
Abstract
Between October 2012 and October 2013, unprecedented high numbers of Barmah Forest virus (BFV) disease cases were reported in the Northern Territory (NT). An investigation was launched by the NT Department of Health in cooperation with the Department of Primary Industry and Fisheries and the Department of Land Resource Management to investigate possible causes for this phenomenon. The investigation included virus isolations from mosquitoes collected in Darwin urban areas, BFV antibody testing in peri-urban small mammals and a human BFV disease case series investigation of recent cases. No BFV was isolated from the 4641 mosquitoes tested, none of the mammals tested positive for BFV antibodies, and the high BFV disease case numbers did not correlate with the relatively low mosquito vector numbers trapped in 2012–2013. It was estimated that up to 89% of the 79 human cases investigated did not have an acute arboviral illness and therefore had tested falsely positive. An Alere PanBio BFV immunoglobulin M enzyme-linked immunosorbent assay test kit is generally used to test for BFV, with the BFV disease case definition based on immunoglobulin M positives only. Other jurisdictions in Australia also reported high numbers of BFV disease cases, with the majority of the cases suspected to be false positives. Therefore, current testing methods need to be revised to reflect the true numbers of BFV disease cases occurring in Australia and to provide correct diagnoses for patients.
Introduction
B
BFV infection is a nationally notifiable disease with cases reported annually throughout Australia. Symptoms include joint pain, fever, malaise, and a rash, most commonly occurring on the limbs and trunk (Fraser 1986).
Although an outbreak of BFV infection of 16 confirmed cases occurred in Nhulunbuy in the NT in 1992 (Merianos et al. 1992), average reported case numbers in the NT per year are relatively low, with annual case numbers varying between 12 (1994–1995) and 122 (2008–2009) since recording began in 1991–1992 (Northern Territory Department of Health 2014).
However, in October 2012 BFV case notifications increased dramatically in the NT, with a total of 438 notifications between October 2012 and October 2013. The majority of the cases (341) were reported in the Darwin region, followed by 45 cases in the Alice Springs, 32 in the Katherine, and 19 in the East Arnhem regions. Only one case was reported from the Barkly region (Fig. 1).

Northern Territory administrative boundaries.
Cases are notified if they fulfil the national case definition as established by the Communicable Disease Network Australia. This definition includes laboratory criteria such as isolation of the virus and positive nucleic acid testing, but in practice almost all cases of BFV infection are notified by virtue of a positive immunoglobulin M (IgM) test. Cases are not routinely followed up and no clinical criteria are used in the definition. Testing for arbovirus in the NT at the time was carried out by several laboratories, all using the Alere PanBio BFV IgM enzyme-linked immunosorbent assay (ELISA) test (
An investigation into possible causes for the increase in BFV disease cases was launched by the NT DoH Centre for Disease Control in collaboration with the Department of Primary Industry and Fisheries (DPIF) and the Department of Land Resource Management (DLRM). The investigation included vector mosquito trapping and virus isolations, testing of small peri-urban mammals for BFV antibodies, and follow-up of a series of cases to ascertain the proportion of confirmed cases with a clinically consistent illness.
This paper outlines the BFV investigation carried out and reports on its findings.
Materials and Methods
Mosquito collection and processing
On May 13, 2013, four adult mosquito CO2-baited encephalitis vector surveillance traps were set in Darwin, adjacent to known Cx. annulirostris and Ae. vigilax breeding sites. Two traps were set on the edge of the Leanyer Swamp bordering the northern Darwin suburbs, with two other traps set adjacent to the Marrara freshwater swamp and in the Casuarina Coastal Reserve (Fig. 2). The traps were collected the following morning and transferred to the DoH Medical Entomology laboratory for processing.
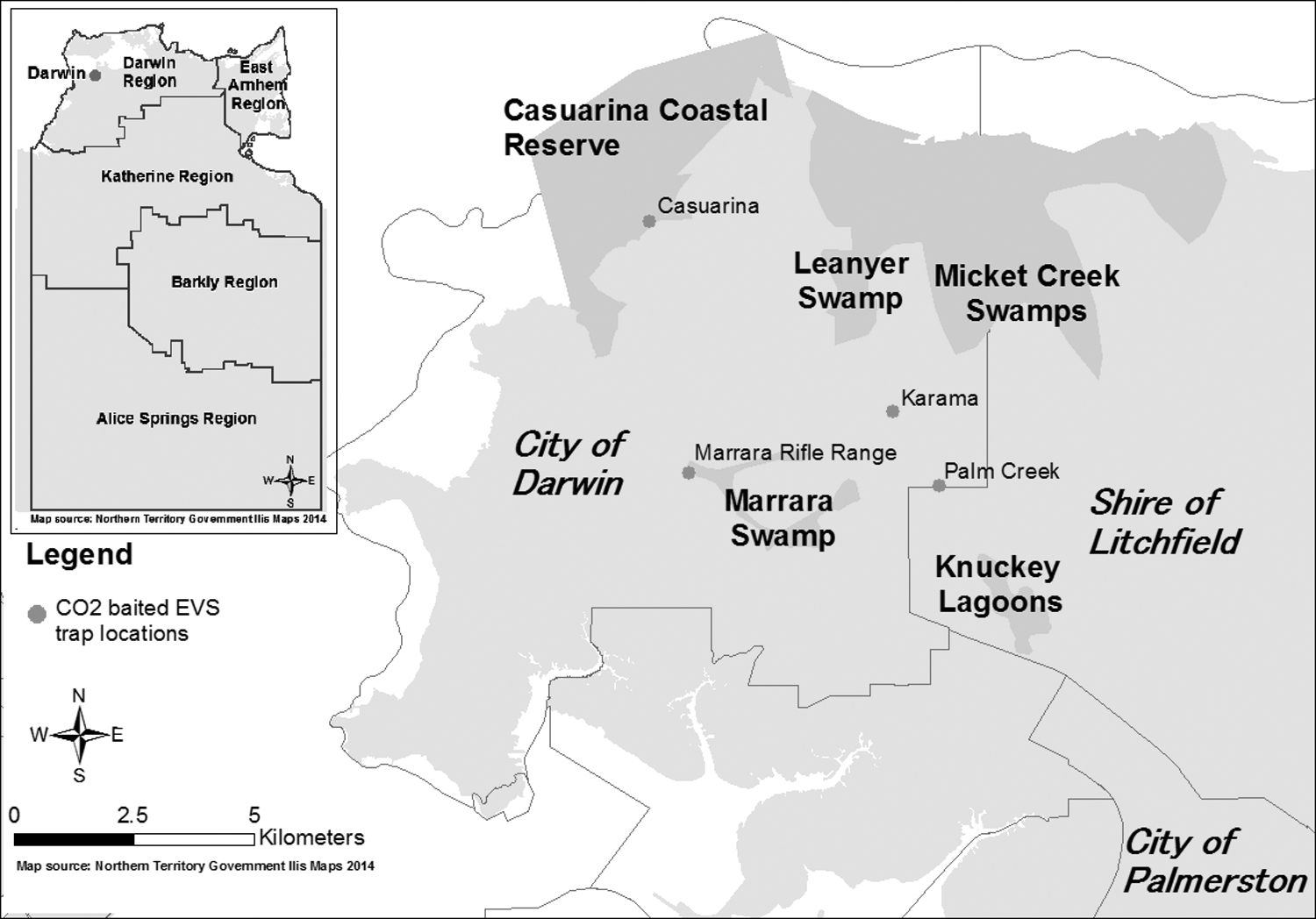
Location of CO2 baited encephalitis vector surveillance traps.
Adult mosquitoes were identified on a cold table to species level, with blood-fed mosquitoes removed to avoid sample contamination during virus testing. A maximum of 50 mosquitoes of the same species were pooled and stored in liquid nitrogen. The samples were transferred to DPIF for virus isolation.
Virus isolation and mammal BFV antibody testing
Methods used for mosquito virus isolation were as described by Weir (2002). In summary, up to 50 monospecific mosquitoes were added to tubes containing brain heart infusion broth, homogenized and clarified by centrifugation. Two confluent C6/36 cell culture tubes were each inoculated with 100 μL of mosquito homogenate and incubated. Each pair of C6/36 tubes was pooled together before passage to two baby hamster kidney (BHK)-21 and two hamster lung (HmLu)-1 cell culture tubes. At >passage two, day seven, cytopathic effect (CPE) negative cultures were pooled and inoculated to single BHK-21 and HmLu-1 cell culture tubes. Seed virus stocks were prepared from all CPE positive cultures by inoculation of BHK-21 or HmLu-1 or if both cell lines were CPE positive.
Inoculation of the third cell culture passage used the C6/36 second passage plates. The same method was employed as described in Weir 2002 for the inoculation of the second passage. The type and extent of CPE was recorded and at 80–100% CPE the supernatant was aseptically removed from the CPE positive wells and inoculated to BSR cells for the production of virus stocks. All homogenates from which virus was isolated were processed a second time to confirm the isolates and to rule out the possibility of cross contamination.
Concurrent with the investigation into the high BFV case numbers, DLRM in collaboration with the School of Veterinary and Life Sciences at Murdoch University, Perth, Western Australia, carried out research into the potential role of disease in the broad scale decline of native small mammal populations in the NT. This presented an opportunity to test small mammals from the Darwin area for BFV and Ross River virus (RRV) antibodies to assess BFV activity in the general area. Mammals were trapped in a 50 meter × 50 meter quadrat, using 20 Elliott and 4 small cage traps at 11 selected sites close to known Ae. vigilax and Cx. annulirostris breeding sites in the Darwin and Palmerston area, with traps open for four nights at each site during January and February 2014. Mammal trapping was approved by the Charles Darwin University Animal Ethics Committee (no. A11027). Blood samples from trapped mammals were tested for BFV and RRV antibodies. All animals were anaesthetized using isoflurane and were released at their point of capture after blood was taken, except for a feral cat and black rats that were euthanized.
The virus neutralization test was performed by a modified version of the method described by Weir (2003). The testing was carried out in 96-well plates using minimum essential medium (MEM; Sigma-Aldrich) supplemented with 10% fetal bovine serum. Briefly, 50 μL of serially diluted serum in quadruplicate wells was incubated with 50 μL of MEM containing 100 tissue culture infective doses of virus for 1 h at 37°C, then 100 μL of MEM containing 2 × 105 BSR cells (Sato et al. 1977) per mL was added and the plates were read for cytopathic effect after a 5-day incubation at 37°C. The serum neutralization antibody titers were calculated using the 50% end-point method first reported by Reed and Muench (1938).
Case follow-up
Follow up of a series of notified cases was undertaken to ascertain the proportion of cases having symptoms consistent with an acute arboviral infection of recent onset. Power calculations based on a standard error of 3% and a positive rate of 30% (based on a pilot of 25 cases) suggested that 121 cases were required for the series. A convenience sample of cases which fulfilled the national case definition for BFV infection was taken and included all cases notified after the commencement of the investigation and a smaller group of cases notified prior to the investigation, starting with those most recently notified. Only urban cases from Darwin, nearby Palmerston, and Alice Springs were included. Permission to contact each case and their contact details were sought from the relevant general practitioner. Three attempts were made to contact each case by phone. Cases were noted but excluded from further analysis if evidence was found that they were previously BFV IgG positive, or if subsequent testing had failed to show any BFV antibodies.
Clinical details were obtained by administering a questionnaire developed in-house and based on a clinical case definition for an acute arboviral infection. In the absence of a validated definition in the literature, the clinical case definition was established by reference to symptom profile reported in the literature, and discussion with clinical staff based on BFV infection being an acute illness characterized by fever and small joint arthralgia with or without arthritis (Hawkes et al. 1987, Merianos et al. 1992, Lindsay et al. 1995, NSW Government 1996, Flexman et al. 1998, Doggett et al. 1999, Passmore et al. 2002, Dore and Auld 2004, Cashman et al. 2008, Jacups et al. 2008, Public Health Laboratory Network 2013) (Table 1). It was not validated. Patients were questioned about symptoms, time to peak severity of illness, duration of symptoms, occupation, history, and laboratory results of prior infection with RRV or BFV and whether they could recall being bitten by mosquitoes in the 3 to 12 days preceding their illness. A differentiation was made between involvement of small joints and large joints due to the emphasis on small joint polyarthritis reported with BFV infection in the literature (Flexman et al. 1998). The data was analysed using Intercooled Stata® 11. The investigation was treated as a response to an outbreak and ethics approval was not sought.
Small joints include joints in hands, feet, wrists, or ankles.
Large joints include elbows, shoulders, knees, neck, hips, or back.
Results
Mosquito processing and virus isolation
A total of 4641 mosquitoes, including 3671 Cx. annulirostris and 862 Ae. vigilax were processed for virus isolations between May 14 and 17, 2013 (Table 2).
No BFV was isolated from the mosquitoes tested. Two unidentified viruses (V8952 and V8953) were isolated from two pools of Cx. annulirostris, with identification of the viruses pending.
BFV mammal antibody testing
During January and February 2014, a total of 19 mammals were trapped and tested for BFV and RRV antibodies, including 2 brushtail possums (Trichosurus vulpecula), 5 black-footed tree-rats (Mesembriomys gouldii), and 12 northern brown bandicoots (Isoodon macrourus). Two opportunistically sampled black rats (Rattus rattus) and a feral cat (Felis catus) were also tested. None of the animals tested positive for BFV antibodies. However, both brushtail possums, four black-footed tree-rats, three northern brown bandicoots, and the feral cat tested positive for RRV antibodies.
Case follow-up
All cases were notified by virtue of a positive IgM. Due to resource and time constraints, the follow up was stopped after collecting data on 80 cases. This represented 75% of the 107 cases contacted and 33% of the 241 cases notified between February 13 and June 11, 2013. One person was later excluded from the case series based on a previous positive result for BFV IgG antibodies in 2009. Symptoms reported from the 79 cases included in the series are shown in Table 3.
BFV, Barmah Forest virus.
Of the 79 cases, 9 (11.4%) fulfilled the clinical case definition for a confirmed acute arboviral infection and a further 12 (15.2%) for a probable infection (Table 4). Of the 58 cases that did not meet the clinical case definition, 34 (59%) failed to fulfil the clinical criteria by virtue of a delay of greater than 4 weeks between symptom onset and being tested, suggesting a subacute or chronic course rather than one of acute onset. Of these 34 cases, 28 (82%) tested negative for BFV IgG antibodies, whereas at this stage of their illness they would be expected to be positive.
Evidence from this case series suggested that between 11% and 27% of BFV notifications had a clinical illness compatible with an acute arboviral infection (Table 4), that is the positive predictive value of the test is at most 27%. Results for RRV infection were available for 76/79 (96%) of the people contacted, with 3 people testing positive for RRV IgM antibodies.
Discussion
In 2012–2013, unusual high numbers of BFV disease cases were reported throughout Australia. In response to the high number of cases in the NT reported between October 2012 and October 2013, mosquito virus isolations, limited small mammal BFV antibody testing and human case investigations, were carried out. No BFV was detected in the known vector mosquitoes tested. In addition, mosquito vector numbers were relatively low in the Darwin area in 2012–2013 and did not correlate with the increase in reported BFV disease cases. These findings agreed with results from Western Australia, where high numbers of BFV disease cases were also notified in 2012–2013, while environmental conditions were not favourable for a BFV disease outbreak, and the level of BFV isolated from mosquitoes was similar compared with previous years (Western Australia Department of Health 2013). In South Australia, increases in BFV notifications were also not noticeably associated with elevated levels of mosquitoes (C. Williams, personal communication, October 31, 2014), and in the past, unusual high numbers of BFV cases were notified in New South Wales during relatively dry periods when mosquito vector numbers were low and minimal arbovirus activity was recorded (Doggett et al. 2004).
Although Whelan and Weir (1993) suggested a BFV detection rate of 1/38,089 for Cx. annulirostris and 1/6493 for Ae. vigilax, derived from virus isolation work carried out in the NT between 1982 and 1992. A much higher detection rate of 1/910 for Ae. vigilax was reported during the BFV outbreak in Nhulunbuy in 1992 (Merianos et al. 1992). In addition, the University of Western Australia Arbovirus Surveillance and Research Laboratory reported detection rates of 0.8/1000, 1.9/1000, and 2.7/1000 for Ae. vigilax and 2.3/1000 for Cx. annulirostris in the north of Western Australia in 2013–2014 (University of Western Australia 2014). The Western Australian and Nhulunbuy BFV outbreak detection rates suggest that the relatively small number of vector mosquitoes tested during this investigation might have been sufficient to detect virus during a BFV disease outbreak. Although it is acknowledged that the absence of BFV in the mosquitoes tested is no proof of low BFV activity, the fact that all mosquitoes tested negative for the virus during the suggested 2012/13 outbreak supports the suggestion that BFV activity was low during the time when high numbers of human BFV disease cases were reported.
In addition, although the principal mammalian hosts for BFV are still unknown, brushtail possums and cats have previously been found to be infected with BFV (Boyd et al. 2001, Kay et al. 2007). Thus, during periods of high BFV activity, it should be expected that some brushtail possums and cats show antibodies to BFV. However, despite the relatively small sample during this investigation, the fact that all mammals tested negative to BFV antibodies, while some tested positive to RRV antibodies, with both the principal vectors Cx. annulirostris and Ae. vigilax known to feed on brushtail possums and cats (Key et al. 2007), further supports the suggestion that BFV activity might have been low in the NT during the time of high human BFV case notifications.
Our case series results indicated a low positive predictive value (PPV) in this population, suggesting a possible recent decrease in the specificity of the Alere PanBio BFV IgM ELISA and concomitant rise in false positive results. Our findings are supported by the fact that the BFV test kits (lot numbers 12354, 13051, and 13140) were recalled by Alere on September 13, 2013, due to suspected increases in false positive results (Department of Health Therapeutic Goods Administration [TGA] 2013). However, we were unable to interview those cases prior to the October 2012 increase and thus could not be certain that the fall in the PPV was recent.
It is also possible that a contributory factor to the loss of the PPV was a change in testing behavior by clinicians, such that the test was being used in a population with a lower pre-test probability. While it is unlikely that this change occurred over the few months in which case numbers increased, it is noteworthy that a large proportion (63%) of cases had a history of joint pain for greater than 2 months, suggesting a chronic or subacute course.
Moreover, arboviruses are increasingly being listed as causes of chronic arthralgia and chronic fatigue syndrome in the lay media (Griffen 2005), and this may be stimulating demand from patients to be tested for arbovirus disease. Our estimate of the PPV of 27% is compatible with the specificity and sensitivity of the ELISA test as stated in the product specifications (94% and 97% respectively) (Alere Panbio Barmah Forest Virus IgM ELISA) if the true prevalence of BFV infection in the population tested was 2%. Interestingly the recall statement from the Department of Health TGA mentioned a “shift in the sero-epidemiology of the patient population currently being tested” as a reason for the recall (Department of Health TGA 2013).
A limitation of our case series was the use of an unvalidated clinical case definition to identify true cases of BFV infections. Even though the definition was developed from the disease spectrum reported in the literature, the sensitivity and specificity of the definitions are uncertain. We are confident that RRV infection was not the cause of illness, as most people in the case series were tested for RRV and showed no evidence of recent infection. Therefore, it is unlikely that the BFV IgM results are a product of cross reactivity with RRV infection.
In the case series, 82% of IgM positive cases who had symptoms for greater than 4 weeks had a negative BFV IgG result. Even though no follow-up testing results were available, a rise in IgG titer would be expected 2 to 4 weeks following onset of symptoms, so failure to show presence of IgG antibodies after this period suggests a falsely positive IgM result. Therefore, results based on a single positive IgM for BFV should be interpreted with caution (Cashman et al. 2008). Collection of a convalescent sample, which shows conversion of IgG from negative to positive provides stronger evidence and confirmation of recent infection (Public Health Laboratory Network 2013). To aid diagnosis, physicians should be encouraged to collect a second blood sample 4 weeks following onset of symptoms.
Conclusions
Findings from our environmental investigations together with evidencefrom the case series and the recall of the Alere PanBio BFV IgM ELISA test kit supports the conclusion that a decrease in BFV IgM test specificity was the most likely cause of the surge in BFV notifications. A collection of a convalescent sample, which shows conversion of IgG from negative to positive provides stronger evidence and confirmation of recent infection, with a four-fold increase in titer providing conclusive evidence of a recent infection. Clinicians may need to consider alternative diagnoses while awaiting convalescent sample results in patients.
Footnotes
Acknowledgments
We thank all medical entomology staff who were involved in the mosquito trapping and processing, DPIF staff involved in the virus testing, DLRM staff involved with the mammal trapping program, and all participants in the BFV case series. Work undertaken by Danielle Stokeld was in part funded by the Australian Government's National Environmental Research Program.
Author Disclosure Statement
No competing financial interests exist.