
Abstract
Leishmaniases are vector-borne diseases transmitted by phlebotomine sand flies. Three species of Leishmania are found in the Mediterranean basin: Leishmania infantum, the most common species responsible for both visceral (VL) and cutaneous leishmaniasis (CL); Leishmania major, found in North Africa and Middle East causing CL; Leishmania tropica with a limited presence in Europe, causing CL. During the last 25 years, Crete has become an endemic zone for L. infantum with a high number of infected dogs and an increasing number of human cases every year; in the last 4 years, the incidence has reached an average of seven VL patients per year in a population of 600,000. At the same time, CL has re-emerged in Crete due to L. tropica, with an average of three CL cases per year in the last 4 years. Isolates were typed as L. infantum MON-1 and MON-98 and L. tropica MON-300, a zymodeme not reported before. Both VL and CL have spread to the whole of the island during the last 25 years, primarily in semi-urban and urban areas with altitudes of 0–50 m. The prevailing Phlebotomus species were Phlebotomus neglectus (proven vector of L. infantum) and Phlebotomus similis (suspected vector of L. tropica).
Introduction
L. infantum behaves as an opportunistic parasite; therefore, the importance of VL is not fully appreciated, since asymptomatic infections do not present the full extent of the spread of the disease. Also, such infections constitute a hidden problem since, if asymptomatic people become infected by human immunodeficiency virus (HIV), then they will develop the disease and, in addition, may be able to transmit the parasite to sand flies, thus changing the epidemiology of leishmaniasis. It is estimated that for every clinical case of VL there are 30 to 100 subclinical infections (Pampiglione et al. 1975).
On the other hand, CL is underreported because of its benign nature and the fact that it usually does not require hospitalization (Dujardin et al. 2008). As CL caused by L. tropica is anthroponotic in some, but not all, foci (Svobodova et al. 2006), patients are infective to sand flies, thus allowing the parasite to circulate and spread unnoticed.
Dogs constitute the reservoir of L. infantum to the sand fly vectors. Sero-prevalence in dogs has reached 42% in many endemic areas of Southern Europe (Belazzoug 1992), where it is a major veterinary problem (CanL). The most important factor in the epidemiology of VL, however, is that asymptomatic dogs, which are usually overlooked, can also infect sand flies (Alvar et al. 1994).
As far as Greece is concerned, L. infantum is present in nearly all the geographical areas of the country, causing VL, and L. tropica is found in the Ionian Islands (Nicolis et al. 1978, Stratigos et al. 1980) and in Crete, causing CL (Frank et al. 1993).
Twenty-five years ago, leishmaniasis was not considered a health problem in Crete although, before the 1940s, the visceral as well as the cutaneous form were widespread. In Crete, VL was first recorded in 1907 with high incidence in the human (Adler et al. 1938) and the dog population (Chaniotis 1994). The use of DDT against malaria vectors during World War II drastically reduced sand fly populations (Hertig 1949, Hadjinicolaou 1958). From 1951 to 1975, 33 alleged human VL cases were recorded on the island (Leger et al. 1979) and few canine leishmaniasis cases were reported until 1983 (Chaniotis 1994). Since then, Phlebotomus neglectus, the putative vector of L. infantum in Crete (Leger et al. 1988), has been found in high numbers on the island (Leger et al. 1993, Ivovic et al. 2007) and seroepidemiological studies in dogs, during the last 25 years, showed that the number of seropositive animals increases with time (Antoniou et al. 2009): from 0.27% in 1990 (Data of the Greek Ministry of Agriculture) to 2.9% in 1994 and 19.8% in 2009. This may be explained by the fact that dogs are brought into the island from mainland, especially from Attica, where leishmaniasis is endemic. The yearly increase in the number of seropositive dogs continues (Antoniou et al. 2009) and has been followed by the re-emergence and the yearly increase of human VL but also CL cases.
The aim of this study was to estimate the spread of human VL, CL, and also CanL on the island in time and space, to type the Leishmania isolates found in Crete, and to relate these results to the sand fly species present in the different areas of the island.
Materials and Methods
Study area
The study was conducted in the island of Crete, the fifth largest island in the Mediterranean Basin, situated in the Eastern Mediterranean. It is the southern border of Europe, between mainland Greece (160 km) and Africa (300 km). The island is 1 of the 13 districts of Greece with the size of 8336 km2 and population of 601,131 (Greek statistics department 2001). The island is composed of three mountains (2456, 2453, and 2148 m altitude), which take over most of its area, and it is divided into four counties (Fig. 1).
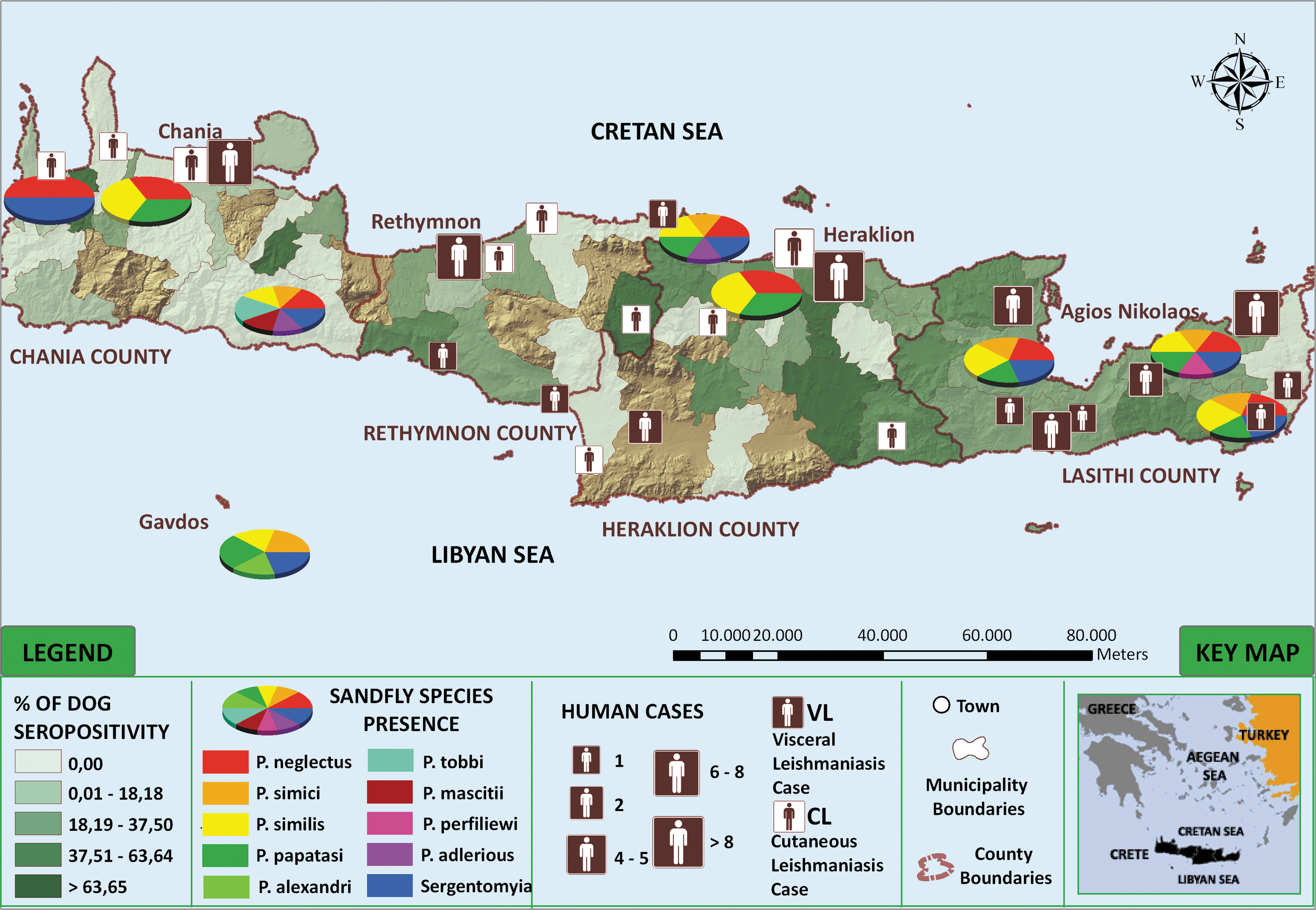
Geographical distribution of human leishmaniases cases (VL, visceral; CL, cutaneous) in Crete, in relation to Phlebotomus species presence and dog seropositivity. (P. adlerious is now Alderius subgenus.)
Human cases
From 1994 to September 2010, 1418 patients registered in different hospitals of the island, with persisting fever of unknown etiology or suspicious skin lesions, were tested in our laboratory since laboratory diagnosis of leishmaniasis in Crete is carried out in our hospital. In patients suspected of VL (with serology titer ≥1/160), polymerase chain reaction (PCR) and culture were performed on available biological material, and clinical and epidemiological information was collected, with the patients consent, using a questionnaire. A human CL case was confirmed by PCR and an attempt was made to culture the parasite from skin tissue and blood. Additionally, all members of the patient's family were checked for leishmaniasis by serology and the Government Veterinarians were informed of the case in order to test the dogs living in the area of the patient's residence. After treatment, the antibody titer of VL patients was followed for at least 1 year. Additionally, information on 15 human cases from Crete, diagnosed in other hospitals, mainly Athens, between 1986 and 2000, was supplied by the Ministry of Health (9 VL and 6 CL).
Dog epidemiological study
During 2005–2009, 1081 dogs (499 males and 582 females) from all four counties of Crete were sampled randomly: 281 from Heraklion, 463 from Lasithi, 109 from Rethymnon, and 228 from Chania. Villages were chosen by ballot from each county. The villagers were informed about the visit of the veterinarian team, and on the appointed day the dogs were gathered in the central square of the village for examination and bleeding. Samples were collected after the owner's consent and questionnaires with personal, epidemiological, and clinical data for each dog were completed. Peripheral blood (1081 samples) and lymph node aspirates from dogs with swollen lymph nodes (182 samples) were collected after clinical examination of the dog. The majority of these were hunting, guarding, and companion dogs. With the consent of the owner, 17 dogs, parasitologically proven to have leishmaniasis, were euthanized and the spleen was provided for examination. All dogs presented by the owners took part in the study, without eligibility criteria. The number of dogs sampled in each village depended solely on the number of dogs presented, which was a great proportion of the dogs living in that area.
Serology
Patient and dog sera were tested serologically using anti-human and anti-dog anti-IgG antibodies, respectively, by indirect immunofluorescence test (IFAT, Leishmania SPOT IF; BioMerieux France). A series of twofold serum dilutions starting from 1/40 were performed. Based on our experience the surveyed area is considered endemic for canine leishmaniasis, so a cut-off titer of ≥1/160 was regarded as positive for dogs (Ferroglio et al. 2002). A titer of ≥1/160 was considered suspicious for humans with VL symptoms, and further tests were performed to establish active infection. In CL patients, however, as well as in VL patients with immunosuppression, even with negative serology, PCR and culture of the parasite were performed on available biological material.
Polymerase chain reaction
PCR was carried out on peripheral blood, bone marrow, and/or skin from patients, and blood, lymph node, and/or spleen tissue from dogs, according to availability. QIAamp DNA Blood Mini kit (Qiagen) and DNeasy Tissue kit (Qiagen) were used for DNA extraction from blood and tissue, respectively. Primers T2 and B4, specific for Leishmania, were used as described by Minodier et al. (1997) with few modifications. In brief, the PCR mixture contained 1× DNA polymerase buffer (Qiagen) and 0.2 μM of each primer and, additionally, 0.2 mM dNTPs, 3 mM MgCl2, and 1.5U HotStar Taq polymerase (Qiagen). In this mixture, 1, 5, 10, or 20 μL of the template was added (PCR mixture total volume 50 μL). After 15-min initial activation of the HotStar Taq Polymerase at 96°C, 40 cycles of amplification (with each cycle consisting of 30 s at 95°C, 30 s at 62°C, and 20 s at 72°C) and a final extension step of 5 min at 72°C were performed, in an automatic thermocycler (Peltier Thermal Cycler, PTC 200). The reaction mixture (10–20 μL) was then analyzed by electrophoresis on a 1%–2% agarose gel and DNA was detected by post-staining, using the GelStar Nucleic Acid Gel Stain (Cambrex Bio Science Rockland, Inc.). After electrophoresis, the gel was placed in a polypropylene container containing 1× stain solution and incubated with gentle agitation for 30 min. The container was covered with silver foil to ensure gel protection from light during staining. A 312-nm UV transilluminator was used for dye excitation.
Parasite isolation and culture
Blood, bone marrow, and/or skin were used for the isolation of the parasites from all suspicious patients and blood, lymph node aspirate, or spleen tissue, according to availability, from all dogs taking part in the study. The samples were placed over Histopaque 1077 (Sigma; the tissue samples were first macerated in phosphate-buffered saline [PBS]) followed by subsequent washing of the white blood cells, thrice in PBS before they were resuspended in RPMI. Half the harvested cells were then placed in NNN and half in RPMI 1640 culture medium, containing 25 mM Hepes buffer, supplemented with 2 mM glutamine (GIBCO Invitrogen), 10% heat-inactivated fetal bovine serum (Gibco Invitrogen), 100 IU/mL penicillin, 100 μg/mL streptomycin (Roche Diagnostics), and 5% filtered human urine (Howard et al. 1991), at 26°C (±1°C). Promastigote cultures were maintained in the RPMI culture medium at 26°C (±1°C) (WHO 1991).
Parasite typing, zymodeme analysis
The parasites, isolated from patients and dogs, were typed by starch gel electrophoresis using 15 enzymatic systems according to Rioux et al. (1990).
Sand fly sampling
Sampling was carried out in various months during the whole sand fly season (May to October), from 2001 to 2010. Sand flies were collected by Center for Disease Control and Prevention miniature light traps and by mouth and electric-powered aspirators. The traps were battery-operated for one or more nights at various peridomestic domestic or other locations, usually at sites where domestic or productive animals were kept. The insect catch was checked early morning, and the trapped sand flies were sorted out and kept in 70% ethanol. With the exception of 275 females, the collected sand flies were mounted on permanent microscope slides for species identification, which was carried out according to morphology-based keys (Theodor 1958, Perfiliev 1966, Lewis 1982, Leger et al. 1986a, Depaquit et al. 2001). The 275 female sand flies collected in the village of Ziros, which had a high percentage of PCR-positive dogs and two human cases at the time of the study, were examined for the presence of Leishmania promastigotes in the gut, under sterile conditions, before species identification.
Statistical analysis and mapping of the results
Dog seroprevalence was estimated for each county and mapped using the geographical information system software (GIS; ArcGIS 9.3). Associations between (1) dog seropositivity or PCR dog positivity and nine potential risk factors were considered, namely, sampling season, geographical origin, age, sex, weight, coat shade, length of dog hair, presence of at least three of any of the classical CanL symptoms (lymph node swelling, dermatitis furfuracea, alopecia, ulcers, onychogryphosis, epistaxis, ocular lesions, splenomegaly, loss of weight, or unusual tiredness), and dog use (hunting, companion, guard dog, etc.) and (2) human cases in relation to their villages' land cover and altitude. They were presented as unadjusted odds ratios (OR), and adjusted OR allowing for the presence of other variables using logistic regression (univariate and multivariable model), and χ 2-tests were carried out. A 5% significance level was chosen throughout the study; SPSS version 17 was used.
To study the distribution of the disease, human cases and sand fly species were mapped in association with dog seroprevalence using the GIS software.
Results
Human cases
Between 1986 and September 2010, 85 patients developed leishmaniasis: they were 1–84 years old. Of these, 66 developed VL and 19 CL. VL patients were present in all age categories: 1–9 (16), 10–29 (9), 30–59 (12), and over 60 years (21). Additionally, eight VL cases were provided by the Ministry of Health with no information on patients' age. One of the 66 VL patients was HIV positive (45 years old), one had Salmonella typhi infection (73 years old), and one was immunosuppressed due to treatment for kidney failure (55 years old). Forty-five of the VL patients were positive by IFAT (titer 1/160–1/20,480). The parasite was isolated from 7 blood samples and 14 bone marrow samples from 16 VL patients. Most of the 66 patients with VL presented high fever (66), splenomegaly (59), and anaemia (57). All VL patients were treated with liposomal Amphotericine B or Meglumine antimoniate, and all recovered without relapses.
Between 1986 and September 2010, 19 cases of CL from different parts of Crete were diagnosed. Fifteen of these patients were over 60 years old. Of the remaining CL patients, three were 30–59 years old and one was 13 years old. One CL patient had developed Mycobacterium tuberculosis infection (male, 36 years old). All patients were positive by PCR and only three had antibodies against Leishmania (IFAT titer 1/160–1/320); these three patients later developed VL; one was alcoholic (32 years old), the other two were immunosuppressed (66 and 84 years old), and all were men. The parasite was isolated only from five patients. The CL patients had surgical removal of the lesion or cryoablation, and only five were given chemical treatment with Meglumine antimoniate. The CL patients who developed VL were treated with liposomal Amphotericine B.
Dog epidemiological study
During 2005 to 2009, 1081 dogs were examined: they were between the ages of <2 (223), 2–3 (371), 4–5 (220), and over 6 years (267) and the weights of <11 (208), 11–19.99 (477), and ≥20 kg (396). Of the 1081 dogs, 24.6% (266/1081) were positive by IFAT at ≥1/160 cut-off titer. In some municipalities, seropositivity by IFAT reached up to 76.5%. PCR, performed on blood samples of all 1081 dogs, resulted in 27.4% (296/1081) positives; so, 2.8% of seronegative animals resulted a positive PCR. Parasites were isolated from the blood (38 isolates), lymph node (32), and spleen (13) of 71 dogs, 13 of which were healthy-looking animals and 1 was seronegative. The most common symptoms in CanL dogs appeared to be lymph node swelling, dermatitis furfuracea, loss of weight, unusual tiredness, alopecia (especially around the eyes), onychogryphosis, and ulceration. Eighty-six animals without any leishmaniasis symptom were found seropositive.
Isolates
Twenty-one strains were isolated from patients: 16 from VL patients, typed as L. infantum (10 isolates were MON-1 and 6 isolates were MON-98) and 5 from CL patients: 3 were typed as L. infantum MON-1 (patients who also developed VL) and 2 were typed as L. tropica MON-300, a zymodeme that has not been reported before (64-year-old patients). All 71 strains isolated from dogs were typed as L. infantum (56 isolates were MON-1 and 15 were MON-98). One isolate, L. infantum MON-98, originated from the blood of a seronegative dog.
Sand flies
A total of 14,563 sand flies (7877 females and 6686 males) were trapped in nine areas during the summer months of the years 2001–2010. They belonged to nine different species of Phlebotomus and one of Sergentomyia (Table 1). None of the 275 dissected females, from Ziros village, were found to carry Leishmania. Since sampling was not done for the same number of nights and in the same month for each village, the results are mapped only as “presence of species.” P. neglectus, a known vector of L. infantum in the Mediterranean region, was found in all sampling sites in the island but not in the small island of Gavdos, south of Crete. P. similis, a suspected vector of L. tropica, was found in all sampled areas, including those with CL cases (Fig. 1).
Statistical analysis
The risk of a dog to come in contact with the parasite was found to differ according to the season of sampling (p<0.0001), with an increased risk in spring (OR=1.6; 95% confidence interval [CI]=1.2–2.3), summer (OR=2.2; 95% CI=1.5–3.2), and autumn months (OR=3.2; 95% CI=2.1–4.8) compared with winter months. The risk was also found to differ significantly according to the geographic origin of the dog (p<0.0001) with Heraklion prefecture having the greater number of seropositive animals. Age affected significantly this risk (p<0.0001), with the risk in 2–3-year-old dogs being 2.5 times higher than that of dogs less than 2 years old (95% CI=1.6–3.7), 2.2 times in dogs aged 4–5 years (1.4–3.5), and 1.8 times in dogs aged 6 years and over (1.2–2.8), compared with the youngest age group (Table 2).
The reference category for each factor is the level with an OR of 1.
Only variables retained in the final model are presented.
OR, odds ratio; CI, confidence interval.
At least three symptoms of leishmaniasis were observed in 194/1081 dogs (17.9%). The risk of seropositivity in dogs having at least three symptoms (p<0.0001) was found to be 7.05 times greater than that of dogs with no or one to two symptoms (OR=7.05; 95% CI=5.04–9.9). There was an increased risk of seropositivity in hunting dogs (p<0.0001; OR=1.7; 95% CI=1.2–2.4) and guard dogs (OR=1.8; 95% CI=1.1–3.0) compared with companion dogs. Dogs with short hair had a greater risk of being seropositive (p=0.016) than dogs with medium or long hair (OR=0.8; 95% CI=0.6–1.1 or OR=0.4; 95% CI=0.2–0.8). Weight, color, and gender were not significantly associated with seropositivity at univariate analysis at a 5% level. When all variables were initially included in a multivariable logistic regression model, the final model selected, following the stepwise selection procedures, consisted of the following explanatory variables: season (the risk being 1.6, 1.8, and 2.7 for dogs sampled on spring, summer, and autumn compared with winter, 95% CI=1.1–2.4, 1.2–2.8, and 1.7–4.3, respectively), geographic location (the risk being 0.6, 0.4, and 0.4 for dogs in regions of Lasithi, Rethymnon, and Chania, respectively, compared with those in the region of Heraklion (the reference category for each factor is the level with an OR of 1; 95% CI=0.4–0.9, 0.2–0.8 and 0.2–0.7, respectively), age (OR=1.9, 1.4 and 1.3 for 2–3, 4–5, and over 6-year-old dogs, respectively, compared with the youngest age dogs, 95% CI=1.2–3.05, 0.9–2.4 and 0.8–2.2, respectively), dog use (OR=1.6 and 0.8 for guard and hunting dogs, respectively, 95% CI=0.9–2.8 and 0.5–1.3, respectively), and presence of at least three symptoms (OR=5.8; 95% CI=4.0–8.3). In summary, 2–3-year-old guard dogs with at least three symptoms, sampled in autumn in the county of Heraklion, had the highest risk of being seropositive for Leishmania.
Using univariate statistical analyses, the risk of a dog being positive by PCR was found to differ significantly according to the following variables: (1) the season of sampling (p=0.004); (2) the geographic origin of the dog (p<0.0001); (3) the risk of a dog presenting at least three symptoms (p<0.0001); (4) the occupation of dog (p<0.0001); (5) dog age (p<0.0001), and (6) the short length of hair (p=0.029). When all variables were initially included in a multivariable logistic regression model, 2–3-year-old guard dogs sampled from the geographical region of Heraklion with at least three clinical symptoms had the highest risk of being PCR positive for Leishmania.
Studied villages were located at altitudes of 3—870 m with the majority (54.2%) at altitudes of 0–50 m, with predominant habitat semi-urban and urban (63%). When human cases were presented with village altitude, it was found that 80% of the studied villages with altitude 0–50 m had at least one human case: 56% with altitude 51–600 m and 13% with altitude >601 m (p<0.0001). Recorded habitat types also influenced the presence of human cases (p<0.0001) with 92% of semi-urban/urban villages with at least one human case, 42% of nonirrigated arable land, 46% of agricultural land with significant natural vegetation, and 54% of complex cultivation areas.
Discussion
Leishmaniasis, endemic in many parts of Europe, appears to be spreading (Bogdan et al. 2001, Maroli et al. 2008). During the last 25 years Crete has become a re-emerging focus of CanL, VL, and CL. Although L. infantum MON-1 is found predominantly in the Mediterranean Basin (90% of the typed isolates) (Hide 2001), zymodeme MON-98 is rare and this is the first time it is reported in Crete. L. infantum MON-98 was found in three patients and in dogs in Athens (Antoniou and Pratlong, unpublished data); Egypt [isolated from the sand fly P. langeroni (Doha and Shehata 1992), dogs (Shetata et al. 1990), and one VL patient (Youssef et al. 1989)]; Cyprus [isolated from one dog (Mazeris et al. 2010)]; and Portugal [isolated from one dog (Cardoso et al. 2002)]. The fact that this rare zymodeme was found in both Athens and Crete supports the hypothesis that infected dogs can have been brought via boat trips to the island from the mainland, especially from the endemic area of Athens (Tselentis et al. 1994), re-introducing the disease in the island.
In the majority of European countries, notification of VL is not obligatory, but even in countries where it is obligatory, underreporting is a common phenomenon. In Greece, human leishmaniasis is notifiable and has been reported in 8/13 regions and appears to be spreading geographically (Yiannakopoulos 1879, Parissis and Tetsis 1881, Tetsis 1881, Hart 1986, Papadopoulou et al. 2005, Diza et al. 2008, Antoniou et al. unpublished data). The number of CanL cases in Crete, since the re-emergence of the disease, has increased dramatically (Antoniou et al. 2009) accompanied by an increase in human VL cases (Fig. 2). Since leishmaniasis was considered a serious public health problem in Greece, with Athens been an endemic area (Tselentis et al. 1994), the Ministry of Agriculture was carrying out seroepidemiological surveys in the dog population for monitoring the disease. The re-emergence and spread of the disease in Crete is believed to be due to the introduction of infected animals from mainland Greece and not from increased vigilance, introduction of new diagnostic methods, or better medical knowledge. In old days, patients with VL were taken to Athens hospitals for treatment; VL cannot be ignored since it can be lethal if untreated.

Human CL and VL cases in Crete, since the re-emergence of leishmaniasis in 1984.
Canine leishmaniasis is endemic in many parts of Greece (Leontides et al. 2002) and it is known that a great proportion of dogs residing in endemic areas are infected, and infective to sand flies, even if they remain seronegative (Solano-Gallego et al. 2001). Serology detects most of the symptomatic (Ciaramella et al. 1997) and a proportion of the asymptomatic dogs, which may be as high as 50% of the seropositive canine population (Fisa et al. 1999). Consequently, seroprevalence of canine leishmaniasis is believed to be between the prevalence of the disease and that of the infection (Gradoni 1999). The important issue, however, is the ability of asymptomatic, but positive, dogs to transmit the parasite to the vector (Alvar et al. 1994, Gradoni 1999). The isolation of the parasite from the blood of one seronegative asymptomatic dog indicates that this is possible. However, since the majority of the PCR-positive dogs were dogs with at least three CanL symptoms (p<0.0001), symptomatic dogs are more likely to infect sand flies. By multivariable logistic regression analysis, it was found that 2–3-year-old guard dogs with at least three symptoms, living in the county of Heraklion, had the highest risk of being seropositive for Leishmania and thus present the highest risk for infecting the sand fly vectors. The percentage of seropositive dogs was high in most villages studied and human VL cases appeared in areas with dog seropositivity ranging from 9.1% to 57.1% (Fig. 1). Asymptomatic people from such areas may present transient parasitemia (Badaro et al. 1986, Chandra et al. 1991), and antileishmanial antibodies may be detected in healthy individuals making diagnosis of active VL difficult (Luz et al. 1997, Kyriakou et al. 2003).
L. infantum VL is currently considered a health problem for young children. In our study the age distribution of the disease ranged between 1 and 84 years. Of the 66 patients, only 16 were children up to 13 years of age. The others were between 22 and 84 years old, of which 30 were males and 14 females. Additionally, six VL patients were recorded by the Ministry of Health with no information on patients' sex or age. It is interesting to note that five healthy, immunocompetent adult men (34–42 years old) originating from endemic areas developed the disease 1 month after experiencing serious psychological stress. The epidemiology of the disease has been changing during the last years because of immunosuppression mainly due to HIV co-infection and the fact that the majority of HIV/AIDS patients lives in cities and may be infective to sand flies (Desjeux and Alvar 2003).
There are 12 known sand fly species in Greece, 9 of which belong to the medically important genus of Phlebotomus and 3 to Sergentomyia (Leger et al. 1986a, 1986b, 1986c). The putative vector of L. infantum in the Mediterranean region is P. (Larroussius) neglectus (Leger et al. 1988, Garifallou et al. 1989), which was the most frequent and abundant species found in all areas studied except in the small island of Gavdos, south of Crete. Our results confirm previous records of P. neglectus in Crete (Adler et al. 1938, Ristorcelli 1939, Hadjinicolaou 1958, Leger et al. 1993, Aransay et al. 1999), and show that the species is widely spread in the island (Fig. 1, Table 1). The close association of the vectors with human habitation, especially in rural areas, ensures transmission of L. infantum from infected dogs to humans and other animals. Most of the dogs studied (76.4%) lived outdoors, a factor believed to favor the rate of infection (Zaffaroni et al. 1999). Phlebotomus (Paraphlebotomus) similis was also found in all areas studied. Until recently, the importance of P. similis was largely speculated, and was not well understood. This species has not received much attention in terms of both ecology and distribution; moreover, it has often been misidentified as P. sergenti rendering any studies on its relationship with the distribution of leishmaniasis difficult. The phylogenetic study using the ITS2 region, as the genetic marker, suggested that P. similis and P. sergenti are sister species, which could imply a similar vector capability in relation to Leishmania species (Depaquit et al. 2002). The presence of P. similis in foci of human CL in Crete suggests that this species may be the potential vector of L. tropica in the island, a fact that needs further investigation. It has been shown previously that P. sergenti is not the sole vector of L. tropica as P. arabicus was shown to play a role in its transmission in Israel (Svobodova et al. 2006).
Crete had remained a latent focus for CL for over 25 years. Several strains, isolated from CL patients from Crete in the early 1980s, were typed as L. tropica MON-57 (Frank et al. 1993). The disease appears to have relapsed in the 15 CL patients over 60 years old who reported that during their childhood they, as well as most people in their village, had CL lesions known as the “Chaniotico spyri,” meaning “the skin lesion found in the area of Chania,” a well-known and common condition at that time in Crete. Possibly changes in the immune system of these people, due to age, have allowed the parasite to become activated and cause new lesions. The zymodeme L. tropica MON-300, not reported before, was isolated from two women of 64 years old, both from Rethymnon County. The differences between L. tropica MON-57 and MON-300 concern 7 enzymes out of the 15 studied. This expresses a polymorphism of L. tropica in Crete, but more strains need to be studied before associations with different cycles of L. tropica in the island can be made. It is possible that more CL patients are found in Crete since people, being aware of its benign nature, do not consider it necessary to visit the doctor, especially people of older ages, but such patients are infective to sand flies; therefore, the parasite circulates in the environment and spreads unnoticed. The three CL cases, due to L. infantum, were observed in two immunosuppressed patients and an alcoholic male, and all proceeded to visceral disease.
Leishmaniases are favored by the changing conditions, like the movement of people and animals, the buildup of vector populations due to changing climatic and environmental conditions, and changes in animal husbandry practices (many animals in Crete are now kept in farms rather than move around according to availability of vegetation), which are favoring the parasite and its vectors and allowing them to spread in space and time. Studies are undertaken to foresee changing conditions and how they affect parasite spread (EDEN [
Measures for safeguarding unaffected areas from the introduction of this pathogen and its vectors are not undertaken by any country, and the example of the introduction of Leishmania donovani MON-37 in Cyprus (Antoniou et al. 2008) is an indication of the enhanced movement of pathogens by globalization. The introduction of novel pathogens in new areas may pass unnoticed since physicians may be ill-informed on the diagnosis and treatment of the disease, especially if of benign nature. In such cases, genetic exchange between different species or strains of the pathogen can create new hybrids that may behave differently, thus affecting the epidemiology, pathogenicity, or drug resistance of the disease—the case already been illustrated in Leishmania (Ravel et al. 2006, Volf et al. 2007).
In Crete the conditions are favorable for the spread of VL and CL, a situation witnessed in the last 25 years, with the incidence rising from 0 (1984) to 1.33 per 100,000 (2010) inhabitants (Fig. 2). The sand fly vectors, able to transmit L. infantum and L. tropica, are widespread in the island and the parasites are well established.
Footnotes
Acknowledgments
This work is part of a project supported by The European Commission Research Directorates (“Leishmania genotyping” Contract No. QLK-CT-2001-01810); the Ministry of Education of the Czech Republic (projects MSM 0021620828 and LC 06009; to Vít Dvorak and Grant Agency of Charles University (grant no. 131208 “Intraspecific variability and molecular taxonomy of phlebotomic sand flies of subgenus Larroussius, important vectors of human leishmaniosis”); the EU grant GOCE-2003-010284 EDEN (
Disclosure Statement
All authors state that they have no commercial or financial associations that may create a conflict of interest in connection with this article.