
Abstract
Positive cultures from hepatic abscess drainage are extremely rare, and in this case the infection would have remained undiagnosed if Brucella suis had not been isolated. Failure to correctly diagnose this zoonosis delays patient treatment and is dangerous, as in this case that could have been a laboratory-acquired disease. This type of infection is preventable if proper safety protocols are established and followed.
A 74-year-old man was admitted with a 2-week history of mild evening fever, asthenia, night sweats, depression, anorexia, low body weight, fomites, and abdominal pain localized in the right hypochondrium. Laboratory studies showed hematocrit 46.7%, white blood cell count 9700/mm3, platelet count 215,000/mm3, neutrophils 66%, glucose 93 mg/dL, urea 20 mg/dL, cholinesterase 6681 U/L, prothrombin time 15.2 sec, and partial thromboplastin time 28.0 sec. Levels of aspartate transaminase, alanine aminotransferase, and bilirubin were not tested.
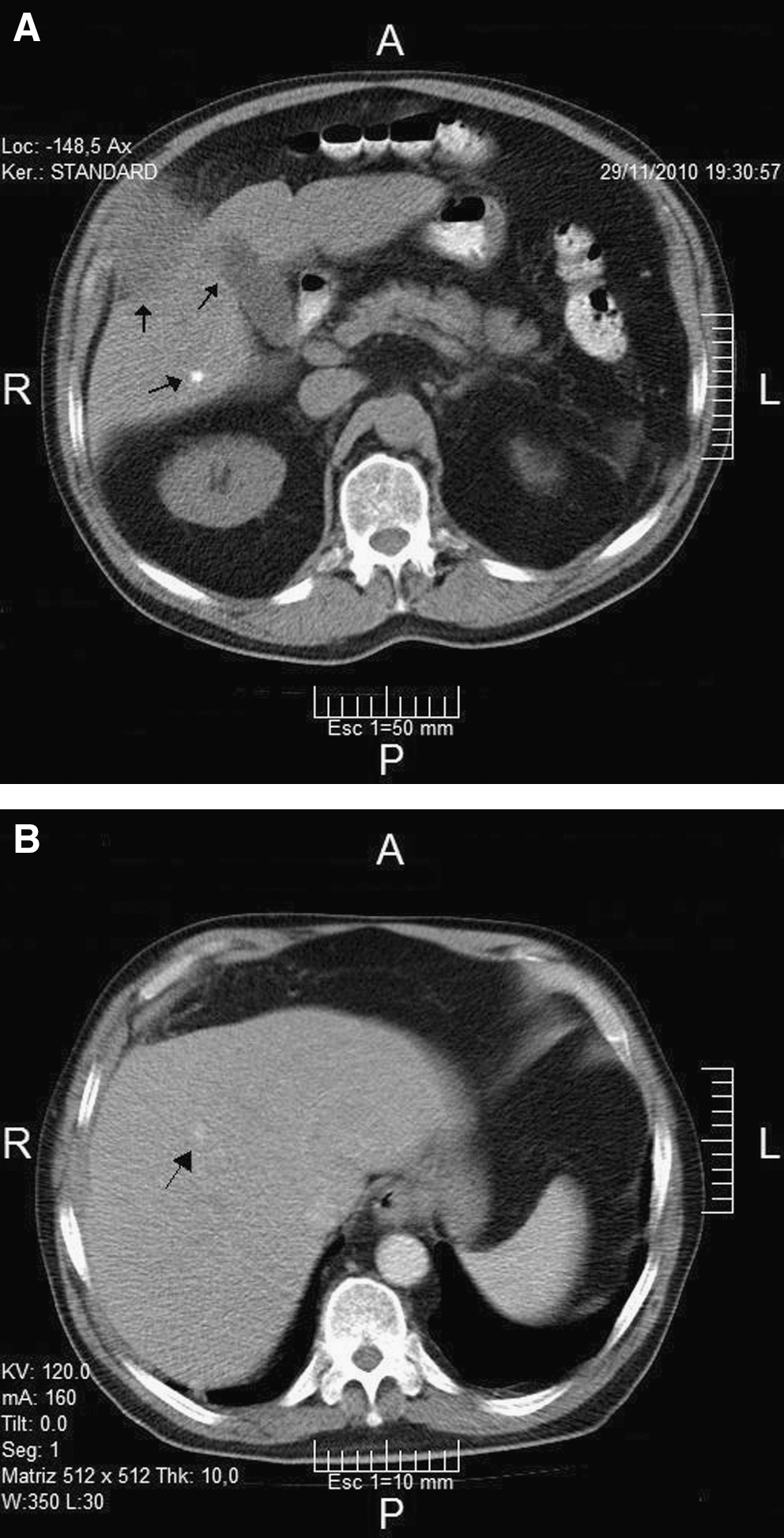
Abdominal ultrasound showed liver enlargement and heterogeneous echogenicity of the parenchyma similar to fatty liver. It demonstrated three well-defined anechoic formations with thin walls, one on the left side that was 2 cm in diameter, and two in the right lobe, the larger of which was 2.8 cm in diameter. Two parenchymal calcifications were also observed, one of which was juxtaposed to a cystic formation. At the subphrenic level, omental thickening surrounding an anechoic area with partially-defined edges about 2.8×1.4 cm in size was seen. Abdominal computed tomography (CT; Fig. 1A) confirmed the ultrasound findings, and a diagnosis of hepatic abscess was made and surgery indicated. The day after admission surgical drainage was performed, and the patient had good recovery and was discharged 4 days later.
(
One week later the patient was re-admitted with complaints of fever and abdominal pain at the surgical site. A CT scan (Fig. 1B) showed no surgical complications and laboratory tests showed hematocrit 44%, white blood cell count 7400/mm3, neutrophils 75%, glucose 110 mg/dL, urea 45 mg/dL, total bilirubin 1.43 mg/dL, direct bilirubin 0.82 mg/dL, aspartate transaminase 24 U/L, alanine aminotransferase 19 U/L, and alkaline phosphatase 178 U/L. A two-dimensional echocardiogram was negative for endocarditis. Gram stain of the liver abscess drainage fluid showed only polymorphonuclear leukocytes; it was spread onto blood soy protein agar plates (BSPA; Britania SA, Buenos Aires, Argentina) and thioglycolate broth. A strain grown in the latter after 72 h of incubation was subcultured on BSPA, and 48 h later gram-negative coccobacilli were observed. They were catalase-, urease-, and nitrate reduction-positive, oxidase- and glucose-negative, and colistin-resistant. Brucellosis was suspected and the strain was sent to our laboratory for confirmation. The patient was placed on doxycycline 200 mg daily and rifampin 900 mg daily for 6 weeks, and recovery was progressive and asymptomatic, and the patient was discharged with good recovery 5 days after the second admission.
In our laboratory the strain was typed as Brucella suis biovar 1 based on procedures described previously (Corbel et al. 2005). An oxidase test was positive, agglutinated with monospecific anti-A serum, CO2 was not required, and upon urease testing using Bauer's method the color changed to pink in 15 min. Production of H2S tested positive on all 4 days, growth on thionine 20 μg/mL and erythritol 1 mg/mL was positive, but was inhibited by basic fuchsin 20 μg/mL and penicillin 5 IU/mL. It was lysed by Wb and Iz phages, but not by Tb and R/C.
Because during the isolation process Brucella spp. had not been considered, it had been manipulated on an open bench by two laboratory technicians; one received prophylactic treatment with doxycycline-rifampin for 6 weeks, and both were monitored by clinical examination and serological tests (Yagupsky and Baron 2005).
Fourteen days after admission the first samples of serum from the patient and the two exposed laboratory workers were assayed. Studies included a buffered plate agglutination test, a Rose Bengal test, a serum agglutination test (SAT), complement fixation test (CFT), and competitive ELISA (cELISA; Lucero et al. 2007). The laboratory workers tested negative on all tests, whereas the patient tested mild positive on the SAT (50 IU/mL), and strong positive on the CFT (400 ICFTU) and cELISA (82). The classic SAT that is valuable for the acute form of the disease is not suitable for the detection of chronic cases. CFT identifies mostly IgG antibodies that appear in chronic forms, and of the newer serological tests, cELISA titers correlate well with the clinical course, and is useful to detect both the chronic and acute forms.
Six months later, serological tests from the patient showed few differences, and the laboratory workers continued to test negative.
This disease is nearly always acquired directly or indirectly from contact with animals, and contaminated abortion, genital discharge, and unpasteurized dairy are major sources of infection. Although the true incidence of human brucellosis is unknown in Argentina, in 2010, 394 new cases were notified to the Laboratory Module of the National Health Surveillance group (SIVILA-SNVS) maintained by the Ministry of Health. Most cases were diagnosed by epidemiology or clinical and serological tests, since isolation procedures are not routinely applied. Nevertheless, at the National Human Brucellosis Network-ANLIS between 1994 and 2010, 473 strains were isolated from humans: 41.2% B. suis, 38.9% B. melitensis, 18.8% B. abortus, and 1% B. canis.
Our patient related a previous brucellosis episode 30 years earlier, when he was working in a pig slaughterhouse, and consequently the present infection could be a reactivation. Recently a case of reactivation 28 years after the first episode was reported (Ogredici et al. 2010). Positive cultures from caseiform pus are extremely rare; however in this case, the infection would have remained undiagnosed if the culture had not been positive, since serological tests were not run because brucellosis was not suspected. On the basis of this experience, brucellosis testing should be used for differential diagnosis in regions where the disease has not been eradicated. Failure to correctly diagnose this zoonosis and identify strains of Brucella spp. is dangerous, and in the present case could pose a potential risk for laboratory technicians working with these specimens, due to its ability to be aerosolized. Additionally, this type of infection is preventable if proper laboratory safety protocols are established and followed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.