
Abstract
To estimate the prevalence of West Nile virus (WNV) immunoglobulin G (IgG) antibodies in residents of northern Greece before the large outbreak of 2010, stored serum samples collected during 2003–2004 from 626 apparently healthy residents of northern Greece were tested. A seroprevalence of 0.62% was detected, with no statistically significant differences among the various prefectures, gender, and age groups, suggesting that the lineage 2 WNV strain that caused the outbreaks for 3 consecutive years was introduced recently. Data from the present study can be used as a threshold in future comparisons with respective data after the outbreaks to estimate and assess the public health impact, as well as for WNV evolutionary studies.
Introduction
In Greece, the first human cases of WNV infection were documented in the summer of 2010, signaling the initiation of a substantial outbreak of 262 clinical cases (197 neuroinvasive, 35 fatal) (Papa et al. 2010a, Danis et al. 2011). The outbreak reoccurred in 2011 and 2012, with 101 (75 neuroinvasive, 9 fatal) and 161 (109 neuroinvasive, 18 fatal) cases, respectively (Hellenic Centre for Disease Control and Prevention 2012, Papa 2012). During a serological survey conducted in the 1960s, WNV antibodies were detected in 1.2% of 1128 healthy individuals (Pavlatos and Smith 1964), whereas in a subsequent one in the 1980s, WNV antibodies were detected in approximately 1% of healthy farmers and shepherds (Antoniadis et al. 1990). A serosurvey in animals in the 1970s identified WNV antibodies in 8.8% of sheep, 8.7% of goats, 3.9% of cattle, 1.4% of pigs, 20.4% of horses, and 24.5% of birds (Koptopoulos and Papadopoulos 1980). The authors of the above studies concluded that WNV or a related flavivirus was circulating in an endemic cycle in Greece. WNV RNA was not detected in cerebrospinal fluid (CSF) of the 115 patients with aseptic meningitis in 2005 and in blood donations from blood banks in Athens in 2006–2007 (Kantzanou et al. 2009). During March–May, 2007, WNV-neutralizing antibodies were detected in 1.02% of the human population in the Imathia prefecture, in northern Greece (Papa et al. 2010b). This area was the focus of the outbreak in the summer of 2010 (Papa et al. 2010a). The aim of the present study was to estimate retrospectively the prevalence of WNV antibodies in residents of the broader area of northern Greece before the outbreak of 2010, providing a threshold for future studies to assess the public health impact.
Materials and Methods
Serum samples from 646 (320 males, 49%) apparently healthy residents of rural and urban areas of 12 prefectures of northern Greece were included in the study. The collection was performed during 2003–2005 for seroprevalence studies on tick-borne encephalitis virus (TBEV). Oral informed consent was obtained from all participants (Pavlidou et al. 2007). All age groups were included almost equally in the study, with ages ranging from 8.5 months to 89 years (median 55 years). Sera were stored at −70°C.
The samples were tested for anti-WNV immunoglobulin G (IgG) antibodies using an “in-house” indirect immunofluoresence assay (IFA). The assay was performed on spot slides containing Vero E6 cells (ATCC CRL 1586) infected with WNV Eg101 strain. Sera were tested by IFA with fluorescein-labeled anti-human IgG immunoglobulin at an initial dilution of 1:16, along with a positive and a negative control on each slide. Samples that tested positive at the initial dilution were tested in four additional two-fold dilutions. All samples positive by IFA were tested for the presence of anti-WNV IgM and IgG antibodies by enzyme-linked immunosorbent assay (ELISA), using a commercial kit (WNV IgM capture DxSelect and WNV IgG DxSelect, respectively, Focus Diagnostics Inc, Cypress, California). To exclude cross-reactivity, the positive samples were tested for the presence of IgG antibodies against TBEV and Dengue virus.
Statistical analysis to assess the statistically significant differences in prevalence rates among age groups, gender, and prefectures was performed by applying the Pearson chi-squared test and binary logistic regression using the IBM SPSS package for Windows, v.19.0. A p value less than 0.05 was considered significant.
Results
In total, anti-WNV IgG antibodies were detected by IFA in four out of 646 (0.62%) samples tested. The four samples were positive also in WNV IgG ELISA, all being negative for IgM. The IFA IgG titer was 160 in the residents from Evros, Kilkis, and Pella prefectures, whereas in the resident from Serres prefecture it was 320. No cross-reactivity was seen with TBEV and Dengue virus. The prevalence of IgG WNV antibodies per prefecture and age group is seen in Table 1. No statistical difference was observed among the different age groups, nor between males and females. The prevalence ranged from 0% to 1.92% (Fig. 1), with no significant difference among prefectures (p<0.05).
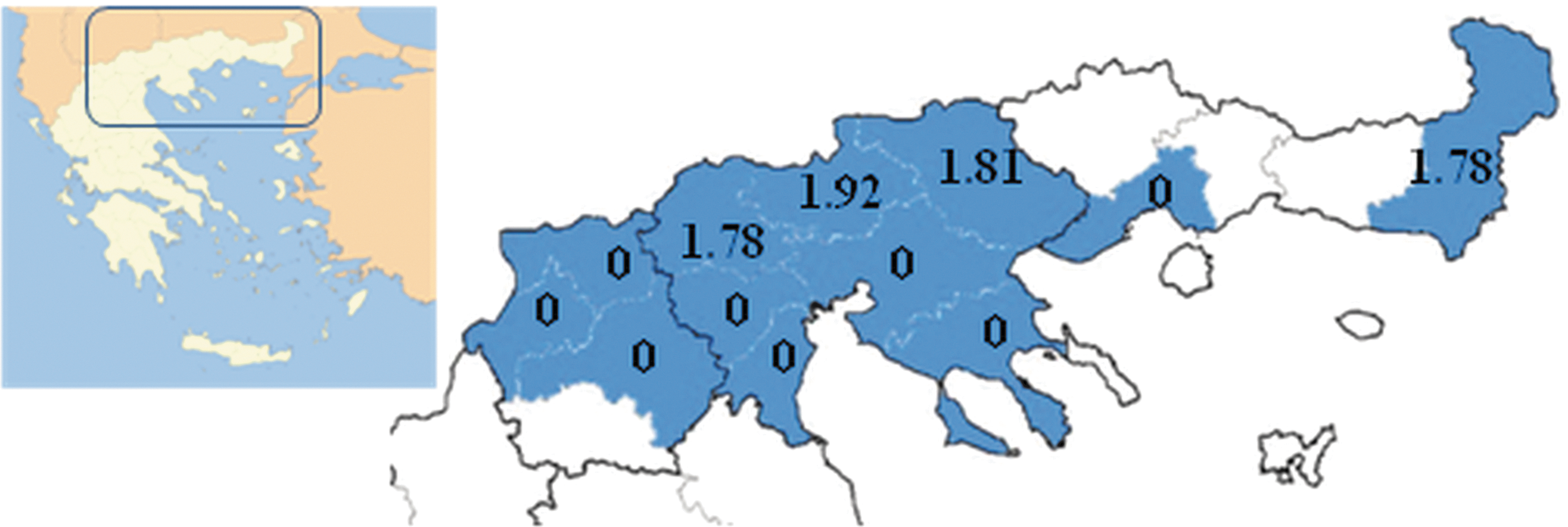
Prevalence of immunoglobulin G (IgG) antibodies in various prefectures of northern Greece, 2003–2005 (before the outbreak of 2010). Color images available online at
IgG, immunoglobulin G; WNV, West Nile virus; M, male; F, female; pos, positive.
Discussion
This is the latest large-scale survey on the prevalence of human WNV antibodies in Greece prior to the outbreak of 2010. The low seroprevalence (0.62%) detected, being even lower than in previous similar studies in the country, suggests that the outbreak in 2010 was caused by a recently introduced strain. Furthermore, all CSF and serum samples from human CNS infections sent to the National Reference Centre for Arboviruses in Thessaloniki in summer and autumn of 2009 produced negative results for WNV IgM and IgG antibodies (unpublished data). The low prevalence of anti-WNV antibodies detected in the present study also indicates the large number of susceptible human population in the area, which might play an additional role for the large outbreak that followed.
Genetic studies showed that the Greek strain (Nea Santa-Greece-2010) shows the closest genetic relationship to the lineage 2 WNV strain detected in Hungary in 2004, however with a few, and probably significant mutations, like the H249P in the NS3 protein (Papa et al. 2011). It is of interest that the lineage 2 strains detected in various parts of Italy, including Sardinia, are similar to the Hungarian rather than the Greek strain (Bagnarelli et al. 2011, Savini et al. 2012, Savini et al. 2013). Whether the outbreak in Greece was a result of southward or northward spread, meaning whether the Greek strain resulted during the evolution of the Hungarian strain in its way to the south or represents an independent introduction from Africa by migratory birds, remains to be elucidated, although a locally acquired mutation cannot be excluded. In any case, the present data can serve as threshold for future studies aiming to estimate the exact increase level in seroprevalence due to the outbreak. Then, by extrapolation from the number of diagnosed meningoencephalitis cases in the specific regions, the total number of WNV infections during the outbreak can be estimated and the public health impact of the epidemic can be assessed (Mostashari et al. 2001).
A study during 2008–2009 in the district of Ferrara, northeastern Italy, where WNV cases have been reported since 2008, showed a seroprevalence rate of 0.69% among blood donors (Pierro et al. 2011), whereas a study in the nearby metropolitan area of Milan, which is considered nonendemic, showed that the WNV seroprevalence among blood donors increased from 0% in 2009 to 0.57% in 2011(Gaibani et al. 2013). Such studies are good indicators and serve as background for risk assessment and surveillance studies.
Concerning Greece, the virus was most probably circulating for 1–3 years before the outbreak in an enzootic cycle between birds and mosquitoes, with few, if any, asymptomatic or mild (thus undetected) human infections. The extremely high temperatures in spring and summer of 2010, together with the increased rainfalls, may have played a role in the outbreak. A recent analysis revealed significant relationships between the spring–summer temperatures in 2010 and West Nile fever cases in Russia, Romania, Greece, Turkey, and Israel, countries with the largest number of cases (Paz et al. 2013).
Conclusion
The Greek outbreak seems to be the result of a recent introduction of a WNV lineage 2 strain and reflects the capacity of WNV to cause outbreaks of major public health significance in previously unaffected areas. Enhanced surveillance activities are required to ensure timely and prompt implementation of appropriate measures to combat the spread of mosquito-borne viruses in general, which is expected to increase in the upcoming years due to climatic changes. Comparative seroprevalence studies in the following years throughout the country will give a further insight into the WNV epidemiology.
Footnotes
Author Disclosure Statement
No competing financial interests exist.