
Abstract
Crimean-Congo hemorrhagic fever (CCHF) is a virus transmitted predominantly by ticks. However, contact with infected body fluids or tissues can result in animal-to-human or human-to-human transmission. Numbers of CCHF cases appear to be increasing, especially in Europe. We reviewed cases admitted to a tertiary referral unit in Kosova with suspected CCHF in 2008 and 2009, and looked at a smaller number of specimens which were sent to the Health Protection Agency, Porton Down, U.K., in further detail. The clinical features of cases admitted with suspected CCHF infection were assessed in more detail, and these are the focus of this article. Between 2008 and 2009, the numbers of patients admitted for suspected CCHF infection increased. Of the samples received in Porton Down, CCHF virus was detected in urine samples, and these patients were found to have prolonged viremia. The detection of CCHF in urine, as well as the prolonged viremias seen, are important for clinicians to know, as they may have public health implications with regard to the risk of infection, as well as provide insights into the biology and pathophysiology of infection. Further studies are required regarding the pathogenesis of this virus.
Introduction
The Balkans are included in the endemic zone for CCHF in Europe, and there have been many reports of sporadic cases and outbreaks from this region. Climatic, environmental, and agricultural changes may affect the distribution of the tick vector, and therefore influence the location and timing of outbreaks. The economic and political crisis in Kosova in the 1990s increased the rural and agricultural populations due to people moving out of larger cities, which could have affected the distribution of these vectors. The first case of CCHF in humans in Kosova was reported in 1954, and seroprevalance rates of the virus in more recent times are reported to be about 24% in humans (Dedushaj 2006), with rates of 14% in cattle and 32% in sheep.
CCHF activity appears to be increasing, especially in the European region (Maltezou et al. 2010; Papa et al. 2011). The pathogenesis of CCHF is not completely understood, mainly due to a lack of adequate animal models and laboratories with the appropriate bio-safety containment facilities. We collected data from suspected cases of CCHF admitted to a tertiary referral unit in a large hospital in Prishtina, Kosova.
Methods
In 2008 a total of 87 patients were admitted with suspected CCHF, and in 2009 this number increased to 124 suspected cases. A number of these samples were sent to the reference laboratory at the Health Protection Agency (HPA), Porton Down, U.K., for further laboratory testing.
A suspected case was defined as an acutely ill patient with clinically-observed signs and symptoms of CCHF infection, and with epidemiological risk factors with or without laboratory data indicative of leukopenia or thrombocytopenia. A confirmed case was defined as a patient with detectable CCHF RNA in serum samples.
Serum samples from some suspected cases and urine samples from some of the same patients were sent for polymerase chain reaction (PCR) testing from 2008 and 2009. Two reverse transcriptase PCR (RT-PCR) assays were performed to detect CCHF viral RNA. The block assay target is a region of the nucleocapsid protein gene, specifically the 5′ end of the S segment (around 520 nucleotides), and is performed with the Qiagen one-step RT-PCR kit (Qiagen, Hilden, Germany). The real-time RT-PCR target is within the S gene, and uses the Taqman methodology on the LightCycler to amplify and detect target RNA, with a positive control RNA transcript designed on a 329-bp sequence from the SA81 CCHF strain (National Center for Biotechnology Information [NCBI] Genbank no. DQ076416). The kit used is the Invitrogen Superscript III Platinum qRT-PCR kit (Invitrogen, Carlsbad, CA; Atkinson et al. 2011). IgG serological analysis was originally conducted using immunofluorescence assay (IFA; in-house methodology) for samples from 2008. Samples from 2009 were analyzed serologically using a recently developed enzyme-linked immunosorbent assay (ELISA; Dowall et al. 2011). ELISA results for the 2008 samples were checked retrospectively and gave the same results as the IFA test.
The clinical diagnostic features of the cases were reviewed from the data provided to the laboratory, and diagnoses in cases with samples found to be negative were also reviewed.
Results
In 2008, 87 patients suspected of having CCHF were hospitalized in the Clinic of Infectious Diseases. All of the patients had a decrease in their erythrocyte count, leukopenia, thrombocytopenia, and raised aspartate aminotransferase (AST 100–1200 U/mL) and alanine aminotransferase (ALT 200–900 U/mL). Fourteen of these patients had samples sent for further analysis. These patients had a median (range) age of 23 years (11–83), and 43% (6 patients) were male. The main presenting signs and symptoms for this cohort included fever (76.9%), myalgias (76.9%), arthralgias (69.2%), bleeding (61.5%), thrombocytopenia (53.8%), epistaxis (21.4%), hematemesis (28.5%), and conjunctival injection (21.4%; Fig. 1).
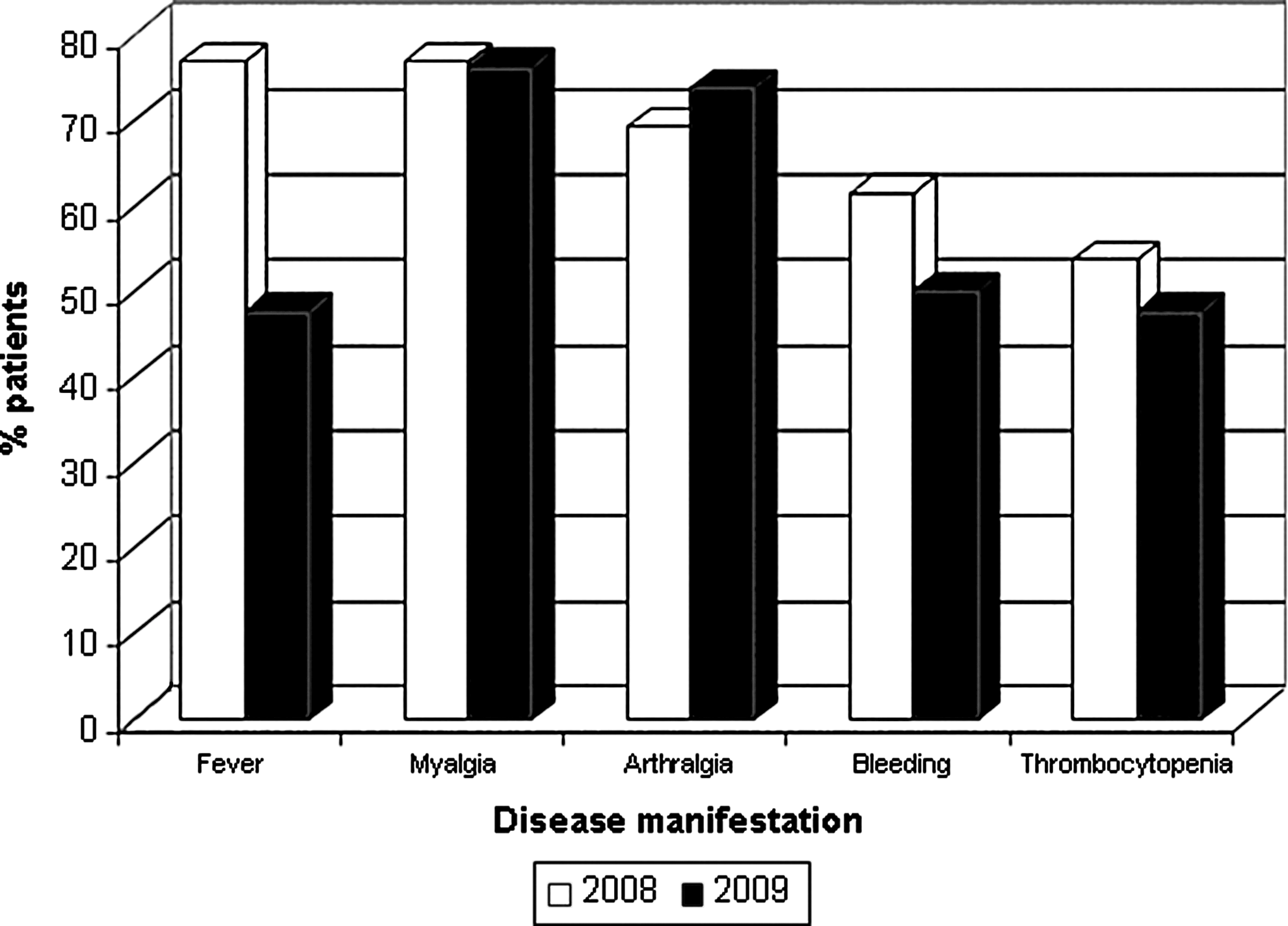
Percentage of patients with disease manifestations of CCHF in 2008 and 2009.
The remaining patients were given a diagnosis of CCHF based on epidemiological, clinical, biochemical, and hematological laboratory data. All of the patients were exposed to tick bites or had direct contact with CCHF patients, and lived in areas of known CCHF prevalence. The clinical manifestations and laboratory data in these patients were similar to those of patients who had positive PCR results.
Of the 14 samples received in the HPA, 5 were proven to have CCHF with a positive PCR from serum samples; 2 of these patients with positive serum samples were also noted to have CCHF RNA detected from urine samples (Table 1). Four of these samples also had positive serology, with the remaining sample being equivocal at the time of testing (Table 2). Attempts to culture the virus from these samples have been negative to date. This may be a result of the challenges faced when transporting samples from one country to another, or to delays or degradation of the samples. The CT values for the PCR tests carried out on these samples ranged between 23.25 and 33.63.
POS, positive; NEG, negative; −, no sample; PCR, polymerase chain reaction.
POS, positive; NEG, negative; −, no sample; PCR, polymerase chain reaction.
In 2009, 124 patients suspected of having CCHF were hospitalized in the Clinic of Infectious Diseases, and 42 of these patients who were suspected of having CCHF based on their exposure histories and clinical findings had their samples sent to the HPA. The median age of the second cohort of 42 patients was 36 years (range 11–84 years), and 42.9% (18 patients) were male. The main presenting features were myalgias (76.2%), arthralgias (73.8%), bleeding (50%), thrombocytopenia (47.6%), and fever (47.6%; Fig. 1). Nine of these patients had a history of contact with patients suspected of having CCHF, and then developed symptoms of infection, but they all had negative PCR results.
Of these 42 patients, 9 patients were proven to have CCHF. All of these diagnoses were based on the detection of viral RNA from serum, and 3 of these patients were also found to have a positive PCR for CCHF from urine samples (Table 1). Serology has so far been positive in 5 out of 6 of these 9 samples (Table 2). All 9 of these patients were treated with either oral or intravenous ribavirin. An additional 8 patients in the cohort had documented evidence that they were also treated with ribavirin. In addition, 3 of the PCR-negative samples had positive serology (Table 2). Unfortunately some of the remaining samples had degraded and were not suitable for further analysis.
Again, the remaining patients were given a diagnosis of CCHF based on epidemiological, clinical, and laboratory data. All the patients were exposed to tick bites or had direct contact with CCHF patients and lived in areas of known CCHF prevalence. The clinical manifestations and laboratory data in these patients were similar to those of patients who were PCR-positive. There was 1 death in the 2008 admissions, compared to 3 in the admissions from 2009, and the remaining patients recovered from their illness.
Patient HR (Table 1) had very severe CCHF with severe hemorrhagic manifestations. He was given ribavirin, and after treatment recovered completely and is now healthy and well.
Discussion
The main vector of disease is the tick, particularly those of the species Hyalomma. The geographical distribution of these ticks also correlates with that of the disease (Hoogstraal 1979), and this distribution is wide, including Africa, Asia, Eastern Europe, and the Middle East (Whitehouse 2004). Kosova covers an area of 10,887 km2 in the central Balkans, and it has a population of 2.4 million people. Following years of conflict, it has a high unemployment rate and increasing rates of poverty. The nation's overall health is considered to be among the worst in Europe.
CCHF is a serious pathogen that can cause a fatal hemorrhagic disease. Few data are available on the numbers of patients affected by this disease in Kovsova before the mid-1990s, but between 1995 and 2002, the number of suspected cases was high, peaking in 1995 (122 suspected cases with 7 deaths), 2001 (115 suspected cases with 7 deaths), and 2002 (114 suspected cases with 3 deaths; Jameson and Medlock 2009; Fig. 2). CCHF appears to be present in about 50% of the municipalities of Kosova, and as such is of serious concern in that region (Jameson 2009). As the vectors for this disease have the capability of spreading, this is also a major concern for the unaffected areas of Europe.
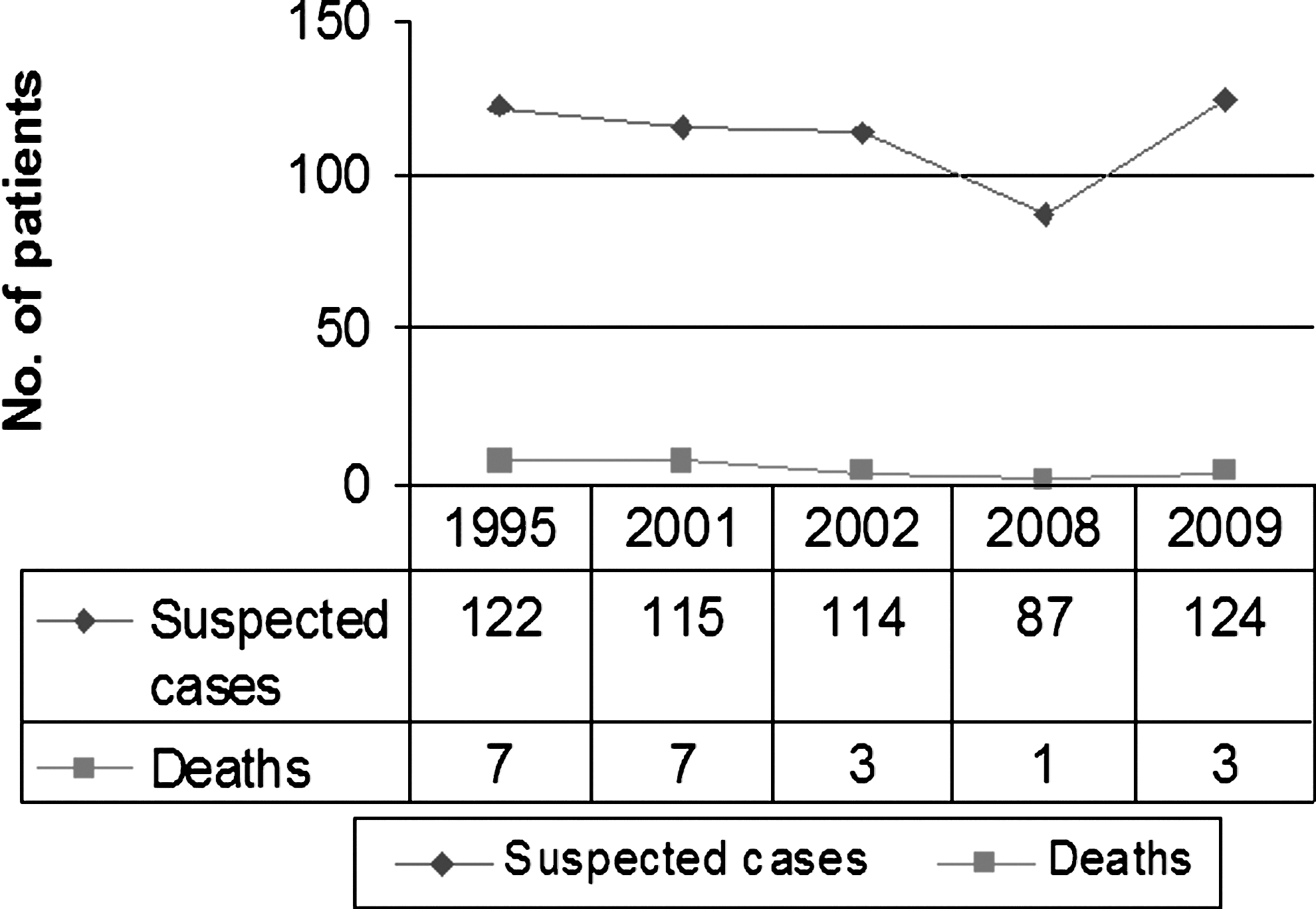
Recorded data of deaths and suspected cases of CCHF infection.
Clinical features of CCHF can be divided into four periods: incubation, pre-hemorrhagic, hemorrhagic, and convalescence (Hoogstraal 1979). The incubation period varies between 2 and 9 days, depending on the transmission route (Swanepoel et al. 1987), and clinical symptoms such as fever, headache, myalgias, arthralgias, and vomiting may appear at this point. Additional features such as sore throat, conjunctivitis, jaundice, and photophobia may also develop. Hemorrhagic manifestations may appear 3–6 days following disease onset in severe cases. Ecchymosis and petechiae of the skin and mucous membranes, as well as gastrointestinal bleeding, are the most common symptoms at this stage (Feldmann et al. 2003). Severe manifestations include cerebral hemorrhage and liver necrosis, and these are associated with a poorer prognosis. Epistaxis can occur, which along with the gastrointestinal bleeds, can be of particular concern to health care workers. Mortality rates usually range between 5 and 50% (Hoogstraal 1979), although numbers as high as 80% have been reported sporadically (Yu-Chen et al. 1985). The World Health Organization cites rates up to 30%. The clinical features of the cohorts reviewed here were consistent with the findings from previously-reported outbreaks.
The positive PCR results from urine are of interest, and this is a relatively new finding in relation to CCHF, which has only been described once before (Bodur et al. 2010; Table 1). This previous study also showed positive PCR results from urine with no virus isolated to date, so it is difficult to determine if the positive PCR results relate to live viable virus or not. However, positive urine results have previously been seen with other viral hemorrhagic fever (VHF) viruses, including Lassa fever, and Marburg and dengue virus, suggesting that CCHF also has a urinary phase in infection, and also suggesting that these samples, in combination with serum samples, could be used for diagnostic purposes (Lunkenheimer et al. 1990; Chupurnova et al. 2000; Mizuno et al. 2007). This also has public health implications. Other VHF viruses have been detected in urine and seminal fluid for months after the initial infection (Rowe et al. 1999; Rodriguez et al. 1999), making sexual transmission a possibility. These patients are therefore advised to have protected sex for at least 3 months post-infection. There is anecdotal evidence in Kosova of sexual transmission of CCHF. This may have further implications regarding infection control for affected patients into the convalescence period, but more work needs to be carried out to establish how common excretion in the urine and seminal fluid is, and for how long into convalescence it continues.
It is also notable that some patients also had positive PCRs from urine samples early in the disease process, which again could have infection control implications. Further investigation into this aspect of infection could improve the current knowledge and understanding of the pathophysiology of this infection.
There was a group of patients presenting with clinical, laboratory, and epidemiological risk factors for CCHF, who had negative PCRs from serum. This may be due to the timing of the sample taken during the illness. The majority of patients admitted had presented late in the course of disease (usually from the 10th day onwards). No other diagnosis was made in these cases, and clinically they behaved like CCHF infections, suggesting that the viremia can be quite variable in different people, and that it appears that the majority of patients are able to clear the virus from their blood while still having a clinical picture of infection. Initial results from three of the PCR-negative samples have shown positive serology, suggesting that the timing of taking these samples can have a bearing on their results (Table 2). Unfortunately, at the time these patients were seen, the laboratory facilities available for diagnosis were variable, and therefore it was not possible to assess the accuracy of clinical diagnosis and correlate this with laboratory diagnosis in all of the cases described above. As facilities improve in countries affected by this disease, this information should become more readily available.
Interestingly, however, two patients (HR and AK; Table 1) in these cohorts had prolonged viremias. Both patients still had detectable viral RNA in their blood at 34 and 36 days from the onset of illness, despite clinically appearing to be in the convalescent phase. The possibility of ongoing infection at this stage in the disease seems unlikely. It is not clear whether these samples represent infection with live, viable virus or not. Clearly, if this does represent live virus, this implies the possibility of continued shedding and transmission, despite a clinically-recovering patient. Patient AK had a stormy clinical course and was in the hospital for a number of weeks following a cardiac arrest. Her electrolytes had been markedly abnormal, and may have contributed to an arrhythmia. She made a full recovery, but continued to have detectable viral RNA in her serum until day 36 from the onset of illness. This could have implications for nosocomial and continued community transmission, and suggests that some patients could act as chronic carriers of virus, despite a clinically-improved picture, with the potential to spread the virus through body fluids, especially semen, but larger groups of infected patients should be monitored to see how common this is.
There is ongoing debate regarding the effectiveness of ribavirin for CCHF, with the suggestion that it could be of some benefit in infected patients (Soares-Weiser et al. 2010). Unfortunately ribavirin was not continually available in Kosava over the period of this review, and therefore it was not possible to assess the relationship of PCR positivity and outcome to treatment in this group of patients. This is, however, an area for future research.
Data on CCHF outbreaks allow the disease to be studied in more detail, and help us understand not only the pathogenesis of the disease, but also the factors involved that led to outbreaks. Complete analysis of samples from infected patients throughout the course of their illness (including serum, whole blood, and urine) is needed to provide an accurate picture of what happens during CCHF infection. This is a serious illness, and its vectors are capable of spreading; therefore a better understanding of the natural history, clinical presentation, and progression of the disease, as well as its pathogenesis and available treatments will ultimately allow more timely interventions not only at the local hospital level, but also on a larger public health level, which should help prevent its spread.
Footnotes
Acknowledgments
We wish to thank the staff of the Clinic of Infectious Diseases, University Clinical Center of Kosova, Prishtina.
Author Disclosure Statement
No competing financial interests exist.