, Kazakhstan, and Turkmenistan. However, recent outbreaks of tularemia with hundreds of reported cases have occurred in Portugal, Spain, Sweden, Denmark, Finland, and Norway (WHO 2007).
Arthropod-borne transmission of tularemia was first observed by Francis in 1919, and tick-borne tularemia was first recognized in 1923 (Eliasson et al. 2006).
In humans, tularemia may take any of six different clinical courses: ulceroglandular (the most common form), glandular, typhoidal, oculoglandular, oropharyngeal, and septic (Jeżyna et al. 1976).
The bite of an infected vector may cause two primary disease forms: ulceroglandular and glandular (Eliasson et al. 2006). Here, we present a case report of a patient who was infected with F. tularensis through an arthropod bite in Poland.
Case Presentation
A 30-year-old male patient was admitted to the Department, because of enlargement of the right inguinal lymph node, which had been present for a month. The history indicated an arthropod bite in the area of the right ankle joint, possibly from a tick.
The disease began suddenly with high fever, shivers, and erythema-like skin change in the right ankle area (Fig. 1). The patient was treated with fluoroquinolone with no improvement.
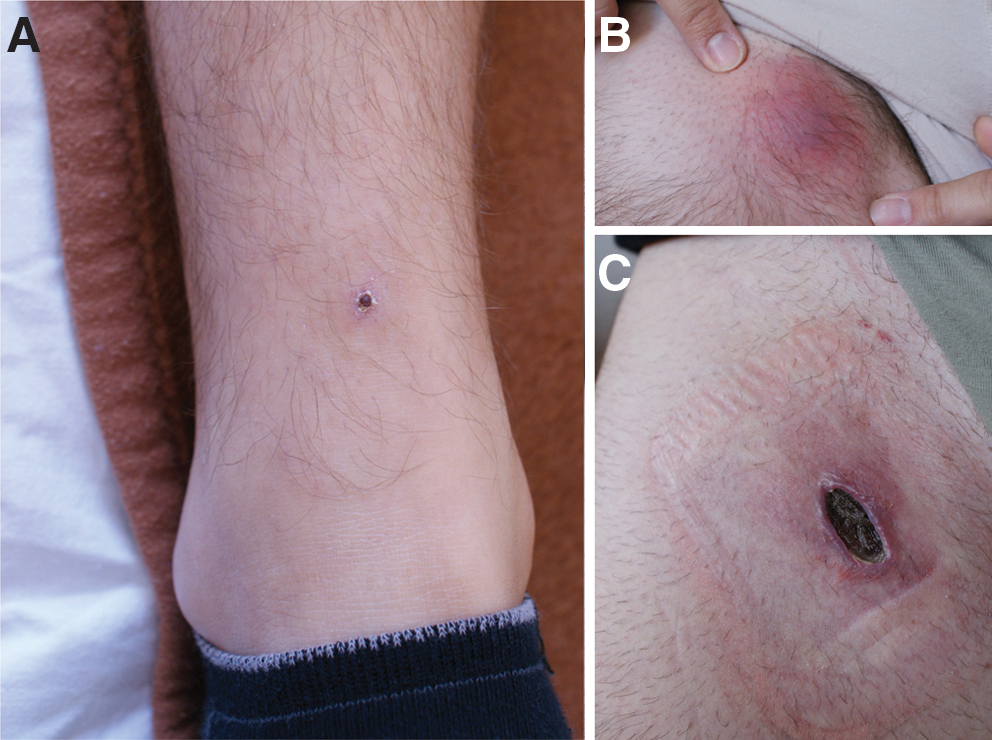
At admission to the hospital, a physical examination showed a tender, swollen, 1–2 cm diameter right inguinal lymph node with reddish and warm skin (Fig. 1). In laboratory tests, C-reactive protein (CRP) (53.9 mg/dL) and erythrocyte sedimentation rate (ESR) (23 mm/h) were raised.
An agglutination test was positive. Anti-F. tularensis antibody titer dynamics from 1:640 to 1:160 was observed. An ultrasound scan of the groin area showed an enlarged right inguinal lymph node (44×12 mm) surrounded by many smaller lymph nodes (15 mm diameter). An aspiration biopsy showed detritus with inflammatory cells.
Tularemia was diagnosed, and therapy of streptomycin—2×1.0 g i/m and ceftriaxon—2×1.0 g i/v for 12 days and then rifampicin for 10 days was introduced. During hospitalization, a fistula in the area of the suppurating right inguinal lymph node was observed. The wound required surgical treatment (Fig. 1).
After hospital discharge, the patient continued antibiotic therapy (rifampicin 2×600 mg) for 2 weeks. Then, in the right inguinal lymph node area, a wound with serous exudates was observed. Two weeks later, development of granulation tissue and purulent secretion were observed. Antibiotic therapy (doxycycline) was prolonged for another 2 weeks. After 8 weeks of antibiotic therapy, the patient reported complete recovery.
Discussion
It seems that tularemia occurs in humans much more frequently than previously thought. Worth emphasizing is the fact that, in Europe, tularemia has recently been reported mostly in Scandinavia and rather rarely in other countries (former Yugoslavia, Russia, Switzerland, Turkey). In 2008, Sweden reported the highest incidence rate (4.2 per 100,000 population), followed by Finland (2.2 per 100,000) and Norway (1.4 per 100,000) (ECDC 2010).
Outbreaks of tularemia may be associated with exposure to arthropods, infected mammals, food, water, or may be occasionally aerosol borne. Moreover, an increasing role of arthropod bite in transmission of F. tularensis in Europe is reported. Misić-Majerus et al. (1996) presented four patients affected with F. tularensis in Croatia, due to arthropod, tick, or other insect bite. Also, Hanke et al. (2009) reported a case of a 1-year-old toddler from Southwestern Germany with mosquito-bite-associated ulceroglandular tularemia.
In Poland, in the last 50 years, the most frequent cause of infection with F. tularensis was handling hares, when septic or typhoidal forms of tularemia were observed. Nowadays, the most common form of tularemia is ulceroglandular or glandular, often after an arthropod bite. In this article, we presented a case of ulceroglandular tularemia, although in north-eastern Poland also glandular form has been observed. A 46-year-old woman with glandular form of tularemia (enlargement of her left inguinal lymph node) was admitted to our department a few months earlier than the patient described in this article. The patient's history indicated that she had been bitten by a horsefly in the popliteal area (Moniuszko et al. 2010). Heterogeneity of clinical symptoms can cause diagnostic difficulties and delay treatment. Diagnosis should be based on positive serological tests, followed by cytological examination of lymph nodes (Splettstoesser et al. 2005).
The drugs of choice for tularemia are streptomycin or gentamicin, for 10 days. Other wide-spectrum antibiotics are also effective: tetracycline for 2–3 weeks, fluoroquinolones, and rifampicin. Sometimes, especially when the diagnosis is delayed, the therapy should be prolonged and include two or more antibiotics (Ikäheimo et al. 2000), as found in the described case.
Tularemia requires the special attention of physicians. All patients with lymphadenopathy and arthropod bite history should be screened for tularemia in the outpatient department and, if necessary, treated in hospital.
Footnotes
Acknowledgments
We thank Dr. Lesley Bell-Sakyi from The Roslin Wellcome Trust Tick Cell Biobank; The Roslin Institute and Royal (Dick) School of Veterinary Studies; and University of Edinburgh, Scotland, UK, for discussion and critical review of this article.
Disclosure Statement
All authors of this manuscript disclose any commercial associations that might create a conflict of interest in connection with the submitted article. The competing financial interests of all authors have been appropriately disclosed according to the policy of the journal. No competing financial interests exist.