
Abstract
Objective:
We aimed to assess the association between resting heart rate (RHR) and severe infection in children with Crimean–Congo hemorrhagic fever (CCHF).
Methods:
In all, 121 patients under 18 years of age with a laboratory-confirmed diagnosis of CCHF were enrolled in the study. Patients were classified into two groups based on disease severity (severe group and nonsevere group). RHR was measured by electrocardiography (ECG) on admission. Maximum P-wave duration (Pmax), P-wave dispersion (Pd), QRS duration, corrected QT interval, and QT dispersion were also measured.
Results:
Mean age was 11.4±3.9 years and 84 patients were male. Twenty-six patients were classified as severe. Patients in this group had a higher RHR (103.6±10.4 vs. 80.5±8.1, p=0.001) than those with nonsevere disease. There was no difference in Pmax, Pd, QRS duration, QTcmax, or QTc dispersion. The optimal cutoff value of RHR to predict disease severity was>96 beats per minute (bpm), with 70.6% sensitivity and 50.1% specificity. Bleeding, thrombocytopenia (≤80×109/L), elevated aspartate transaminase (AST) (>208 IU/ L), elevated alanine transaminase (ALT) (>87 IU/ L), elevated lactate dehydrogenase (LDH) (>566 IU/L), long activated partial thromboplastin time (aPTT) (>42 s), and increased hospitalization days were more frequent in patients with RHR >96 bpm. Multivariate logistic regression analysis revealed low platelet count (<80×109/L), long aPTT (>42 s), high LDH (>566 IU/L), and elevated RHR (>96 bpm) as independent risk factors for severe disease.
Conclusions:
We conclude that elevated RHR was significantly associated with severe disease in children with CCHF, thus offering the potential to identify patients with increased risk.
Introduction
C
The most important component in the management of CCHF is supportive treatment, which includes intensive monitoring of administered platelets, fresh frozen plasma, and erythrocyte preparations (Whitehouse 2004, Ozkurt et al. 2006, Yilmaz et al. 2010). Because severe cases need to be treated with antiviral drugs and supportive care, prediction of the severity of the infection is a first step in deciding whether to initiate treatment (Ergonul et al. 2004, Ergonul et al. 2006). Involvement of the heart in adult patients has been described previously, and cardiac involvement may have a role in the pathogenesis of CCHF and may also influence the outcome (Engin et al. 2009). However, there is insufficient data about cardiac involvement in CCHF from postmortem studies, and little is known about the effect of CCHF virus on the heart. Elevated resting heart rate (RHR) has shown to be a robust risk factor for both fatal and nonfatal cardiac outcomes in populations with and without cardiac disease (Fox et al. 2008, Jouven et al. 2009, Cook et al. 2010). RHR has not previously been evaluated in children with CCHF. Hence we aimed to assess the association between RHR and severe infection in children with CCHF.
Methods
This was a prospective study; 121 patients under 18 years of age with a laboratory-confirmed diagnosis of CCHF were enrolled in the study. The diagnosis of CCHF infection was based on typical clinical and epidemiological findings and enzyme-linked immunosorbent assay (ELISA) tests (anti-CCHF immunoglobulin M [IgM] and IgG antibodies) or on detection of genomic segments of the CCHF virus in sera by RT-PCR in the acute and/or convalescent phase of the disease. Serum samples were sent to the Virology Laboratory of Refik Saydam Hygiene Central Institute, Ankara, Turkey, for microbiological analyses.
The diagnosis of suspected CCHF was based on the presence of an epidemiological risk factor (tick bite or travel to an endemic region, involvement in animal husbandry or farming, contact with the body fluid of a CCHF patient, and individuals with similar complaints in the proximity of a CCHF patient), compatible clinical presentation (fever, malaise, bleeding, acute-onset headache, myalgia/arthralgia, lethargy, nausea/ vomiting, and abdominal pain/diarrhea), and laboratory data consisting of a platelet (PLT) count <150×109/L and/or white blood cells (WBCs) <4×109/L, and elevated levels of transaminases (32-fold normal limits), lactate dehydrogenase (LDH), and creatine phosphokinase (CPK) (Ozkurt et al. 2006, Yilmaz et al. 2009). All patients received appropriate therapy, including supportive care with intravenous fluids, platelet suspension, blood, and fresh frozen plasma transfusion, when indicated. Confirmed CCHF patients were classified into a severe group and a nonsevere group, as previously reported by Cevik et al. (2008). Patients with at least one of the following were considered severe cases: Somnolence, melena, activated partial thromboplastin time (aPTT) ≥60 s, and thrombocyte count ≤20×109/L during their hospital stay. Patients with a previous history of structural heart disease, atrial fibrillation, sustained or symptomatic ventricular dysrhythmias, sinus node or atrioventricular node dysfunction, bradycardia, bronchial asthma, significant renal, hepatic, gastrointestinal disease, or endocrine disorders or patients taking any drugs influencing electrocardiography (ECG) and use of antiarrythmic drugs were not included in the study.
Demographic characteristics, occupation, tick exposure history, incubation time, symptoms, duration between onset of symptoms and admission, clinical findings, and laboratory tests (WBCs, PLT, hemoglobin [Hb], aspartate aminotransferase [AST], alanine aminotransferase [ALT], LDH, CPK, blood urea nitrogen [BUN] and plasma creatinine [Cr], prothrombin time [PT], aPTT, international normalized ratio [INR]) of all patients were recorded on admission. Standard 12-lead ECG readings were obtained simultaneously using a recorder set at 50-mm/s paper speed and calibration of 1 mV/cm in a comfortable supine position. RHR was measured by ECG on admission. ECG recordings were registered after 5 min at rest in a quiet room with a constantly controlled temperature (Palatini et al. 2006). The duration of measurement was 30 s (Vogel et al. 2004). Following the determination of maximum P-wave duration (Pmax) and minimum P-wave duration (Pmin), P-wave dispersion (Pd) was calculated by subtracting the Pmin value from the Pmax value. QT intervals were measured from the beginning of the QRS complex to the end of the T wave, which was defined as return to baseline in each ECG lead (Postema et al. 2008). QTc dispersion (QTcd) was calculated according to the difference between the longest and shortest QT interval measured in each individual ECG lead (Malik et al. 2000). All measurements were repeated by a second investigator who was blinded to the demographic information and therapy.
The study protocol was approved by the local ethics committee. A written informed consent was obtained from all participants.
Statistical analysis
Descriptive statistical analysis was performed for all the studied variables. The data obtained were analyzed for normal distribution using the Kolmogorov–Smirnov test. Nonnormally distributed continuous variables were expressed as medians and compared with a Mann–Whitney U-test. Categorical data were expressed as absolute frequency and percentage. Proportions for categorical variables were compared using the chi-squared test, although the Fisher exact test was used when the data were sparse. Receiver operating characteristic (ROC) curve analysis was performed to identify the optimal cutoff point of RHR (at which sensitivity and specificity would be maximal) for the prediction of disease severity. Areas under the receiver operator curve (AUROC) were calculated as measures of the accuracy of the tests. Sensitivity, specificity, negative predictive values, and positive predictive values were calculated according to ROC curves for RHR. In addition, we used univariate analysis to quantify the association of variables with disease severity. Variables found to be statistically significant in the univariate analysis, as well as potential confounders (age and gender, fever, PLT <80.000/mm3, aPTT >42 s, AST >208 IU/L, ALT >87 IU/L, LDH >566 IU/L, and RHR >96 bpm), were used in a multivariate logistic regression model with forward stepwise method to determine independent prognostic factors of disease severity. The results of the analysis were presented as p values, odds ratio (OR), and 95% confidence interval (95% CI). A p value of 0.05 was considered statistically significant. Statistical analyses were performed using SPSS 11.0 statistical package (SPSS Inc., Chicago, IL).
Results
The demographic, clinical characteristics, and electrocardiographic findings of severe and nonsevere CCHF cases are shown in Table 1. Mean age was 11.4±3.9 years and 84 out of 121 patients were male. All patients survived and were discharged after a median of 9 (7–10) days. Twenty-six (21.5%) patients were classified as severe. The age, gender, initial complaints (fever, nausea-vomiting, myalgia, and headache), and the duration between onset of symptoms and admission were similar between the groups. Fever, myalgia, headache, and nausea-vomiting were the most common symptoms. The rates of hemorrhage, somnolence, and hospitalization days were significantly higher in severe cases compared with nonsevere cases, and ribavirin treatment was similar in the two groups. On admission, and in comparison to the nonsevere group, patients in the severe group demonstrated significantly lower mean platelet counts, longer mean aPTT and higher mean values for AST, ALT, AST/ALT, LDH, and CPK.
CCHF, Crimean–Congo hemorrhagic fever; PLT, platelet; WBC, white blood cell; Hb, hemoglobin; PT, prothrombin time; aPTT, activated partial thromboplastin time; INR, international normalized ratio; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LDH, lactate dehydrogenase; CPK, creatine phosphokinase; bpm, beats per minute; Pmax, maximum P wave duration; QTcmax, maximum corrected QT interval.
On electrocardiography, all patients had sinus rhythm and none had electrolyte abnormalities, which could cause ECG abnormality during ECG recording. All electrocardiographic parameters were within normal ranges according to age. Patients in the severe group had a higher average RHR (103.6±10.4 vs. 80.5±8.1, p=0.001). There was no difference in Pmax, Pd, PR intervals, QRS durations, QTcmax, or QTcd. There was no change in ST segments or T waves. Intra- and interobserver variability for ECG parameters were assessed in 18 randomly chosen patients and varied from 3.2% to 4.6%.
According to the ROC curve analysis, the optimal cutoff value of RHR to predict disease severity was >96 bpm, with 70.6% sensitivity (95% CI 0.457, 0.881), 50.1% specificity (95% CI 0.408, 0.732), 56.4% positive predictive value, and 75.2% negative predictive value (AUROC 0.753, 95% CI 0.595–0.852) (Fig. 1). The patient cohort was divided at the cutoff point of RHR into two groups. The patients in the upper RHR (>96 bpm) group did not differ from those in the lower RHR (≤96 bpm) group at the initial evaluation in terms of age, gender, fever, days from first symptoms to admission, symptoms, and ribavirin use. Bleeding, thrombocytopenia (≤80×109/L), elevated AST (>208 IU/ L), elevated ALT (>87 IU/ L), elevated LDH (>566 IU/L), long aPTT (>42 s), requiring platelet transfusions, and increased hospitalization days were significantly more frequent in the upper RHR group. RHR was positively correlated with disease severity (r=0.713, p=0.003). With respect to the other prediction factors, RHR was positively correlated with AST (r=0.627, p<0.001), ALT (r=0.605, p<0.001), LDH (r=0.635, p=0.047), aPTT (r=0.751, p<0.001), and hospitalization days (r=0.678, p<0.001) in the severe group. Also, RHR was negatively correlated with platelet count in the severe group (r=−0.763, p<0.001). Additionally 32 (70%) of the upper RHR group and 4 (5%) of the lower RHR group required platelet transfusion (p<0.001). General characteristics of patients stratified by cutoff value of resting heart rate are shown in Table 2. Low platelet count (<80×109/L), prolonged aPTT (>42 s) and high AST (>208 IU/L), ALT>87 IU/L, LDH (>566 IU/L), and elevated RHR (>96 bpm) were predictors for severity using univariate analysis. Our multivariate logistic regression model with a forward stepwise method using the cutoff values predetermined for severe patients, revealed low platelet count (<80×109/L), prolonged aPTT (>42 s), and high LDH (>566 IU/L), and elevated RHR (>96 bpm) as independent risk factors for severe disease. Results of the univariate and multivariate logistic regression analyses for the prediction of severe CCHF are listed in Table 3.
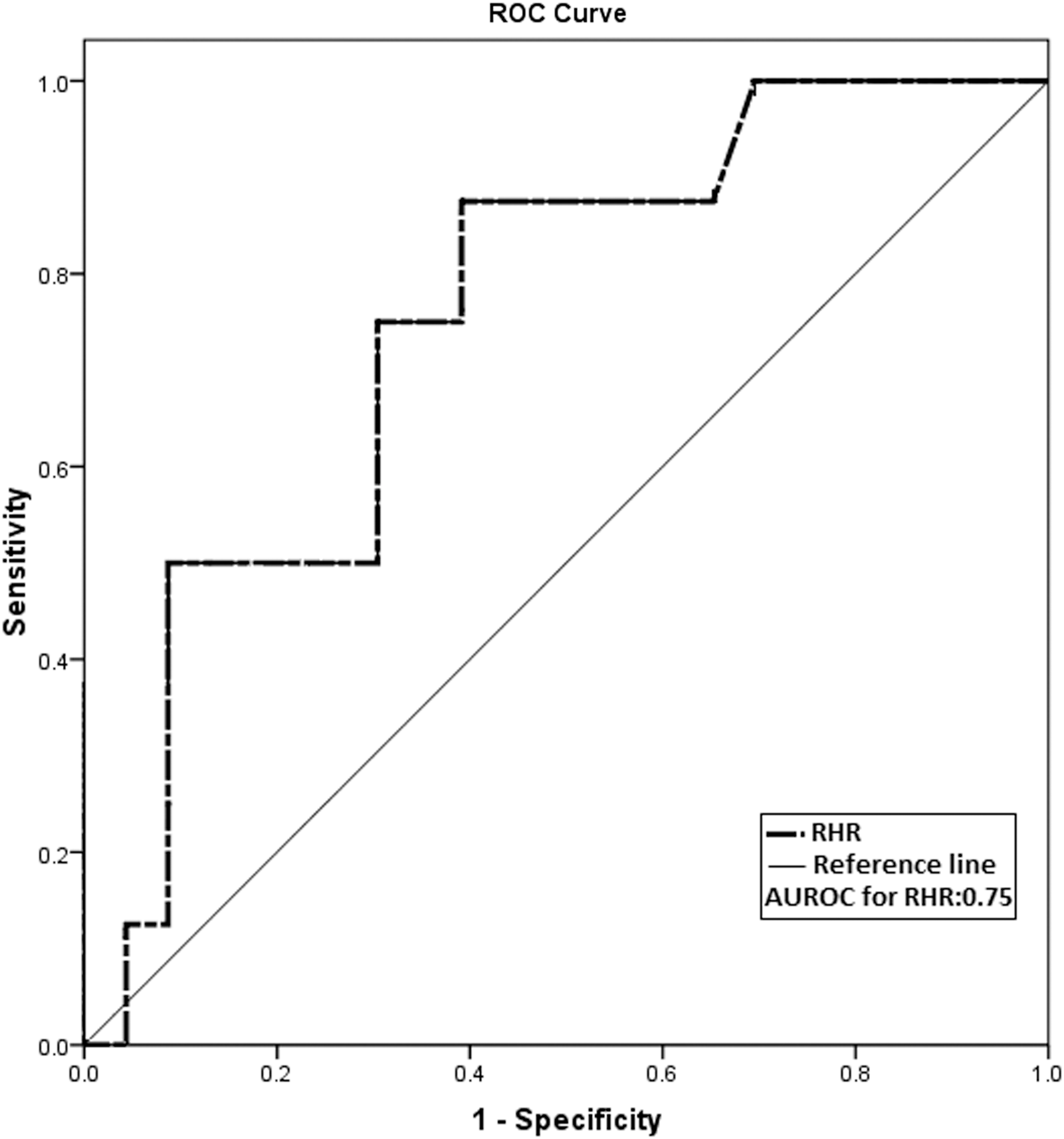
Receiver operating characteristics (ROC) of resting heart rate (RHR). AUROC, area under the receiver operating curve.
RHR, resting heart rate; bpm, beats per minute; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LDH, lactate dehydrogenase; aPTT, activated partial thromboplastin time.
Age and gender, fever, PLT <80×109/L, aPTT >42 s, AST >208 IU/L, ALT >87 IU/L, LDH >566 IU/L, and RHR >96 beats per minute (bpm) were entered into the multivariate logistic regression model.
CCHF, Crimean–Congo hemorrhagic fever; OR, odds ratio; CI, confidence interval; PLT, platelet; aPTT, activated partial thromboplastin time; LDH, lactate dehydrogenase; RHR, resting heart rate; bpm, beats per minute; WBC, white blood cell; BUN, blood-urea-nitrogen; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
Discussion
In this study, we analyzed the relevance of RHR for disease severity in children with CCHF, and we conclude that elevated RHR was significantly associated with severity and can potentially be used to identify subjects with an increased risk.
CCHF involves many organ systems (Whitehouse 2004). After detection of the disease in Turkey in 2002, CCHF has become endemic in our country and large outbreaks have been seen in the service area of our hospital during the spring and summer seasons. The severe form of CCHF is characterized by hemorrhage, disseminated intravascular coagulation, vascular dysfunction, and shock (Whitehouse 2004, Ergonul et al. 2006). The high mortality rates in the literature underline the importance of predictive criteria to determine the severity of CCHF using laboratory results obtained on admission (Ergonul et al. 2006, Cevik et al. 2008). Severity criteria were previously defined by Swanepoel et al. (1989), but there is no such classification for pediatric patients. Ergonul et al. reported hemorrhagic complications in severe cases (Ergonul et al. 2004, Ergonul et al. 2006). Cevik et al. also reported that hemorrhages such as ecchymosis, hematemesis, melena, and gingival bleeding were the commonest clinical findings in fatal cases (Cevik et al. 2008). In our study, planned in the light of those studies, where CCHF patients were classified into two groups based on disease severity, 16.5% of our patients exhibited hemorrhage and 29.7% were given platelet transfusion. No mortality was observed in our patients. The fact that we had no fatal case may be due to admission of patients in the early stages of infection due to awareness of the disease, supporting therapy, and the prompt supply and transfusion of blood and blood products.
Despite increasing knowledge about hemorrhagic fever viruses, the specific mechanisms underlying the pathogenesis of CCHF infection have not been explained clearly (Whitehouse 2004, Ergonul 2006, Engin et al. 2009). Mononuclear phagocytes, hepatocytes, and endothelial cells are major targets of CCHF virus during the course of the infection (Burt et al. 1997). It has been demonstrated that hemorrhagic fever viruses can cause cardiac involvement in experimental and clinical studies (Oubina et al. 1986, Burt et al. 1997). Direct invasion of the heart muscles by the virus or endothelial damage of cardiac structures may have a role in cardiac involvement. A histopathological study by Burt et al. showed congestion and interstitial edema in the heart tissues of one fatal CCHF case (Burt et al. 1997). The observation of cardiac congestion and edema in that fatal CCHF case may support cardiac involvement in CCHF infection. A recent study by Engin et al. showed that CCHF virus impairs cardiac functions in adults (Engin et al. 2009). In that study, Engin et al. showed that severe and fatal CCHF cases have impaired cardiac functions, which may be associated with fatality in CCHF infection. In another study, cardiac involvement was recognized with electrocardiographic abnormalities and abnormal wall motion detected by early echocardiography (Gul et al. 2011, Yilmaz et al. 2011). The wall motion abnormalities might be due to involvement of the myocardium by the CCHF virus and/or myocardial endothelial injury and might contribute to the pathogenesis of shock in CCHF and might influence the outcome (Wali et al. 1998, Ergonul 2006, Saggioro et al. 2007).
In our study, the optimal cutoff value of RHR to predict disease severity was >96 bpm, with 70.6% sensitivity and 50.1% specificity. These values can be considered to be low. When RHR combined with aPTT for evaluation, sensitivity was 79.4%, specificity was 68.6%, and AUROC reached a better score (0.914). Also, when RHR combined with platelet count, the sensitivity was 81.6%, the specificity was 70.2%, and AUROC reached a better score (0.920). Therefore, combination of RHR with different markers might give a better sensitivity and specificity.
In our study, we found that RHR was significantly increased in children with severe CCHF. Furthermore, after controlling for confounding parameters, we found that high RHR was associated with severe disease. In addition, parameters associated with disease severity were frequent in the group of patients with elevated RHR. Several studies identified elevated RHR as a predictor of cardiac involvement (Fox et al. 2008, Jouven et al. 2009, Cook et al. 2010). In fact, recent studies have reported that oxidative stress positively affects the sympathetic nervous system activation, which is responsible for the increase of RHR (Hirooka et al. 2010). Alternatively, the myocardial perfusion defect itself could trigger tachycardia in an attempt to improve blood supply to areas of the myocardium with unmet demands. In turn, an elevated heart rate response decreases diastolic and coronary perfusion time and increases the likelihood of ischemic events (Fox et al. 2008, Williams et al. 2012). Indeed, any existing clinical pathology, such as myocardial involvement or endothelial dysfunction caused by CCHF, characterized by an unfavorable oxygen supply–demand imbalance may serve as a tachycardia stimulus that limits cardiac performance (Arnold et al. 2008, Fox et al. 2008, Jouven et al. 2009). The stressed endothelium releases growth hormones and vasoconstrictor peptides (endothelin), which are associated with increased platelet aggregation and a relative deficiency of nitric oxide synthesis (Arnold et al. 2008). All of these factors may facilitate the development of shock in CCHF. However, there is insufficient data about cardiac involvement in CCHF from postmortem studies, and little is known about the effect of the CCHF virus on the heart. Endomyocardial biopsy can be fatal due to the low platelet count in CCHF patients. Further studies are needed to determine the pathogenesis of myocardial involvement in CCHF.
We found very few studies in the literature on electrocardiographic findings in CCHF. A study by Gul et al. showed that CCHF in children involves the heart and that cardiac involvement is more frequent in children than in adults (Gul et al. 2011). In that study, no electrocardiographic abnormalities were detected. In contrast, Yilmaz et al. showed that fatal adult cases had variable degrees of ECG abnormalities (Yilmaz et al. 2011). Particularly, T-wave changes and bundle branch blocks were noted in fatal cases. Electrocardiographies in our patients revealed no abnormality, suggesting that CCHF does not involve the conduction system of children's hearts.
Study limitations
Several limitations of this analysis are noteworthy. First, this study presents data from a tertiary care center. Second, when considered alone, the sensitivity and specificity of RHR to predict severity are relatively low. It was reported in studies evaluating adult patients that sensitivity of aPTT was 67.2% and specificity was 67.4%; sensitivity of platelets was 74.6% and specificity was 52.8%; sensitivity of AST was 71.4% and specificity was 50.6%. Therefore, combination of RHR with different markers might give a better sensitivity and specificity. The cross-sectional design does not offer support to causality statements and, therefore, prospective studies from childhood to adolescence are necessary to describe more accurately the longitudinal relationship between RHR and disease severity in CCHF virus infection.
Conclusions
In conclusion, RHR can be measured easily in routine examination and was significantly associated with disease severity in children presenting to the hospital with CCHF. We conclude that RHR may guide the clinician in identifying cases that may follow a severe course and will contribute considerably to the design, practice and management of supportive therapy, blood and blood products replacement, and intensive care services when required. Further studies are needed to determine the pathogenesis of myocardial involvement in CCHF virus infection.
Footnotes
Acknowledgments
The authors thank Refik Saydam Hygiene Center of Ankara, Turkey, for testing the serum samples.
Author Disclosure Statement
The authors have no conflicts of interest and no funding sources to declare.