
Abstract
In 2011, autochthonous Plasmodium vivax malaria emerged in a focal geographical area in Greece after importation by immigrants from the Indian subcontinent. We report the case of complicated P. vivax malaria in a previously healthy 42-year-old Greek female. The patient presented acute respiratory distress syndrome (ARDS), worsening jaundice, and thrombocytopenia after the administration of antimalarial treatment and despite a decreasing burden of parasitemia. She recovered fully after admission in the intensive care unit and support with mechanical ventilation. We discuss the risks potentially associated with the reappearance of P. vivax malaria in a previously malaria-free area.
Introduction
P
A relevant example is Greece, where a cluster of 34 cases of autochthonous P. vivax malaria was noted during 2011 in a limited geographical area around the delta of Evrotas River, District of Laconia, according to official data from the Hellenic Center for Disease Control and Prevention (
Case Presentation
A 42-year-old female schoolteacher from the District of Laconia in South Peloponnese, Greece, was transferred to our hospital in August, 2011, because of prolonged fever combined with severe thrombocytopenia, transaminasemia, and jaundice. She had been well until 2 weeks earlier when fever with rigors developed. As an outpatient, she had initially been treated with cefuroxime, but showed no clinical response. When first admitted to a district hospital due to persistent fever and prostration, she received moxifloxacin for 3 days but was referred to our hospital as her general condition deteriorated.
The patient had no history of recent travel abroad or receipt of a blood transfusion. She reported occasional tobacco use. At presentation to our hospital, she was conscious and fully oriented. Her temperature was 38.5°C, her blood pressure was 105/60 mmHg, and her pulse rate was 100 beats per minute (bpm). Oxygen saturation was 99% while breathing room air. The pulmonary and cardiac sounds were normal. The rest of the physical examination was unremarkable. The following routine laboratory tests results were noted (Table 1). Abdominal ultrasonography, chest X-ray, and electrocardiography were unrevealing. Examination by microscopy of the peripheral thick and thin blood film revealed P. vivax with a low level of parasitemia (7 parasites/1000 erythrocytes). Further confirmation was provided with a single-step, multiplex PCR-based method, at the Malaria Reference Laboratory, National School of Public Health, Athens, Greece. The laboratory details for this method have been described previously (Patsoula et al. 2003). There was no microbiological evidence of bacterial or viral co-infection (negative blood cultures at admission). The patient was treated with mefloquine (1250 mg in total). During the following 3 days, the fever persisted but the rigors regressed. Despite further reduction of P. vivax parasitemia, the patient experienced clinical deterioration (Table 1). Seventy-two hours after the administration of antimalarial treatment, she developed acute dyspnea, tachypnea, bilateral crepitations at lung bases, and hypoxemia while breathing room air [arterial blood gases: pH 7.48, partial carbon dioxide pressure (PCO2) 30 mmHg, partial oxygen pressure (PO2) 60 mmHg, bicarbonate (HCO3) 23 mmol/L, saturation level of oxygen (SaO2) 91%]. A new chest X-ray showed bilateral diffuse alveolar infiltrates (Fig. 1).
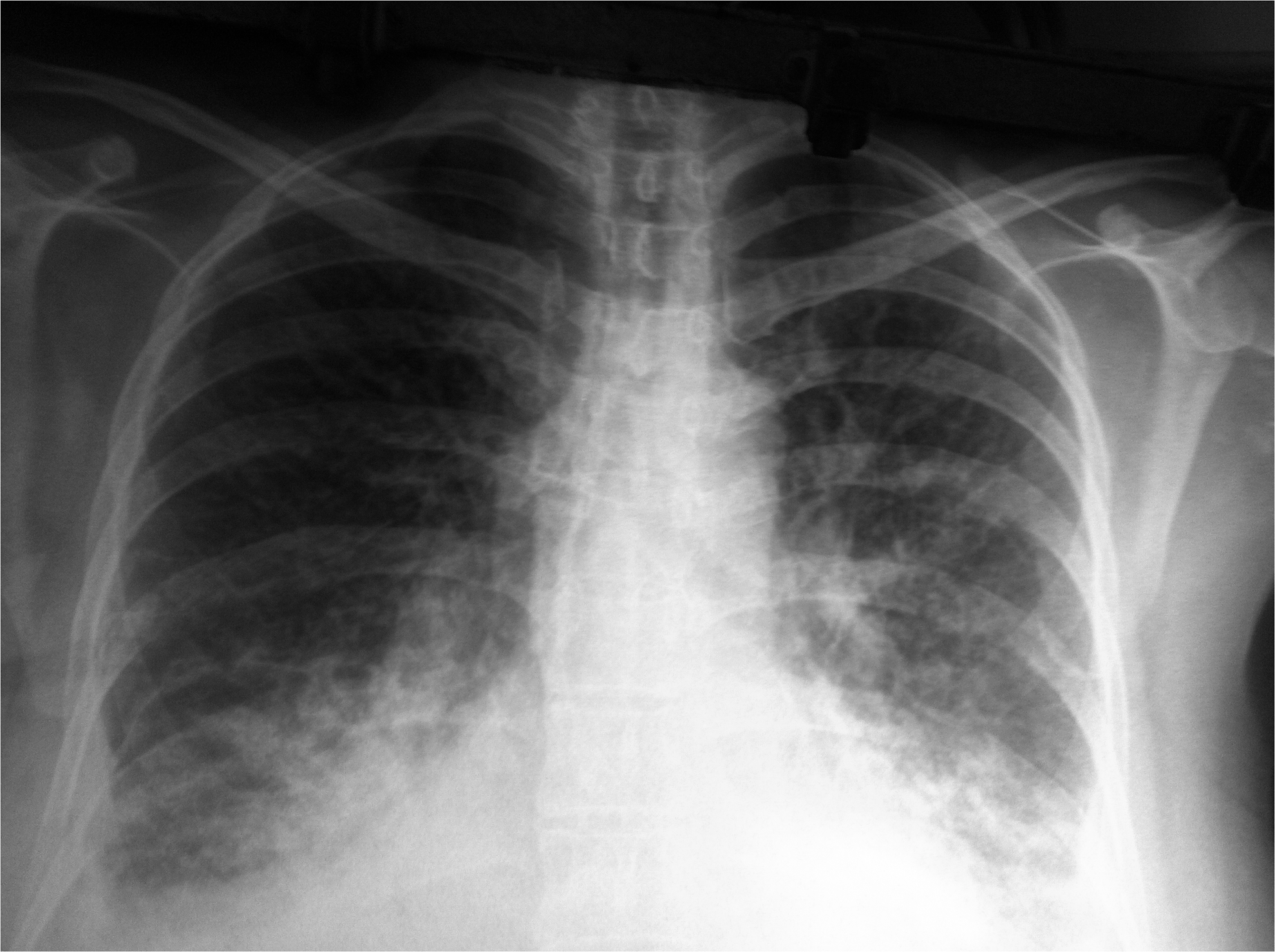
Chest radiograph showing acute respiratory distress syndrome on day 3 after antimalarial treatment.
ND, not determined.
The patient's condition deteriorated rapidly and she was intubated because of ARDS (PaO2/FiO2 <200, compatible radiographic signs, no clinical evidence of elevated cardiac filling pressures). There was no evidence of a bacterial co-infection (negative blood cultures). The patient was treated with intravenous quinine and doxycycline as for severe malaria. She soon became afebrile and 3 days later she was extubated. She was then treated with primaquine (30 mg/day) for 14 days to eradicate liver hypnozoites. She was discharged on day 13 in a very good clinical condition with improved laboratory tests.
Discussion
The case presented herein highlights the potential for occurrence of severe P. vivax malaria in otherwise healthy nonimmune individuals. Another relevant study by Danis et al. reported 20 cases of P. vivax malaria in Greek citizens with no travel history to malaria endemic countries and 16 additional cases in immigrants from endemic countries, which all occurred between May and September, 2011, in Greece (Danis et al. 2011). Among the total 36 P. vivax malaria cases, one, who had serious underlying cardiopulmonary co-morbidity, developed ARDS and died, whereas three additional cases presented central nervous system complications but recovered. The case presented herein is referred by Danis et al. as the one admitted to the intensive care unit (Danis et al. 2011).
According to the official data reported by the Hellenic Center of Disease Control and Prevention, the total number of autochthonous P. vivax cases in the epidemic area around the Evrotas River in 2011 was 34. The case presented herein and the ARDS case reported by Danis et al. both acquired malaria in this area. Thus, the frequency of ARDS among autochthonous P. vivax malaria was 5.9% [95% Fischer exact confidence interval (CI) 0.72–19.7%]. This is comparable with the frequency reported in another study, where ARDS developed in 1 out of 38 (2.6% [0.06%–13.8%]) P. vivax malaria cases that occurred among US military personnel deployed to Afghanistan (Kotwal et al. 2005, Taylor et al. 2012).
Over the past decade, there have been increasing reports of severe P. vivax malaria cases. Although such reports have initially been perceived with skepticism due to the possibility of a misdiagnosis of or a co-infection with P. falciparum, the ability of P. vivax to cause severe malaria has now firmly been established (Kochar et al. 2009, Price et al. 2009). Apart from pulmonary complications, P. vivax has also been associated with both sequestration-related and nonsequestration-related complications, including severe anemia, jaundice, thrombocytopenia, cerebral manifestations, shock, bleeding, and renal failure (Bassat and Alonso 2011).
The detailed characteristics of patients developing ARDS in association with P. vivax malaria have only rarely been described in the medical literature. In the case presented herein, severe pulmonary involvement became evident on the third day after the administration of antimalarial therapy, while mixed infection with P. falciparum had been ruled out. Such severe pulmonary complications usually appear from a few hours to 8 days after the initiation of antimalarial treatment, triggered by a potential exacerbation of inflammatory responses in the lung associated with parasite killing (Anstey et al. 2007). This results in progressive alveolar–capillary dysfunction, enhanced by excessive cytokine release, despite a low parasite burden. However, severe pulmonary symptoms can also appear before the initiation of antimalarial therapy. Intravascular pulmonary sequestration or trapping of leukocytes is another possible contributing mechanism (Anstey et al. 2007). Recent data suggest that P. vivax-infected red cells can cytoadhere to endothelial cell ligand chondroitin sulfate A, which is expressed in the lung (Anstey et al. 2007). Yet, to date, P. vivax–parasitized erythrocytes have not been documented in humans to sequester within the pulmonary microvasculature (Taylor et al. 2012).
ARDS can be one of the most serious complications of P. vivax malaria in terms of mortality, particularly when associated with multiorgan involvement, or when facilities for mechanical ventilatory support are lacking (Kochar et al. 2009, Taylor et al 2012). ARDS should be distinguished from other causes of respiratory distress in malaria cases, which primarily include metabolic acidosis, concomitant pneumonia, and severe anemia (particularly in children). In the case presented herein, ARDS developed posttreatment, in temporal association with clinical deterioration, consisting mainly of worsening jaundice, thrombocytopenia, and anemia, but the patient nevertheless survived.
In differential diagnosis, the above laboratory abnormalities could have been attributed to side effects of mefloquine therapy. Mefloquine has also rarely been associated with drug-induced pneumonitis (with or without eosinophilia), which may necessitate the administration of corticosteroids (Soentjens et al. 2006). In our case, the acute and concurrent presentation of the above manifestations as well as their rapid resolution with the use of supportive measures only indicate their association with a systemic inflammatory response syndrome, triggered by the dying parasites. Mefloquine has a very long half-life and more common or characteristic side effects, such as gastrointestinal and neuropsychiatric ones.
It is difficult to assess the exact incidence of severe P. vivax malaria, given the heterogeneity between the relevant studies. Still, in regions where P. vivax is endemic, it can compare with or even outnumber P. falciparum as the cause of severe malaria (Tjitra et al. 2008). A potential explanation why P. vivax has historically been disregarded as a potential cause of severe malaria could be that the case-fatality rate remains rather low, even when complications occur (Naha et al. 2012). Still, there are increasing reports attributing a substantial case-fatality rate to P. vivax malaria (Price et al. 2009). An alternative, more worrisome, relevant explanation might be that the virulent potential of P. vivax is increasing. This has been attributed to the relatively high genetic diversity among P. vivax strains, as a result of the potential for recombination between different clones that can be present simultaneously in a single host (Arnott et al. 2012). Moreover, increasing virulence might be associated with the acquisition of chloroquine resistance (Price et al. 2009).
The risk factors for the development of severe P. vivax malaria have not been clearly established (Bassat and Alonso 2011). The traditional risk factors for severe P. falciparum malaria might also apply to P. vivax malaria (Barcus et al. 2007). Individuals from nonendemic areas could be more susceptible than those from endemic areas, although the level of immunity in the community typically attained in the latter areas is usually low, due to a relatively low transmission rate (Mendis et al. 2001). Different immune responses, which are thought to be associated with greater severity of illness, have been observed in native-born compared with foreign-born returning travelers with malaria from all species in Canada (McMullin et al. 2012). Delayed disease diagnosis leading to delayed administration of specific treatment can also be common for malaria occurring in individuals in nonendemic countries, as highlighted by the case presented herein. The patient's age could also be a determinant of the type of complications associated with P. vivax malaria (Genton et al. 2008, Tjitra et al. 2008).
Conclusion
The risks associated with the emergence of autochthonous P. vivax transmission in a previously malaria-free area for the population may not be negligible. The absence of pre-existing immunity among the natives, coupled with a low level of suspicion of malaria between the treating and laboratory physicians, could be particular determinants of an adverse patient outcome in the above setting. Further studies are needed to accurately quantify the risk for severe malaria associated with P. vivax infection.
Footnotes
Author Disclosure Statement
The authors have no conflict of interest to declare.