
Abstract
Anthrax is a zoonotic infectious disease caused by Bacillus anthracis. While anthrax is rare in developed countries, it is endemic in Turkey. The names of the different forms of the disease refer to the manner of entry of the spores into the body—cutaneous, gastrointestinal, inhalation, and injection. The purpose of this study was to evaluate the clinical characteristics, epidemiological history, treatment, and outcomes of patients with anthrax. Eighty-two cases of anthrax hospitalized at Atatürk University Faculty of Medicine Department of Infectious Diseases and Clinical Microbiology in 2008–2014 were examined retrospectively. Gender, age, occupation, year, history, clinical characteristics, character of lesions, length of hospitalization, and outcomes were recorded. Thirty (36.6%) patients were female and 52 (63.4%) patients were male; ages were 18–69 and mean age was 43.77 ± 13.05. The mean incubation period was 4.79 ± 3.76 days. Cases were largely identified in August (41.5%) and September (25.6%). Sixty-nine (84.1%) of the 82 patients had been given antibiotics before presentation. Lesions were most common on the fingers and arms. The most common occupational groups were housewives (36.6%) and people working in animal husbandry (31.7%). All patients had histories of contact with diseased animals and animal products. Penicillin-group antibiotics (78%) were most commonly used in treatment. One patient (1.2%) died from anthrax meningitis. The mean length of hospitalization was 8.30 ± 5.36 days. Anthrax is an endemic disease of economic and social significance for the region. Effective public health control measures, risk group education, vaccination of animals, and decontamination procedures will reduce the number of cases.
Introduction
A
In Turkey, anthrax is endemic in the eastern, southeastern, and central Anatolian regions (Akbayram et al. 2010, Doganay et al. 2010, Engin et al. 2010). It causes economic burdens due to health problems and animal deaths (Özkurt et al. 2005, Doganay et al. 2010). Transmission of anthrax may be laboratory, industrial, or agricultural in origin (Doganay et al. 2010, Engin et al. 2010), but no industrial cases have been reported from Turkey (Kaya et al. 2002). Instead, agricultural anthrax predominates (Kracalik et al. 2014); it is seen in all seasons, but most commonly in summer and fall (Karahocagil et al. 2008. Özcan et al. 2008).
Anthrax may be cutaneous, pulmonary, gastrointestinal, or injectional (Sweeney et al. 2011, Kajfasz et al. 2014). The cutaneous form constitutes 95% of human cases (Doganay et al. 2010). Its course is benign, with an untreated mortality rate of 0–20% (Kaya et al. 2002). Cutaneous anthrax derives from the slaughter, skinning, and preparation of meat from diseased animals (Kamal et al. 2011, Kayabas et al. 2012). Cutaneous anthrax is the most benign form and rarely causes sepsis or meningitis (Parlak et al. 2015). Gastrointestinal anthrax results from the consumption of infected meat, with mortality reported at 50% (Kaya et al. 2002, Lucey 2005). The most lethal form is pulmonary anthrax (Kamal et al. 2011, Sweeney et al. 2011). Laboratory transmission is rare. The most memorable case of laboratory transmission was an accident in the Soviet city of Sverdlovsk (now Yekaterinburg, Russia) in 1979 that affected 96 people and caused the deaths of 64 (Meselson et al. 1994, Bravata et al. 2007).
The incubation period for anthrax is 1–9 days (Kaya et al. 2002). The disease begins with itching and burning in the skin at the site of spore entry. A small red macule forms, which turns into a papule and grows into a vesicle. The center of the vesicle is depressed and filled with fluid and is surrounded by an erythematous, edematous area. Within a few days, the fluid inside the vesicle turns unclear and dark in color and then turns black and necrotic. The lymph nodes become swollen and painful (Irmak et al. 2003, Karahocagil et al. 2008). It may take 2–3 weeks for the eschar to cast off (Özcan et al. 2008).
Definitive diagnosis of anthrax is based on observation of the bacillus at Gram staining and growth in culture. Diagnosis is made following growth of the agent in culture and presence of the agent at PCR. The enzyme-linked immunosorbent assay (ELISA) shows an increase in anti-protective antigen (PA) and anti-lethal factor (LF) titers (Oncül et al. 2002, Baykam et al. 2009, Sweeney et al. 2011).
In this study, we evaluated clinical and laboratory data of anthrax cases and examined these cases in terms of epidemiological characteristics, clinical findings, treatment, and prognosis.
Materials and Methods
Cases of cutaneous anthrax monitored at the Atatürk University Faculty of Medicine Department of Infectious Diseases and Clinical Microbiology were included. The records of cases hospitalized between April, 2008, and December, 2014, were scanned retrospectively. Sex, age, occupation, exposure, nature of lesion, place, year, month and town of presentation, previous antibiotic use, treatment, and outcomes were recorded. Full blood count, short biochemical analyses, and C-reactive protein (CRP) were investigated. Specimens were taken from lesions for Gram staining and culture, and blood cultures were taken from patients with fever. Diagnosis of cutaneous anthrax was based on medical history, nature of lesion, clinical findings, and/or microbiological investigations. Medical history inquired into contact with diseased animals or animal products, time of appearance of lesions, and previous antibiotic use. Specimens were taken from lesions for Gram staining and culture using a conventional method with a needle, lifting the lesion edge with a swab. The specimen was placed in sheep's blood broth and kept in a stove at 37°C for 1 day. Observation of Gram-positive bacilli at Gram staining and the growth of Gram-positive, flat, adherent, penicillin-sensitive bacilli with no hemolysis and an undulating hair structure were evaluated as positive.
Statistical analyses were performed using SPSS software version 20 (IBM, Chicago, IL). Laboratory and epidemiological data were entered. The chi-squared test, Student t-test, and the Kruskal–Wallis test were used. A p value of <0.05 was considered statistically significant.
Results
Eighty-two cases of anthrax from our department were evaluated in terms of clinical characteristics, occupation, months of presentation, treatment, and prognosis. The cases consisted of 30 (36.6%) women and 52 (63.4%) men. The mean age of patients was 43.77 ± 13.05 years. Thirty (36.6%) patients were aged 26–40, 22 (26.8%) were aged 41–50, 24 (29.3%) were aged over 51, and 6 (7.3%) were under 25. All patients had cutaneous anthrax, with 29 (35.4%) cases being the mild cutaneous form. The mean incubation period was 4.79 ± 3.76 days. A history of animal slaughter was present in 46 (56.1%) patients, contact with animal meat in 29 (35.4%), administering drugs to animals or injury with a needle used on animals in four (4.9%), wool shearing in two (2.4%), and of being bitten during feeding in one (1.2%). Thirty (36.6%) patients were housewives, 26 (31.7%) worked in animal husbandry, and 16 (19.5%) were farmers (Fig. 1).
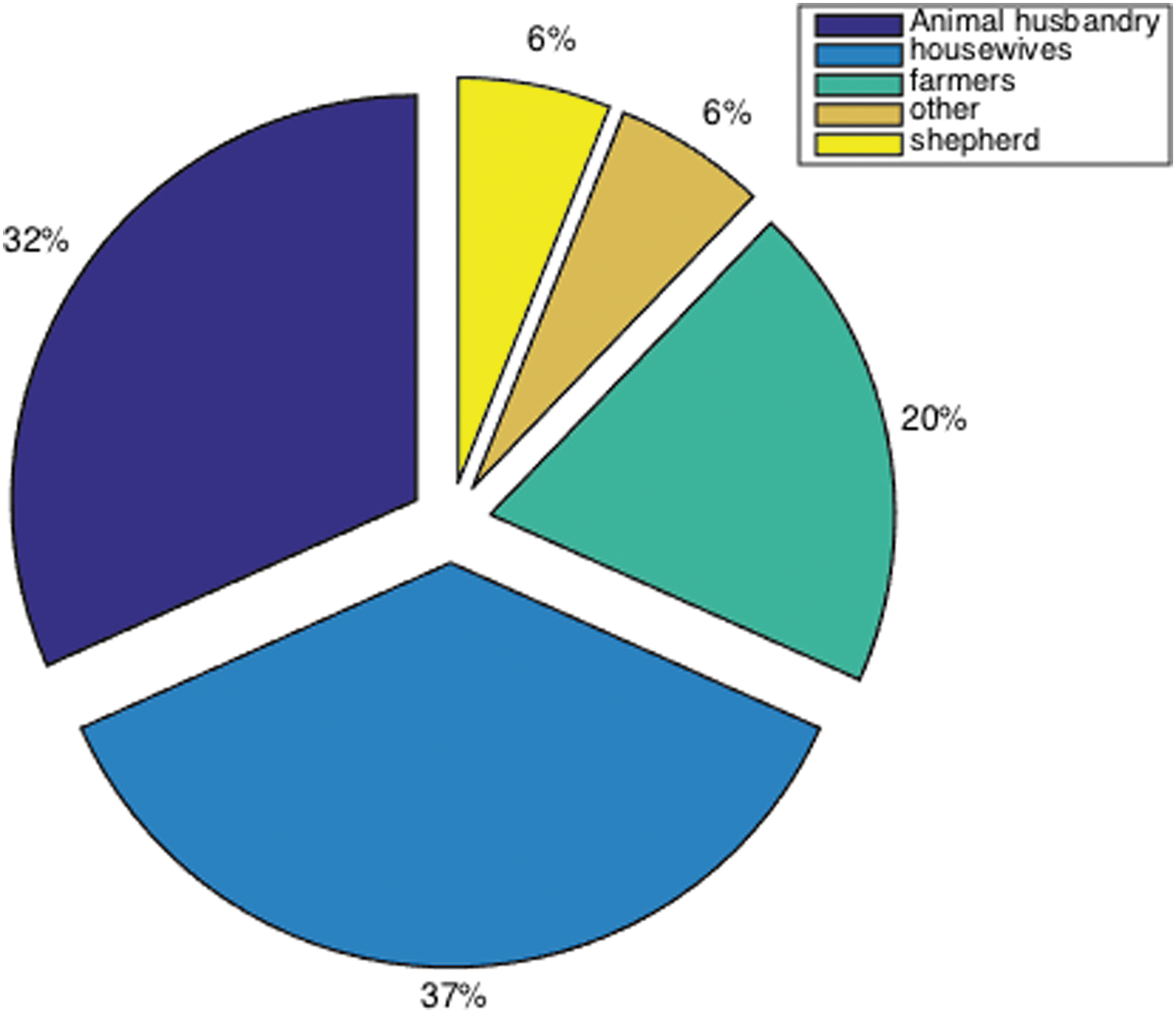
Distribution of cases by occupation. Color images available online at
Cases were mostly clustered in August and September; 34 (41.5%) were determined in August and 21 (25.6%) in September (Fig. 2). No cases were detected in January or March. In terms of distribution by year, 27 (32.9%) cases were determined in 2008, nine in 2009, 11 (13.4% (in 2010 and 2012, 10 (12.2%) in 2011 and 2013, and four in (4.9%) in 2014 (Fig. 3). Lesions were seen on the fingers in 31 patients (37.8%), the arms in 19 (23.2%), the hands in 17 (20.7%), the face and neck in nine (11%), and the eyes in six (7.3%). There was no lower extremity involvement in any case. Upper extremity involvement was present in 67 (81.7%) patients (Figs. 4 and 5) and face and neck involvement in 15 (18.3%) (Figs. 6 and 7). The most common findings were erythema in 74 (90.2%) cases, swelling in 72 (87.8%), eschar in 63 (76.8%), pain in 35 (42.7%), fever in 21 (25.6%), and itching in 11 (13.4%). Presentations to our hospital were most common from the provinces of Erzurum in 44 (53.7%), Kars in 15 (18.3%), and Agrı in eight (9.8%). The mean length of hospitalization was 8.30 ± 5.36 days. Two patients were pregnant and gave birth in a healthy condition. Compartment syndrome developed in three patients, and two of them underwent surgery. One was a case of eyelid anthrax resulting in blindness. There was one case of anthrax meningitis, and this patient died on the 5th day of hospitalization, despite treatment.
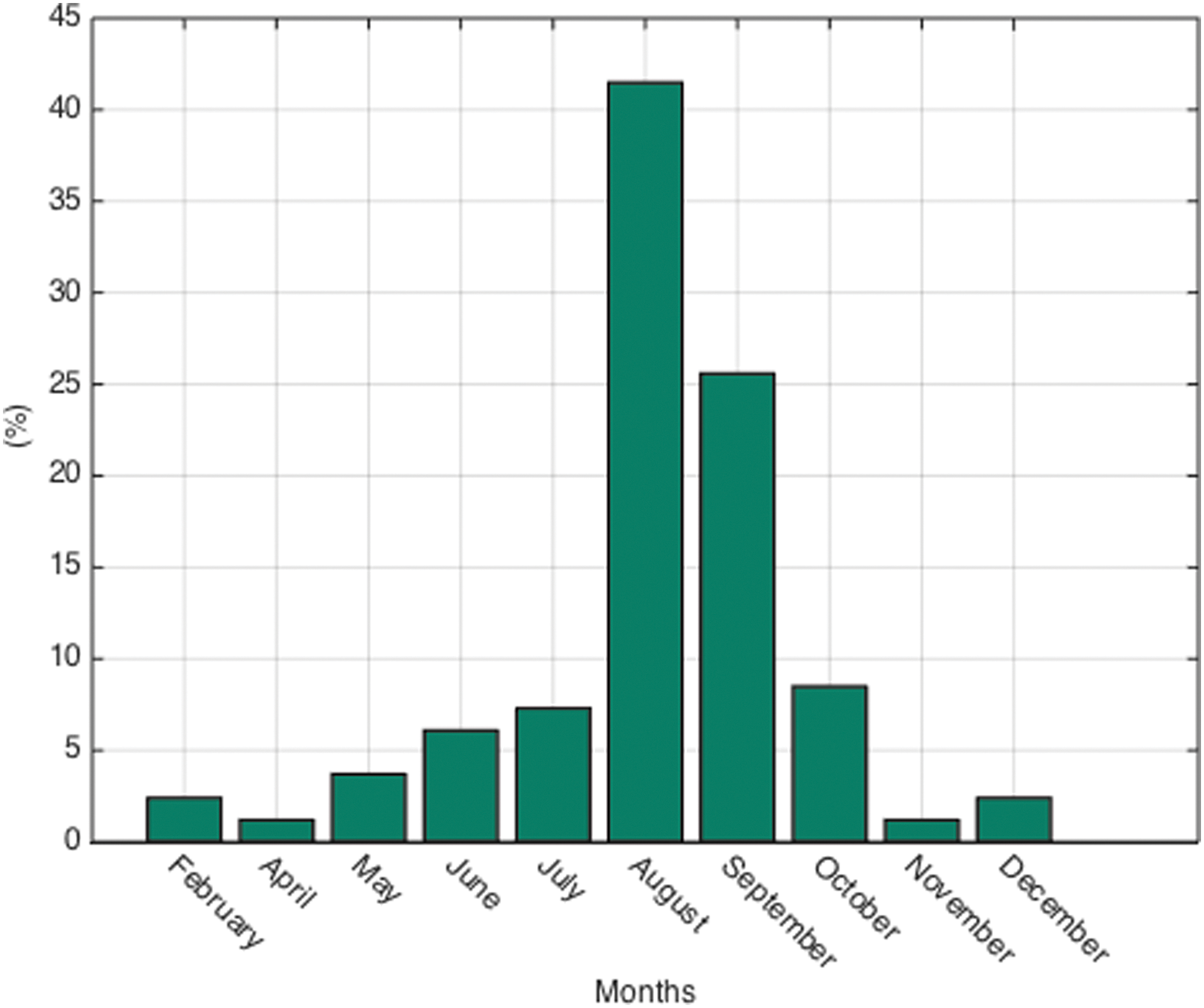
Distribution of cases by month. Color images available online at
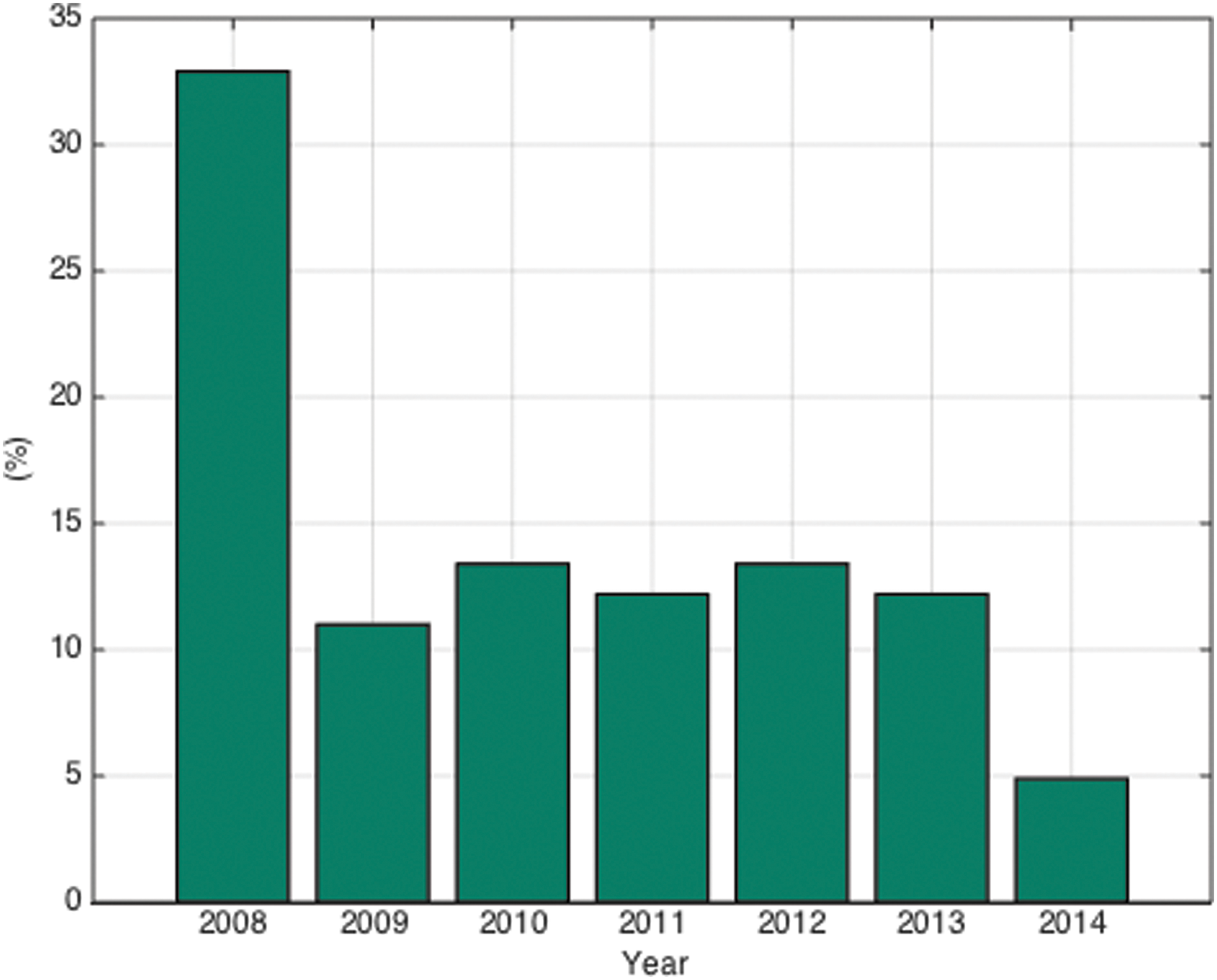
Distribution of cases by year. Color images available online at

Edematous lesion around on the left hand. Color images available online at

Cutaneous lesion on the right hand. Color images available online at

Extensive edema surrounding the right eye. (Patient permission received) Color images available online at

Cutaneous anthrax lesion on the lips. Color images available online at
Bacteria were observed at Gram staining in 15 (18.3%) patients, and growth in culture in 11 (13.4%). Patients' clinical and laboratory findings are summarized in Table 1. Because the number of patients previously using antibiotics was very high, 69 (84.1%), the level of growth in culture in this group was significantly lower compared to those not using antibiotics (p = 0.001). Cases of findings in the form of mild pustules and those with severe cutaneous anthrax differed significantly in terms of alanine aminotransferase (ALT), aspartate aminotransferase (AST), CRP, and platelet and white blood cell values (Table 2). Penicillin group drugs were the most commonly used antibiotics at 78%. Crystallized penicillin was used in 50% of patients. Procaine penicillin, ampicillin, or ciprofloxacin were used in mild cutaneous anthrax. Treatment started with crystallized penicillin in patients with severe cutaneous anthrax and was altered to procaine penicillin with decreased fever. Prednisolone was added to treatment in this clinical form. Penicillin and ciprofloxacin were used in the case of the one patient (1.2%) that had anthrax meningitis and died; B. anthracis grew in blood and cerebrospinal fluid culture in that case. The erythrocyte sedimentation rate was higher than normal (20 mm/h) in 40 (48.7%) patients, and white blood cell count was higher than normal (3000–10,000) in 41 (50%). CRP was higher than normal in 47 (57.3%) patients.
The p value in the comparison of cases of severe and mild cutaneous anthrax.
SD, standard deviation; CRP C-reactive protein; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
Discussion
Industrial anthrax may be transmitted from materials worked in factories, such as skin, hair, wool, and bone, and represents the majority of cases in developed cases. Agricultural anthrax is associated with animal husbandry and occurs after direct animal contact. All cases in Turkey are agricultural anthrax (Demirdağ et al. 2003). A history of animal slaughter (56%) and/or contact with animal flesh (35.4%) was present in most of our cases. Direct contact with animals was present in almost all cases.
Control of the anthrax in humans depends on controlling the disease in animals (Kracalik et al 2014). Anthrax in Turkey has been seen for many years due to traditional agricultural practices. As a precaution, animal carcasses should be buried at a depth of 2 meters, and necropsy must not be performed (Kajfasz et al. 2014).
The various forms of anthrax—cutaneous, gastrointestinal, inhalation, and injection—depend on the site of entry of spores into the body. The most widespread and mildest type is the cutaneous form, representing 95% of all cases. Other forms are very rare (Kajfasz et al. 2014). The injection form has been reported in heroin users from European countries during the last 5 years (Booth et al. 2010, Holzmann et al. 2012). Cutaneous anthrax represents the majority of cases reported from Turkey (Karahocagil et al. 2008, Özcan et al. 2008, Doğanay et al. 2010); however, no transmission between patients has been reported and other forms of anthrax are not observed in health personnel through contact with a cutaneous anthrax patient.
The B. anthracis micro-organism enters the body through injured skin. A primary lesion surrounded by red edema forms with the release of toxins (Karahocagil et al. 2008). Lesions are frequently located on exposed parts of the body and most commonly on the hands, fingers, and arms due to contact with animals and animal products (Kaya et al. 2002, Irmak et al. 2003) and are reported as the most commonly affected areas (Kaya et al. 2002, Karahocagil et al. 2008). In a study involving children, Akbayram et al. (2010) reported predominantly facial involvement, with eyelid involvement at a level of 32.3% and involvement of the area around the mouth at a level of 24.6%. Baykam et al. (2009) reported hand and finger involvement at levels of 39% and 29%, respectively. Özden et al. (2012) reported hand involvement at a level of 54.5% and Engin et al. (2010) at 48.7%. Demirdağ et al. (2003), Karahocagil et al. (2008), and Irmak et al. (2003) reported hand and finger involvement at 48%, 43%, and 38.5%, respectively. Similarly, in our study, the most common involvements were in the fingers (37.8%), arms (23.2%), and hands (20.7%). Eyelid involvement was present in six (7.3%) patients. Toxemia-related blindness developed in one of these patients.
Some studies report no variation in terms of gender (Kaya et al. 2002, Öncül et al. 2002, Karahocagil et al. 2008, ). We attributed this to men and women working together in the animal husbandry and agriculture sectors. Demirdağ et al. (2003) reported that males constituted 60% of cases, whereas Doğanay et al. (2010) determined a level of 68%. Irmak et al. (2003), however, reported that women represented 65.4% of cases. Akbayram et al. (2010) reported greater numbers of males (56.9%) in a series of pediatric patients. A publication from Georgia reported that 84% of patients were male and that male gender increased the risk 4.95-fold (Kracalik et al. 2014). Women work alongside men in animal husbandry in some regions. Gender variation is associated with working with animals and with sociocultural practices. We attributed the majority of our patients being men to animal husbandry, which is a primarily male activity in our region.
Agricultural anthrax is primarily seen in individuals occupied in animal husbandry and farming. Engin et al. (2010), Özden et al. (2012), Kaya et al. (2002), and Karahocagil et al. (2008) reported that farmers represented 59%, 48%, 44.8%, and 23.5% of cases, respectively. Kracalık et al. (2014) reported a 68% level of working in animal husbandry or as a butcher, whereas Irmak et al. (2003) reported a 35.9% level of working in animal husbandry. Levels of working as housewives were reported at 43% by Özden et al. (2012), 41.2% by Karahocagil et al. (2008), and 32.5% by Kaya et al. (2002). In terms of our own cases, 36.6% were housewives, 31.7% worked in animal husbandry, and 19.5% were farmers. All of those describing themselves as housewives worked either in animal husbandry or farming. Our results were comparable with those in the literature.
Because cutaneous anthrax is primarily agricultural in origin, contact with animals predominates. A level of contact with diseased animals and products exceeds 90% in the majority of studies (Demirdağ et al. 2003, Karahocagil et al. 2008, Engin et al. 2010). The level of contact with animals and products in our study was almost 100%. The greatest exposure has been reported during animal slaughter, skinning, and meat preparation (Kaya et al. 2002, Irmak et al. 2003, Baykam et al. 2009, Engin et al. 2010). Similarly, in our study, the most common mode of transmission was animal slaughter or assisting with slaughter in 46 (56.1%) patients, followed by contact with meat in 29 (35.4%). The most significant history of contact was animal slaughter or assisting with slaughter.
Some studies have reported that cases are most commonly seen in August (Demirdağ et al 2003, Karahocagil et al. 2008, Engin et al. 2010). In our study, no cases were determined in January or March, and 41.5% of cases were seen in August and 25.6% in September. These levels are compatible with the published literature. Studies have reported a significant relation between seasonal variation and incidence of cases. Contact with animals increases in spring and summer. Spores may be more active in the environment in association with dry conditions.
Penicillin and ciprofloxacin are the recommended agents for first-line treatment. Tetracycline, macrolide, aminoglycoside, chloramphenicol, and first-generation cephalosporins can also be used as alternative treatments (Bravata et al. 2007, Doğanay et al. 2009, Sweeney et al. 2011, Kajfasz et al. 2014, Goel 2015). Penicillin therapy is effective and is the preferred treatment of cases of agricultural anthrax (Demirdağ et al. 2003, Irmak et al. 2003, Karahocagil et al. 2008). Penicillin therapy was administered to 78% of our patients, and a response was achieved quickly, a result compatible with the literature. No resistant cases were determined in culture-positive cases. Öncül et al. (2002) identified penicillin sensitivity in all 14 strains and Bakıcı et al. (2002) in all 28 strains. Ortatatlı et al. (2012) assessed the results of sensitivity tests in 55 strains of B. anthracis. Resistance to erythromycin was determined in one strain, resistance to gentamicin in two, and resistance to both penicillin and doxycycline in one. Strains used in bioterror attacks are capable of producing inducible cephalosporinase and penicillinase. For cases of inhalation anthrax, the Centers for Disease Control and Prevention (CDC) recommends ciprofloxacin and doxycycline for 60 days as the first choice of treatment. Shorter treatment has been found to be effective in cases of cutaneous anthrax if no complications develop (Baykam et al. 2009, Kayabaş et al. 2012). Treatment was administered for 5–15 days in our cases.
In cases of excessive edema, the addition of prednisolone has been reported to produce a more rapid decrease in edema (Irmak et al. 2003, Karahocagil et al. 2008, Engin et al. 2010). We added 1 mg/kg per day prednisolone in cases with excessive edema and this proved beneficial. Surgical incision is definitely not advised in cutaneous anthrax. Local antibiotics have no effect in treatment. Dressing with local rivanol and covering with gauze bandages is sufficient.
High levels of culture positivity, at 53.6% and 43.6%, have been reported by Akbayram et al. (2010) and Engin et al. (2010), respectively. Özden et al. (2012), Baykam et al. (2009), Karahocagil et al. (2008), and Kaya et al. (2002) reported culture positivity levels of 11.4%, 12.1%, 12.9%, and 16.7%, respectively. There may be no growth in cultures taken 24–48 h after antibiotic use (Demirdağ et al. 2003, Akbayram et al. 2010). Culture positivity in our study was 13.4%, with previous antibiotic use of 84.1%. Growth was significantly low in patients with previous use of antibiotics (Doğanay et al. 2010). Growth levels do not exceed 60–65% (Karahocagil et al. 2008, Baykam et al. 2009, Goel 2015). Öncül et al. (2002) reported a low level of culture positivity of 3.1%. We attributed our low growth rate to patients taking antibiotics before arrival. Patients started on antibiotics either spontaneously or before prescription by physicians due to severity of anthrax. Our university hospital accepts patients from seven surrounding provinces. Baykam et al. (2009), however, reported that prior antibiotic use had no effect on culture and Gram staining.
Culture is the gold standard in microbiological identification. In addition to Gram staining used to assist diagnosis in anthrax, modern diagnostic techniques such as ELISA and PCR are also employed (Lucey 2005, Sweeney et al. 2011, Goel 2015). Lethal factors and protective antigens were investigated in one case of eyelid anthrax. It was not possible to use ELISA and PCR in other cases. There are no specific laboratory findings in patients. Studies in the literature have reported elevated CRP, sedimentation, and leukocyte values (Demirdağ et al. 2003, Karahocagil et al. 2008, Özcan et al. 2008). In our study, 40 patients had a sedimentation rate above 20 mm/h, 47 had CRP values above 5 mg/liter, and 41 had leukocyte values greater than 10,000. Further studies investigating the relation between high values and toxin levels are now needed.
Twenty-seven patients were seen in 2008, nine in 2009, 11 in 2010, 10 in 2011, 11 in 2012, 10 in 2013, and four in 2014. A decrease on an annual basis was observed due to increased animal monitoring, higher rates of vaccination, and improved public education and veterinary services. The most important agent in the decrease is thought to be the reduction in animal anthrax cases (Özkurt et al. 2005, Doğanay et al. 2009, Kracalik et al. 2014).
Lesion type and appearance and patient history are very typical. An experienced individual can immediately establish diagnosis. Immediate commencement of antibiotics can prevent development of systemic disease (Irmak et al. 2003). It does not alter eschar form, lesion appearance, or healing. Tularemia, zoster, erysipelas, actinomyces, staphylococci infections, cowpox virus, and orf lesions must be considered at differential diagnosis (Irmak et al. 2003, Kajfasz et al. 2014).
In conclusion, anthrax is still endemic in Turkey. Early diagnosis and appropriate treatment and procedures when required are life saving. Physicians working in these regions must consider anthrax when they see typical lesions or if contact with diseased animals or animal products is present at anamnesis. Vaccination of animals, education, and prevention of slaughter of diseased animals are essential if the numbers of cases are to be reduced.
Footnotes
Author Disclosure Statement
No competing financial interests exist.