
Abstract
Introduction:
Suriname is a country on the northeastern Atlantic coast of South America. It is unique in the sense that different ethnic cultures live together within the country, resulting in high levels of transport of both humans and products between the Asian, African, and European continents as well as the Caribbean. Travel is only one of the many factors present in Suriname contributing to the risk for the emergence or introduction of any infectious disease. Recently, circulation of both chikungunya virus (CHIKV) and hantavirus was reported in areas neighboring Suriname. Here we report a retrospective and prospective study into chikungunya and hantavirus circulation.
Methods:
A chikungunya and hantavirus retrospective serological study was conducted on samples submitted for dengue, leptospirosis, and/or influenza virus diagnostics between 2008 and 2012 to the Bureau of Public Health in Suriname. This was followed by a prospective CHIKV serological and molecular surveillance study until the detection of the first autochthonous CHIKV cases in Suriname in May and June of 2014.
Results:
None of the tested samples showed the presence of CHIKV antibodies in the retrospective serological study. Prospective testing of CHIKV-suspected patients resulted in the detection of the first autochthonous CHIKV cases in Suriname in May, 2015. In one sample, we were able to isolate and sequence the virus. Retrospective testing for the presence of hantavirus antibodies showed a relative high response in both pan-hantavirus enzyme-linked immunosorbent assay (ELISA) and immunofluorescence assay (IFA). However, neutralization tests did not yield any evidence for infection with either Seoul or Andes hantavirus.
Conclusion:
Here we report the presence of CHIKV in the republic of Suriname and the first serological indication of hantavirus infections in symptomatic patients.
Introduction
T
The Bureau of Public Health in Suriname (BOG) has put much effort in the control of two endemic mosquito-borne diseases, yellow fever and malaria, resulting in a strong reduction and almost no reported cases of these diseases in the domestic areas in the past decennium (BOG Annual Report). Despite sporadic cases of malaria in the Amazons (tropical rainforest in the inlands of Suriname), both diseases are now successfully controlled, resulting in hardly any human cases reported the past 10 years. However, sporadic cases of Mayaro virus have been reported in the literature (Hassing et al. 2010). In addition, dengue is endemic in Suriname, while an epidemic of chikungunya virus (CHIKV) is currently ongoing in the Caribbean and Americas. The first local transmission of CHIKV in the New World, in this case the Caribbean, was reported from the Saint Martin Island in December of 2013 (Staples and Fischer 2014). As of January 30, 2015, a total of 1,135,892 cases have been reported in the Americas, of which 24,320 have been confirmed by RT-PCR, immunoglobulin M (IgM) immunofluorescence assay (IFA) or a four-fold increase in CHIKV-specific IgG antibodies (Pan American Health Organization 2015). Next to fever, patients with CHIKV often show (poly)arthralgia, which is usually symmetric and bilateral. Arthralgia can be very severe, and patients could have a long recovery, resulting in a serious burden of disease.
Besides mosquito-borne diseases, rodent-borne diseases like leptospirosis are also endemic in Suriname. Furthermore, the circulation of hantaviruses in adjoining countries might be indicative for circulation of hantaviruses in Suriname as well (de Araujo et al. 2015). Hantaviruses are often neglected, emerging viruses. Both unawareness and difficulties in both the clinical and laboratory diagnosis contribute to misdiagnosis of hantavirus cases (Goeijenbier et al. 2014). Pathogenic hantaviruses are able to cause two types of disease in humans, hemorrhagic fever with renal syndrome (HFRS) in Europe and Asia and hantavirus cardiopulmonary syndrome (HCPS) in North and South America (Figueiredo et al. 2014). In South America, many New World hantaviruses are able to cause often clustered and small outbreaks of HCPS, of which Andes virus (ANDV) seems the most widespread (Matheus et al. 2010, Montoya-Ruiz et al. 2014, Munoz-Zanzi et al. 2015). Furthermore, another country neighboring Suriname on the southern border, Brazil, has shown the highest number of hantavirus outbreaks in recent years and reservoir species have been identified in Akodon and Oligoryzomys species (Oliveira et al. 2014, Teixeira et al. 2014). Furthermore, the worldwide migration of rats resulted in the introduction of the Old World hantavirus Seoul (SEOV) in South America that is able to cause HFRS in humans (Iversson et al. 1994, Lin et al. 2012).
Currently, most of the diagnostics for (viral) infections are performed at the central laboratory of the Bureau of Public Health in Suriname. Starting from 2008, samples and clinical data have been stored from patients for which dengue, leptospirosis, or influenza tests were negative, for future use in retrospective studies into the presence of (newly) emerging infectious diseases. Here we aimed to gain insight in the emergence of CHIKV in Suriname through retrospective analysis of samples collected in the period 2008–2012 and prospective analysis of samples collected in 2014. In addition we investigated the possibility of hantavirus infection in patients with no adequate diagnosis at the time of disease in Suriname.
Materials and Methods
Study design and study site
This study was executed in Paramaribo, at the central laboratory, Department of Virology, Bureau of Public Health. Paramaribo is the capital and largest city of Suriname, located in the northern part of the country at the banks of the Suriname river close to the North Atlantic coast. The laboratory is the major diagnostic center in Suriname. A CHIKV and hantavirus retrospective serological study was conducted, followed by a prospective CHIKV serological and molecular surveillance study until we detected the first autochthonous CHIKV cases in Suriname in May and June of 2014.
CHIKV serology
CHIKV IgM and IgG serology was tested by use of an in-house IFA and commercially available IFA (Euroimmun, Germany). Serum samples were diluted 1:10 and 1:100. CHIKV diagnosis was confirmed in the laboratory of Erasmus MC, Rotterdam, The Netherlands, which is a World Health Organization reference laboratory for arbovirus diagnostics.
CHIKV detection by real-time PCR
The presence of CHIKV in patient serum samples was determined by qRT-PCR in the secondary laboratory in Rotterdam, The Netherlands, by detection of the envelope protein 1 (E1) gene (Laurent et al. 2007). Briefly, CHIKV RNA was extracted from 100 μL of serum using the MagNAPure LC robotic system and MagNA Pure LC Total Nucleic Acid Isolation Kit (Roche, Germany). The presence of viral RNA was measured with a real-time qRT-PCR assay (TaqMan®Fast Virus 1-Step Master Mix, Invitrogen, Life Sciences) using Applied Biosystems® 7500 Real-Time PCR system.
CHIKV isolation and detection by electron microscopy
Patient sera, with a positive result in the CHIKV real-time PCR, were diluted 1:100 in medium and added onto a 70–80% monolayer of C6/36 insect cells and incubated for 60 min at 30–C. The supernatant was discarded and cells were washed once and incubated with fresh Leibovitz-15 medium supplemented with 5% heat inactivated fetal bovine serum (HI-FBS), 10% tryptose phosphate broth, 0.75% sodium bicarbonate, 10 mM HEPES buffer, 100 U penicillin, 100 μg/mL streptomycin, and 2 mM
Sequence and phylogenetic analysis of CHIKV E1 gene
A PCR targeting a portion of the E1gene was performed for one virus isolate (Supplementary Data). PCR products were separated on a 1% agarose gel, and bands of the correct size were collected for DNA gel extraction using a MinElute Gel Extraction Kit Protocol (Qiagen, USA). Amplicons were purified and sequenced using the Sanger method and the BigDye Terminator v3.1 Cycle Sequencing Kit on an ABI Prism 3130XL Genetic Analyzer sequencer (both from Life Technologies). The phylogenetic tree was constructed using 800 nucleotides of the CHIKV E1 gene. Sequences were aligned using MUSCLE (v. 3.7), and the phylogenetic tree was reconstructed using the maximum likelihood method implemented in the PhyML program (v. 3.0). Reliability for internal branch was assessed using the bootstrapping method (100 bootstrap replicates). All software was used via
Hantavirus serology
Sera were screened using pan-hantavirus IgG and IgM DxSelect ELISA Kits (Focus Diagnostics, USA). These enzyme-linked immunosorbent assays (ELISAs) are used for testing a broad range of hantaviruses, although there are variations in sensitivity and specificity for each specific hantavirus (Goeijenbier et al. 2014). According to the manufacturer's data, both tests were compared with a reference in-house ELISA by external investigators. For Suriname, the performance of these ELISAs in detecting New World hantaviruses and, potentially, SEOV, is of importance. For New World hantavirus infections, the IgM ELISA sensitivity is reported to be 100% in a small cohort (11/11 samples from Andes virus patients tested positive), and for the IgG ELISA this was 60% (3/5 samples from Andes virus patients tested positive). On the basis of SEOV focus reduction neutralizing test (FRNT)-positive samples, the sensitivity was 50% (11.8–88.2%) in the IgM ELISA and 95% (54.1–100%) in the IgG ELISA (Focus Diagnostics 2008).
ELISA IgM-positive or equivocal sera were tested by IFA using commercial slides, Euroimmun Hantavirus Mosaic 1 (Euroimmun, Germany). This test is based on biochip slides coated with Puumala (PUUV), SEOV, Dobrava (DOBV), Hantaan (HTNV), Saaremaa (SAAV), and Sin Nombre (SNV) antigens. Samples were pretreated with Eurosorb IgG absorbent (Euroimmun) and subsequently tested in dilutions 1:10 and 1:100 according to the manufacturer's protocol.
Hantavirus FRNT
All samples positive in the pan-hantavirus IgM ELISA and Euroimmun Mosaic IgM IFA were selected for FRNT confirmation. FRNTs for SEOVstrain 80-39 and ANDVstrain Chile-9717869 were carried out as described elsewhere (Lundkvist et al. 1997, Goeijenbier et al. 2014). Diluted sera were mixed with an equal volume of diluted virus containing 30–70 focus-forming units/100 μL. The serum end dilution was 1:40. The mixture was incubated at 37°C for 1 h and subsequently inoculated into wells of six-well tissue culture plates containing confluent Vero E6 cell monolayers. The wells were overlaid with a mixture of agarose and tissue culture medium and incubated for 7–13 days. The agarose was removed from the wells and the cells were fixed. Antibody detection of SEOV- and ANDV-infected cells was done as described elsewhere (Lundkvist et al. 1991). This step was followed by adding peroxidase-labeled conjugate followed by substrate reaction (tetramethylbenzidine), and foci were counted. An 80% reduction in the number of foci, compared with the virus control, was used as the criterion for virus neutralisation titers.
Results
Retrospective analysis of the presence of CHIKV antibodies
To test if CHIKV was already present in Suriname, all samples of patients with symptoms of fever and arthralgia or fever and rash sent to BOG in the period 2008–2012 were tested retrospectively for the presence of CHIKV IgM or IgG by in-house and commercial IFA. In total, 194 samples matched these criteria. Serum was available for 68 of these samples. All samples were nonreactive in the assays except one that showed low reactivity in the in-house–developed CHIKV IgG IFA (positive in 1:10 dilution) drawn from a patient with a 3-day history of fever and rash, but no reactivity was seen in the in-house–developed CHIKV IgM IFA or the commercially available IgM and IgG IFAs.
Prospective surveillance for the introduction of CHIKV in to Suriname
Starting from March, 2014, CHIKV serological and molecular diagnosis was implemented in the diagnostic laboratory at BOG. Physicians in Suriname were informed about the possibility of CHIKV circulation and the availability of diagnostics. On average, eight to 10 samples were tested per week. The first cases testing positive by the IgM in-house–developed IFA were observed in late spring (May, 2014). All positive IFA results, and a random selection of the negatives, were sent for confirmation to a second laboratory. Serological results and clinical data for the first 2 months of prospective CHIKV screening are listed in Table 1. In total, 23 samples tested positive in Suriname of which the secondary laboratory confirmed 10 samples. All negative test results were confirmed in the second laboratory. One sample (no. 19) also tested positive by the RT-PCR for CHIKV. This sample was drawn from a patient presenting with arthralgia, hemorrhage (skin bleeding), and a macopapular rash over the whole body (Table 1).
IgMa and IgGa are the results from the in-house developed chikungunya virus (CHIKV) immunofluorescence assay (IFA).
IgMb and IgGb are the results from a commercially available CHIKV IFA.
Traveled <15 days to the Caribbean.
Sample was drawn >4 weeks after onset of the symptoms.
Originate from one family.
Ig, immunoglobulin; F, female; M, male; Neg, negative.
CHIKV virus isolation, sequence and phylogenetic analyses of the E1 gene and electron microscopy imaging
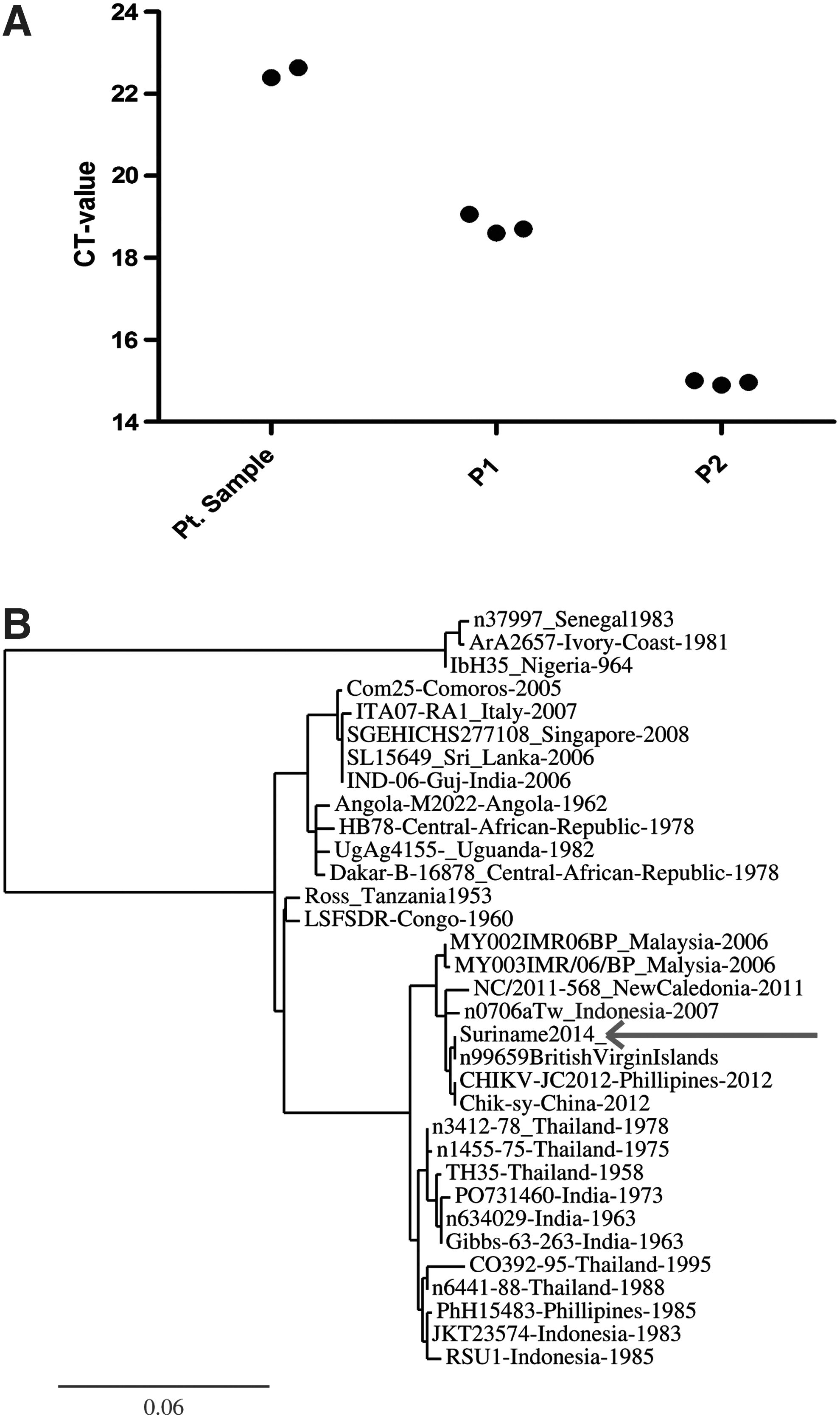
To confirm the molecular detection of CHIKV RNA in the serum of case number 19, this sample was cultured. Figure 1A shows the CT values of the inoculum supernatant after passage number one and of the supernatant after passage number two. The rapid increase in viral RNA suggested replicating CHIKV. This was confirmed by use of electron microscopy. Microscopy of multiple samples drawn from the culture supernatant revealed particles of typical size and shape for that reported from CHIKV particles. Phylogenetic analyses of the 800 nucleotides PCR product showed clustering of the Suriname isolate with isolates of the CHIKV Asian genotype. The closest relationship was seen with the British Virgin Island isolate from 2014 (Lanciotti and Valadere 2014).
(
Serological indication of human hantavirus infections in Suriname on the basis of ELISA and IFA results
In total, 532 samples from patients suspected for leptospirosis or presenting with the combination of symptoms of fever and respiratory complaint or fever and signs of hemorrhage were submitted to BOG. All selected and available sera (n = 264) were screened by pan-hantavirus ELISA. Results are listed in Table 2. IgM testing resulted in 45 samples with an optical density (OD) of >1.1 times the cutoff calibrator, which, according to the manufacturer can be regarded as a positive result. Furthermore, five samples gave an equivocal result in the IgM ELISA (OD 0.9–1.1 times the cutoff calibrator). In total, 18 samples tested positive for the presence of hantavirus IgG antibodies and two samples had an equivocal test result. Samples with a positive result in IgM or IgG ELISA were tested with IFA slides reactive with six different hantaviruses (PUUV, SEOV, HNTV, SNV, DOBV, and SAAV). Results from individual samples are listed in Table 2 together with specific clinical data and additional information. In total, 21 of the 45 samples positive in IgM ELISA were also found positive by IFA testing. Reactivity against both Old and New World hantaviruses in IFA were found in multiple samples. Because recent published work has revealed numerous false-positive samples in a comparable cohort study (Goeijenbier et al. 2014), we decided to repeat the initial ELISA screening by hands of a second investigator unaware of the first results. Twenty-five of the 45 samples (56%) tested positive (OD of >1.1 times the cutoff calibrator) in the second IgM ELISA. Second, IgG ELISA analysis confirmed the presence of IgG hantavirus antibodies in nine of these 18 samples (50%), whereas one equivocal sample tested negative and one positive (Table 2).
IgMa and IgGa, tests performed on site by BOG laboratory workers.
IgMb and IgGb, results of the confirmation test performed by trained laboratory workers.
ELISA results are given in optical density (OD) ratio compared to the cutoff calibrator. A result of >1.1 is considered positive, whereas a result between 0.9 and 1.1 is considered as equivocal (Equi).
ELISA, enzyme-linked immunosorbent assay; IFA, immune fluorescence assay for which an IFA test was used which is able to distinct among six hantaviruses being: ANDV, Andes virus; SEOV, Seoul virus; SNV, Sin Nombre virus; SAAV, Saaremaa virus; HNTV, Hantaan virus; PUUV, Puumala virus (only results positive in 1:100 dilution are given); FRNT, focus reduction neutralizing test; M, male; F, female; Ig, immunoglobulin; Neg, negative; All Pos, all positive; DOBV, Dobrova virus.
Confirmation by FRNT
FRNT was performed on 21 sera with a positive IgM response in the hantavirus mosaic IFA. No samples showed significant neutralizing activity against SEOV or ANDV. Therefore, FRNT did not yield any evidence for infection with either SEOV or ANDV.
Discussion
This study reports the methods and data on the first detection of CHIKV in the Republic of Suriname. Furthermore, our results indicated the occurrence of hantavirus infections of humans in Suriname. The introduction of CHIKV into Suriname follows the large outbreak in the Caribbean, which followed the first reports of introduction of CHIKV to the New World in December of 2013 (World Health Organization 2014). With the magnitude of trade and travel between the Caribbean (the CHIKV outbreak areas) and Suriname, the risk of introduction of CHKV into Suriname was relatively high at forehand. Latest numbers from the National Centre for Statistics (Algemeen Bureau voor Statistiek Suriname [ABS]) show that up to 8% of all people who enter Suriname originate from the Caribbean (Algemeen Bureau voor Statistiek Suriname 2011).
Therefore, local authorities have put much effort in raising CHIKV awareness in (returning) travellers and health care workers in all areas of the country, putting special emphasis on the border areas with neighboring countries. The fact that this eventually failed clearly shows the difficulties in preventing the spread of this emerging arthropod-borne virus. Analysis of the first cases in Suriname shows several interesting observations. First of all, the clinical signs and symptoms, as summarized in Table 1, include the classical symptoms of rash and arthralgia in almost all confirmed patients. Other symptoms include headache, myalgia, arthritis, conjunctivitis, vomiting, and maculopapular rash. Furthermore, hemorrhage occurred in three out of the 11 confirmed CHIKV patients that was most often described as skin bleeding, conjunctival bleeding, or nose bleedings. Although in our cohort this observation is based on a small number of patients, it does show the potency of hemorrhage in the course of infection of CHIKV, something that could be validated by combining the clinical data from the Caribbean outbreak.
Bleeding complications in CHIKV have been reported previously, raising the question of whether CHIKV should be categorized as a (mild) viral hemorrhagic fever pathogen (Weiss et al.1965, Mohan et al. 2010, Nkoghe et al. 2012). Currently, the Pan American Health Organization (PAHO) puts much effort into controlling and monitoring the CHIKV outbreak in the Caribbean and subsequently South America. The case definition used for CHIKV surveillance is formulated by PAHO and the World Health Organization (WHO) as follows: A suspected case is a person with fever >38.5°C and severe arthralgia/arthritis not explained by other medical conditions who is residing or has visited epidemic areas within 15 days prior to onset of symptoms. A confirmed CHIKV case is a suspected patient meeting laboratory confirmation criteria, which are either virus culture, RT-PCR, IgM antibody assay in single sample, or four-fold increase in CHIKV-specific antibody titers IgG (Pan American Health Organization 2015).
Potential problems in estimating the magnitude of the CHIKV outbreak in the Caribbean could be specificity and sensitivity of newly introduced diagnostics in centers not familiar with these procedures. In our small cohort, a large number of positive IgM IFA tests could not be confirmed in a secondary laboratory by gold standard serology testing. This illustrates the need for assay validation in epidemiological research to obtain solid and trustworthy data. Reports depending on only IgM assays in one single sample should be interpreted with caution. Phylogenetic analysis of the E1 protein gene was in line with other reports coming from the Caribbean, indicating that CHIKV circulating in Suriname is of Asian genotype, the same as the virus detected on St. Martin Island. The Asian genotype introduced in the Caribbean is closely related to strains recently isolated in China and the Philippines, suggesting that CHIKV strains circulating currently in the Western hemisphere originated from strains recently circulating between China, the Philippines, and Yap in Southeast Asia (Lanciotti and Valadere 2014). CHIKV disease is highly debilitating and can have severe economic consequences (Morrison 2014). Therefore, there is an urgent need for studies focusing on prevention, intervention (antiviral and vaccine developments), pathogenesis, and treatment of CHIKV infection.
Screening for hantavirus antibodies in undiagnosed patients in samples submitted to the BOG diagnostic laboratory indicated the possibility of human hantavirus infections in Suriname. On the basis of the results and case definition from the Dutch Hanta-Hunting study (Goeijenbier et al. 2014), confirmation of a routine serological test by FRNT is needed to define a “definite” hantavirus case. Because FRNT did not confirm the presence of (neutralizing) hantavirus antibodies in any of our samples, we cannot draw a firm conclusion about the presence and magnitude of hantavirus infections in Suriname. The lack of confirmation of the serological screening is the major limitation of our study, and for now we can only show an indication of hantavirus infection in Suriname. However, the high number of “probable” hantavirus cases as presented in Table 2 does stress the need for prospective studies addressing the presence and burden of hantavirus disease in Suriname.
For confirmation by neutralization tests. we relied on the hantavirus species for which we currently have virus stocks available. This meant that FRNT could be performed with one New World hantavirus, ANDV, and one Old-World hantavirus, SEOV, with a large global spread due to the global distribution of its reservoir, black and brown rats (Lin et al. 2012, Goeijenbier et al. 2013). New World ANDV is known to circulate in the southern parts of South America and with the long tailed pygmy rice rat (Oligoryzomys longicaudatus) as its reservoir (Bi et al. 2008, de Oliveira et al. 2014, Kruger et al. 2015). Currently, no data are available regarding the exact rodent species present in Suriname. Data from French Guiana, located on the eastern border of Suriname, showed the circulation and human cases of Maripa hantavirus infection, closely related to Rio Mamore hantavirus which circulates in Brazil (Montoya-Ruiz et al. 2014). Furthermore, a recent publication described the circulation of both Araraquara and Juquitiba virus in a region in Brazil closely to the southern border of Suriname (de Aurujo et al. 2015).
Because pathogenic hantaviruses are (almost) always associated with one specific rodent species, different or even undiscovered hantaviruses might circulate in Suriname. This could explain positive results in routine serology due to cross-reactivity with hantavirus species in the panel, but lack of FRNT confirmation. Another option can be that both ELISA and IFA test generated false-positive results. Potential limitation of routine diagnostic tests performed could have great implications for interpretation of epidemiological reports based only on ELISA and IFA results. Furthermore, the usability of these commercially available assays in areas where hantavirus epidemiology is not clearly studied could be debatable with the absence of FRNT confirmation. Especially the value of one positive result either in ELISA or IFA warrants further evaluation. Molecular detection of pathogenic hantaviruses either in rodents or symptomatic patients is warranted to confirm the presence and circulation of hantaviruses in Suriname.
Footnotes
Acknowledgments
The authors would like to thank Merril Wongsokarijo and Marina Sew-Atjon for their help during the collection of samples and data used in this study. We also thank Dr. James G. Fernandes (Groene Hart Hospital, Department of Urology) for his collaboration, personal effort, and advice.
Author Disclosure statement
No competing financial interests exist.