
Abstract
Borrelia species fall into two groups, the Borrelia burgdorferi sensu lato (Bbsl) complex, the cause of Lyme borreliosis (also known as Lyme disease), and the relapsing fever group. Both groups exhibit inter- and intraspecies diversity and thus have variations in both clinical presentation and diagnostic approaches. A further layer of complexity is derived from the fact that ticks may carry multiple infectious agents and are able to transmit them to the host during blood feeding, with potential overlapping clinical manifestations. Besides this, pathogens like Borrelia have developed strategies to evade the host immune system, which allows them to persist within the host, including humans. Diagnostics can be applied at different times during the clinical course and utilize sample types, each with their own advantages and limitations. These differing methods should always be considered in conjunction with potential exposure and compatible clinical features. Throughout this review, we aim to explore different approaches providing the reader with an overview of methods appropriate for various situations. This review will cover human pathogenic members of Bbsl and relapsing fever borreliae, including newly recognized Borrelia miyamotoi spirochetes.
Introductory Remarks
B
Appropriateness of different diagnostics vary with both time, clinical course and causative species, each additionally having strengths and limitations. These differing methods should always be considered in conjunction with potential exposure and compatible clinical features. Throughout this review, we aim to explore different approaches providing the reader with an overview of methods appropriate for various situations. This review will cover human pathogenic members of Bbsl and relapsing fever borreliae, including newly recognized Borrelia miyamotoi spirochetes.
Detection of Borrelia in the Arthropod Vector
Various methods can be applied to detect the presence of Borrelia in vectors. Widely used approaches that demonstrate significant sensitivity, specificity and reliability include the following: multiple formats of PCRs, mostly nested PCR that target different genomic loci, selection of which depends on the sample origin (template); reverse-line blotting, based on hybridization of amplified selected Borrelia genes with spirochete-specific probes; and multilocus sequences analysis and multilocus sequence typing, based on the sequence analysis of amplified fragments of spirochete genome or microscopy with stained spirochetes in tick midgut or salivary glands (Aguero-Rosenfeld et al. 2005, Margos et al. 2011). The most recently applied techniques include next-generation sequencing (NGS) and proteomic approaches.
Cultivation of Borrelia in commercial Barbour-Stoenner-Kelly (BSK) or home-made modified Kelly- Pettenkoffer (MKP) media, which for a long time is considered to be a gold standard in LB diagnostics, is still widely used, but is rather time-consuming and challenging. The culture-negative cases do not necessarily mean the absence of spirochetes in a sample. The failure to culture the spirochetes might be caused by multiple vector-, spirochete-, media-, or cultivation condition-related factors (Cerar et al., 2008, Ružić-Sabljić et al. 2014, Rudenko et al., 2016).
Nowadays, the priority of all used techniques is redirected from simple detection of pathogen in either environmental sample or clinical sample, to simultaneous detection and identification of spirochete species (or possible coinfection agents). Considering the high possibility of the presence of multiple pathogens in tick vectors, the other question is whether to use singleplex or multiplex formats for their detection/identification. Fluidic microarrays allow the assessment of multiple tick-borne pathogens simultaneously (Vayssier-Taussat et al. 2013).
Use of proteomic methods to detect presence of some relapsing fever Borrelia in the hemolymph of ticks provides additional options for borrelial detection in vectors (Fotso Fotso et al. 2014).
These methods provide invaluable research tools and facilitate epidemiological studies, but their clinical relevance is debatable. Detection of a pathogen in the vector does not imply that it has been successfully transmitted to the host upon which the tick has fed. Transmission dynamics are complex and multifactorial, and beyond the scope of this review. Home-use diagnostic kits are available and allow individuals to test collected ticks for the presence of Lyme borreliae. The reliability of these tests has been highly debated. Tick bites are frequently unnoticed and might only demonstrate that you have been in a risk environment, but do not necessarily correlate with any infectious consequences. That is why, the use of such tests is of limited value for diagnosis, but can be useful for epidemiological studies.
Recommendation
Tick testing as supportive data for identification of LB endemic regions; correct selection of PCR target based on the final goal of tests and sample nature; reanalysis of tested sample targeting different genomic loci; and to consider the presence of coinfection with multiple pathogens as highly possible.
Clinical Diagnosis of LB and Supportive Diagnostic Strategies
A reliable clinical diagnosis of LB is only evident to the nonexpert physician when a typical erythema migrans (EM) is present (Stanek and Strle 2003). Since the large majority of LB symptoms have minimal diagnostic value because of their lack of specificity, diagnosis of LB might be challenging for general practitioners in patients without EM (Strle and Stanek 2009). Generally, there exists a tendency toward overdiagnosis of chronic LD (Sigal 1996, Koedel et al. 2015, Czupryna et al. 2016). Although different diagnostic approaches (mentioned later) have been explored, to date, the only recommended supportive tests used are serological confirmation. Serological results alone are insufficient to distinguish whether the patient suffers from an acute or reinfection that needs treatment, or is only seropositive because of a past infection. This might be especially problematic for individuals who are frequently exposed to ticks and therefore have a high risk of reinfection. However, even in low-risk areas, the positive predictive value of serological tests can be very low (Lantos et al. 2015), meaning that, clinical manifestations still remain crucially important criteria for a reliable diagnosis of the disease. Factors that need to be integrated for a reliable diagnosis are therefore the occurrence of compatible symptoms, serological results, and risk of tick exposure. Figure 1 provides an overview of different important steps in the diagnosis of LB.
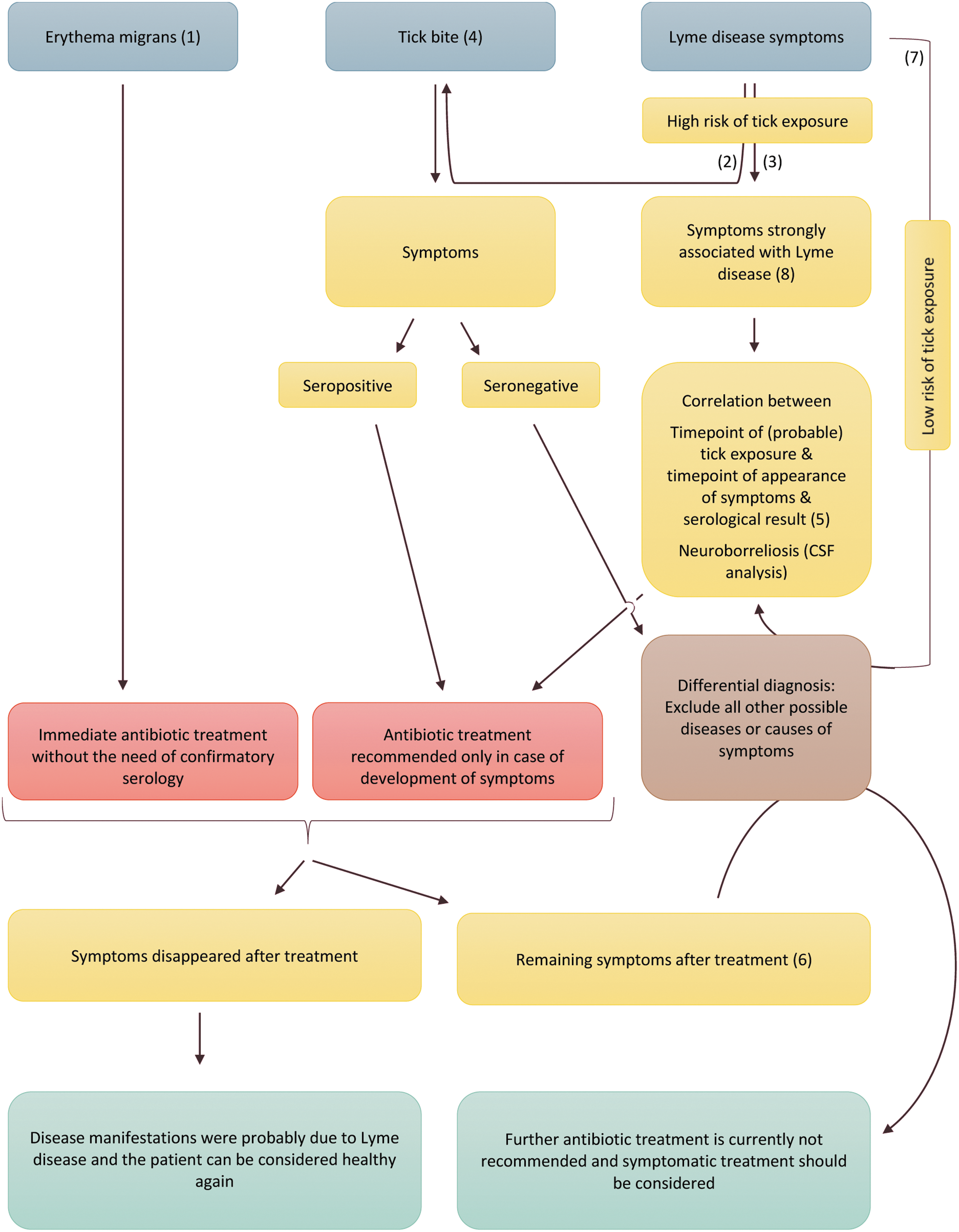
No diagnostic tests currently exist that provide a yes or no result for acute Lyme borreliosis (LB), thus clinical signs still remain the major factor for deciding whether antibiotic treatment is necessary. In case of unclear symptoms, the risk of tick exposure and serological tests should be considered to support the diagnosis. Represented in blue are three possible scenarios for which LB should be considered: the patient presents with the characteristic skin manifestation erythema migrans (EM) or a recent tick bite. A third possibility is that the patient's symptoms might be compatible with LB. As can be readily deduced from this schematic representation (yellow: clinical decision), EM is the least complicated case and should be treated (red) immediately without need for further testing. The situation gets more complicated if the patient cannot remember a tick bite [which can occur in up to 2/3 of cases (Hofhuis et al. 2013)] and/or has nonspecific symptoms. Green: Final outcome. (1) EM: Incubation time between 3 days and 1 month. Red skin lesion that might, in some cases, be associated with slight itching or burning and that expands around the site of the tick bite. EM can be distinguished from a simple tick bite-induced irritation of the skin by the fact that it has a minimum diameter of 5 cm. EM is often associated with nonspecific symptoms like fatigue, headache, fever, or malaise and can occur at different locations on the same patient (multiple EM) (Godar et al. 2015). (2) In case a patient presents with symptoms that have been associated with, but are not clearly specific, for Lyme disease (LD), an assessment of the risk of prior tick exposure should be done. For this purpose, the following questions might be considered: Does the patient pay attention to ticks? Did the patient maybe notice in the recent past an itching and scratched something small off from his body? Does the patient have pets that often have ticks? How much time does the patient spend outdoors in the green? Has the patient recently been on holidays in a risk area? Season or weather conditions supporting high activity of ticks (might also be interesting to exclude other possible infections)? (3) Try to estimate, based on the symptoms (early or late stage), the time point of infection and check if the season and/or weather conditions have been such that at the possible time point that infection ticks might have been active. Ticks are active during wet, not too hot, seasons of the year. For more information on factors affecting tick activity please refer to reference (Medlock et al. 2013). (4) If a patient shows up with a tick bite, appropriate and early removal of the tick can prevent transmission of LD, however, since the transmission efficiency and kinetics depends on the Borrelia strain (Crippa et al. 2002), an early transmission cannot reliably be excluded (Kahl et al. 1998), and the patient should be monitored for the development of symptoms and treatment considered only if such appear. In case the tick has been damaged or removed late, a short-term prophylactic antibiotic (oral or cutaneous) treatment might be considered (Warshafsky et al. 2010, Piesman and Hojgaard 2012, Piesman et al. 2014). However, due to the small time period during which this method is efficacious and the high number of patients who need to be treated for a successful outcome (Hofhuis et al. 2013), controversial opinions exist on this procedure. (5) Please consider, in this study, the fact that patients are not necessarily protected after a first course of LD and reinfection can occur (Nadelman and Wormser 2007, Khatchikian et al. 2014, Shapiro 2015). In this case, the interpretation of serological results might be complicated. (6) In case of persistent flu-like symptoms after appropriate treatment of EM, consider coinfections with other tick-borne pathogens (Godar et al. 2015). Make sure that treatment has been done in the correct way, otherwise consider retreatment with an appropriate method. In case of a post-treatment chronic course of LD, other possible reasons for the symptoms should be excluded. (7) Make sure that the symptoms have only occurred after potential exposure to a tick bite and they did not already exist before the tick exposure. In case of nonspecific disease manifestations, ask the patient if he might recall symptoms similar to EM in the past. (8) To have a better overview of the symptoms that are frequently associated with LD consult for example Stanek et al. (2012) and Koedel, et al. (2015).
To Date, Only Serological Tests are Recommended to Support the Diagnosis of LB in the Absence of EM
In cases where EM is clearly evident, serological tests are not needed and treatment should start immediately (Stanek et al. 2012). In patients who do not develop EM, serological tests are recommended to support the diagnosis (Aguero-Rosenfeld et al. 2005). Initial problems with the specificity and sensitivity of serological tests have resulted in controversial statements on their efficacy to support diagnosis of acute LB. Recently, serological tests have been optimized switching from a single Borrelia strain cell extract to the use of a combination of more precisely chosen recombinant antigens or synthetic peptides (Fang Ting et al. 2000, Goettner et al. 2005). Previously, a two-tier test approach, in which the presence of antibodies is first tested by a highly sensitive ELISA and, in case of a positive result, further confirmed by a highly specific immunoblot, was recommended (Branda et al. 2010, Koedel et al. 2015).
Noteworthy, the reported accuracy of ELISAs and immunoblots varies throughout Europe and a recent study revealed no overall benefit of two-tiered tests over single tests (Leeflang et al. 2016). Only early-stage patients (symptoms <6 weeks) might still be seronegative, as they have not developed antibodies yet. Therefore, diagnosis of LB should be reevaluated in seronegative late-stage patients (Stanek et al. 2012). Low antibody titers have been observed after antibiotic treatment, indicating that the induced B cell immune response is probably not very long-lived and robust. Especially, patients where Borrelia took longer to disseminate seem to develop long-lived antibody titers less efficiently (Hammers-Berggren et al. 1994, Aguero-Rosenfeld et al. 1996, Nowakowski et al. 2003, Elsner et al. 2015). Recent mouse studies have shown that Borrelia have a direct effect on the mouse B cell response (Hastey et al. 2012, 2014, Elsner et al. 2015a, 2015b). However, the underlying mechanism in humans requires further investigation. Showing the induction of strain-specific immunity (but not cross-protective), mouse and human studies together (Khatchikian et al. 2014) may explain reinfection of LB. Consequently, previous Borrelia infections must be taken into account when considering serological testing (Nadelman and Wormser 2007).
Despite the described improvement of these tests, we still face the problem of nonstandardization and inappropriate application of current serological tests (Ang et al. 2011, Muller et al. 2012, Markowicz et al. 2015, Leeflang et al. 2016). Different (in-house) assays and result interpretation remain a major problem (Fallon et al. 2014) that should be solved in the future by the implementation of a universal and worldwide (or Europe/USA wide) diagnostic standard test, or as a minimum, use of internationally agreed standards and participation in quality control schemes. However, the problem remains (especially among high-risk groups) to distinguish between an acute and a resolved infection. Future studies should therefore focus on the development of new strategies that would allow a yes or no result.
Noteworthy, serological tests should not be used as a proof of efficacy of the antibiotic treatment. Although antibody titers generally decrease after antibiotic treatment; however, patients may remain seropositive for years after the infection in the absence of active disease (Hammers-Berggren et al. 1994, Aguero-Rosenfeld et al. 1996, Lomholt et al. 2000, Kalish et al. 2001, Glatz et al. 2006, Kowalski et al. 2010). Instead, the disappearance of symptoms is a more reliable sign of cure.
When neuroborreliosis is suspected, detection of intrathecally produced anti-Borrelia antibodies significantly supports the diagnosis. However, results might be negative at early stages and more often in children (Christen et al. 1993). Measurement of Borrelia-specific antibodies in cerebrospinal fluid (CSF) cannot be used to assess the efficiency of treatment (Koedel et al. 2015).
Since antibiotic treatment is generally considered efficient, differential diagnosis is crucial in case of a chronic course of the disease (Halperin 2015, 2016, Hjetland et al. 2015, Markowicz et al. 2015, Rebman et al. 2015, Wills et al. 2016). A chronic course has been observed in patients infected by Borrelia, viral and nonviral pathogens, such as Epstein–Barr virus (glandular fever), Coxiella burnetii (Q fever), or Ross River virus (epidemic polyarthritis) (Hickie et al. 2006, Galbraith et al. 2011, Aucott et al. 2013, Katz and Jason 2013), and the underlying causes are not clear. In this context, the general health status and/or the lifestyle of the patient should also be considered. In general, immunocompromised or otherwise not completely healthy patients might be at higher risk to develop chronic symptoms after treatment. Patients with hematological malignancies, for example, seem to suffer more often from disseminated disease and more frequently require retreatment (Maraspin et al. 2015). In nonimmunocompromised cases, where symptoms continue to persist even after appropriate antibiotic treatment, it is currently not recommended to prolong the treatment. Clinical studies have shown that the risk of side effects outweighs any potential therapeutic benefits (Klempner et al. 2001, Krupp et al. 2003, Koedel et al. 2015). In these cases, coinfections with other tick-borne diseases or other possible causes of the symptoms should be excluded (Belongia 2002, Swanson et al. 2006, Berghoff 2012, Godar et al. 2015) and symptomatic treatment considered (Koedel et al. 2015). Only in late neuroborreliosis is prolongation of the antibiotic treatment justifiable in cases of persistent CSF lymphocytic pleocytosis (Koedel et al. 2015).
In rare cases, Borrelia can cause problems with the heart and vascular system, and might be considered an underlying cause of stroke-like symptoms in patients who otherwise have no obvious risk for cardiovascular diseases (Zajkowska et al. 2015, Allen and Jungbluth 2016). Full description of LB clinical manifestations and their diagnosis have been recently reviewed by Stanek et al. (2011).
When encountering a tick bite, correct and early removal of the tick is a good way to reduce probability of infection. In Europe, only about 2% (Wilhelmsson et al. 2016) and in USA, about 1% (Heymann and Ellis 2012) of patients bitten by a tick develop LB. Detection of spirochete DNA in ticks alone does not necessarily mean successful pathogen transmission, which is why the value of this test has limited diagnostic value for LB (ESGBOR 2013), but is useful for epidemiological studies (Reye et al. 2010) to define risk areas. In this context, NGS is a new emerging technique that allows screening of the same tick in parallel for various tick-borne pathogens, with the potential of getting more detailed information about coinfections of ticks and identification of new, yet unrecognized pathogens (Vayssier-Taussat et al. 2013, Michelet et al. 2014). As transmission of Borrelia (and indeed other pathogens) depends on the length of tick attachment, measurement of scutal and coxial indexes can indicate the duration of attachment (Kahl et al. 1998, Crippa et al. 2002, Gray et al. 2005, Meiners et al. 2006, Tijsse-Klasen et al. 2011). In the absence of an EM and the presence of other LB-related symptoms, seroconversion can be used for supportive diagnosis. However, in the absence of symptoms, seroconversion is no indication for antibiotic treatment as a study in a Swiss risk group demonstrated that only 2% of patients who seroconverted developed clinical LB (Fahrer et al. 1991). Thus, as tick bite is a poor predictor of disease, treatment is advisable only upon appearance of LB symptoms.
Recommendation
Clinical diagnosis alone, given a history of potential exposure and presence of EM, can be sufficient; however, clinical interpretation should generally be made in conjunction with supporting laboratory findings to reach a reliable diagnosis.
Alternative Strategies Explored for the Diagnosis of LB but Not on the List of Recommended Tests (ECDC 2016)
Direct detection of Borrelia in the peripheral blood, other body fluids, or tissues by microscopy or molecular methods can be used as strong additional evidence in the diagnosis of LB, but might have limited significance when used alone (Aguero-Rosenfeld et al. 2005). The sensitivity of PCR on skin biopsies is significantly higher than some other molecular tools; however, recognition of the EM itself is the best diagnosis for LB (Aguero-Rosenfeld et al. 2005). Nevertheless, this provides useful research data regarding strain prevalence and virulence, and provides insights into deciphering pathogenesis of LB (Strle et al. 2013). Cultivation of Borrelia from patient samples might be an alternative method to detect viable Borrelia, but is both time-consuming and challenging (Rudenko et al. 2016). As such, cultivation is best reserved as a research tool.
Lymphocyte transformation tests (LTT) have been explored for their potential to overcome the diagnostic gap in LB patients without EM, but before seroconversion and in reinfected seropositive patients. This assay measures lymphocyte proliferation in vitro after stimulation with B. burgdorferi-specific antigens. Currently, results are contradictory and consequently LTT is not recommended as a routine diagnostic tool (Mygland et al. 2010, Dessau et al. 2014). T cell ELISPOT is another in vitro stimulation assay currently explored and improved (Jin et al. 2013). More direct methods measuring peripheral blood levels of specific cell subpopulations (CD57+) cells (Marques et al. 2009) or antigen-reactive cells (Tario et al. 2015) by flow cytometry and direct measure of CXCL13 levels in the CSF or metabolites within serum (Molins et al. 2015) are also not at a point yet to be used reliably for clinical diagnosis. CD57 cell counts seem not to be reliable as a validation study found no difference between patients and healthy controls (Marques et al. 2009). Demonstration of CSF CXCL13 as an activation marker is not specific for LB, its absence is believed to have some value in excluding neuroborreliosis (Rupprecht et al. 2014), and it might become a valuable supportive tool to estimate treatment efficiency in case of neuroborreliosis (Senel et al. 2010, Schmidt et al. 2011, Koedel et al. 2015). Problems with human leukocyte antigen (HLA) types and identification of epitopes for antigen-specific T cell staining are challenges that need to be addressed to validate the potential of Borrelia-specific T cell counts in peripheral blood to support diagnosis of LB. Metabolite measurement is a future strategy under investigation, but needs further validation.
Generally, the detection of Borrelia DNA within ticks as well as other methods discussed above should be considered valuable research tools providing useful information about the epidemiology of tick-borne diseases in general and LB particularly. As with serological methods, their value is lower when used alone. Combination of diagnostic tests and clinical signs provides a more robust and timely diagnosis of disease. In any case, interpretation of test results and clinical diagnosis of LB remains controversial and should currently be restricted to experts.
Development and application of new molecular tools allow the detection and differentiation among LB or relapsing fever spirochetes, clearly separating B. burgdorferi sensu lato spirochetes from recently described B. miyamotoi (Margos et al. 2008, Rudenko et al. 2009, Venczel et al. 2015). Combination of multilocus PCR with electrospray ionization and mass spectrometry has recently been investigated for the detection and genotyping of Borrelia species in whole blood (Eshoo et al. 2012).
Recommendation
These tests are valuable research tools providing useful information about the patient's immune response, but interpretation for clinical diagnosis has not been clearly shown and should currently be restricted to specialized laboratories.
Diagnostics Within Symptomatic Animals
Veterinary infections are less well-documented and benefit from laboratory confirmation to ensure correct diagnosis. This is particularly important as EM lesions have not been reported in animals and clinical signs are often common to several pathologies. As for human cases, serology is the primary diagnostic approach used, sometimes supported by the use of PCR. Despite the absence of EM, cardiac and neurological signs and lameness have been reported among companion animals (Hovius et al. 1999, Krupka and Straubinger 2010, Agudelo et al. 2011). Most veterinary cases have focused upon lameness in dogs with positive serology, although this does not necessarily establish borrelial causality for this condition. Rapid immunochromatographic tests are often used in veterinary private practice to aid diagnosis; however, these assays have not necessarily undergone the rigorous quality control applied to human serodiagnostic tests (Savić et al. 2010).
Relapsing Fever Diagnostics
Clinical diagnosis of relapsing fever infections
In general, the clinical presentation of relapsing fever borreliosis is significantly distinct from that of LB. The possible exception to this being the appearance of a skin rash that challenges the previously believed “pathognomonic” EM, caused by the borrelial agent carried by Amblyomma americanum ticks in the United States, known as STARI (Masters et al. 2008, Borchers et al. 2015).
Human infection by recently described B. miyamotoi usually results in fever and associated flu-like signs (headache, chills, fatigue, myalgia), occasionally with neurological complications such as meningoencephalitis (Fonville et al. 2014, Krause et al. 2015).
Relapsing fever, as its name suggests, results in relapsing febrile episodes interspersed by afebrile periods. This is often accompanied by jaundice, muscle pain, headaches, and sometimes involvement of major organs (Borgnolo et al. 1993). This clinical picture can often be mistaken for other infections such as malaria that tend to overlap geographically in many endemic regions (Lundqvist et al. 2010).
Laboratory Diagnostics for Relapsing Fever
Microscopy
Although for LB, microscopy is not suitably sensitive for detection, this has been the diagnostic gold standard for detection of many relapsing fever spirochetes. Darkfield examination of unstained wet preparations, Giemsa or silver-stained blood or tissue sections, or immunofluorescence methods has been successfully used. Despite its frequent use, even relapsing fever can be difficult to detect using microscopy with some species such as B. crocidurae typically producing lower blood burdens than others, like B. duttonii. For such cases, a centrifugation step to concentrate the sample can be beneficial (Larsson and Bergström 2008). Furthermore, detection is restricted to times of febrile episodes when spirochetes are present at detectable levels. On a cautionary note, various artifacts can share the size and helical shape of spirochetes when viewed by darkfield microscopy, but tend to not show the typical gyrating spirochete-characteristic movement. Microscopy will not provide information regarding the infecting species.
Recommendation
Microscopic methods lack both sensitivity and specificity, but can add value when used in conjunction with other methods. Sample concentration can offer distinct benefits.
Cultivation
Cultivation methods for detection of Borrelia have been particularly challenging, some members of the genus being particularly refractory to cultivation (Cutler et al. 1994), while others are cultivable, but only in a complex medium. Huge advances were made with the formulation of BSK medium with a commercial variant BSK-H supporting the growth of LB strains (Barbour 1984). Relapsing fever strains appear more diverse in their requirements. B. miyamotoi for instance appears to prefer the MKP medium (Wagemakers et al. 2014) or high serum concentrations (Margos et al. 2015). On a cautionary note, these preferences might reflect batch variations of composite ingredients that can vastly influence performance of these “home-made” media (Cutler personal observation). Collectively, cultivation should be considered a low-yield procedure, but vital for recovery of much-needed strains for research purposes (Ružić-Sabljić et al. 2014).
Animal inoculation or xenodiagnosis (allowing infected ticks to feed upon a test animal) has been used for primary recovery of isolates before cultivation in an axenic medium (Schwan et al. 2012, Naddaf et al. 2015). It must be remembered that some species are refractory to growth in most animal models, such as B. recurrentis.
Recommendation
Cultivation is low yield, time-consuming, and expensive, and thus poorly suited to support diagnosis. Nevertheless, it still has a vital role for recovery of isolates for research purposes.
Serological Diagnosis
For the relapsing fever group, specific serology can be undertaken using GlpQ protein as antigen. GlpQ is absent from LB species, thus facilitating its specificity for diagnostic purposes (Fritz et al. 2013). Alternatively, BipA can also serve as a differential antigen present in relapsing fever spirochetes, but absent from the LB group (Lopez et al. 2010). As acutely presenting patients may not have had sufficient time for seroconversion, serology is best reserved for retrospective diagnosis.
Polymerase Chain Reaction
PCR provides a valuable diagnostic approach in acutely ill patients (Mediannikov et al. 2014). This overcomes the poor sensitivity of microscopy and can either be used to diagnose relapsing fever borreliosis or to further characterize the infecting spirochete. The absence of GlpQ in LB species makes it a specific target for detection of relapsing fever spirochetes (Takano et al. 2014). Other assays can either speciate specific relapsing fever borreliae or be designed to detect a single member of the relapsing fever clade such as B. miyamotoi (Elbir et al. 2013, Reiter et al. 2015). The limitation of this approach is having an appropriate sample that is likely to contain spirochetal DNA. Blood collected during febrile episodes and CSF samples have given good results (Gugliotta et al. 2013). Furthermore, in highly relapsing fever endemic areas, it is possible to have positive PCR results unrelated to current clinical pathology (Cutler et al. 2010).
Recommendation
PCR can provide useful supporting information, but multiple available assays must be properly standardized, and are hampered by sample timing, type, and quality.
Next-Generation Sequencing
NGS offers huge potential and data have only recently been forthcoming, limiting comprehensive appraisal at this stage. With the exception of dermatoborreliosis, in this study, the challenge is which diagnostic sample type to investigate for LB in the absence of focal lesions. Sensitivity can be further improved, especially among high levels of host DNA. Care should be taken to avoid bias when using target enhancement strategies to amplify low-copy-number targets. Data analysis represents an additional computational challenge. NGS methods combined with bioinformatics tools might overcome the limitations of culture-connected techniques or some molecular protocols. However, the extreme diversity of spirochetes from B. burgdorferi sensu lato complex reduces the usefulness of NGS as it does not differentiate the pathogenic to human spirochete strains from those that were never connected with human LB. In addition, this offers a means of assessing rank abundance, evolving genomic profiles such as those corresponding to vector adaptations (Gatzmann et al. 2015), and fluctuations over time providing valuable insights into host–microbial interactions (Strandh and Råberg 2015).
To date, enrichment techniques can only partially overcome sensitivity problems caused by the giant excess of host DNA (vector, endosymbiont, and other microbial DNA) compared to the low proportion of target DNA (borrelial DNA in ticks is <0.01% of total DNA within field-collected nymphal ticks) (Carpi et al. 2015). This can impact, upon successful detection, only about a third of infected ticks revealing positive Borrelia NGS data (Carpi et al. 2015).
Recommendations
NGS offers huge potential and data have only recently been forthcoming, limiting comprehensive appraisal at this stage. Sensitivity can be further improved, especially among high levels of host DNA. Care should be taken to avoid bias when using target-enhancement strategies to amplify low-copy-number targets. Data analysis represents an additional computational challenge.
Fact Sheets and Resources
Several excellent fact sheets have been produced by ECDC to provide information on LB and tick-borne relapsing fever. Furthermore, more specific resources can be obtained from European study group for LB (ESGBOR;
Knowledge Gaps and Future Perspectives
The poor sensitivity of direct detection methods coupled with the poor predictive value of indirect serological methods, particularly in less typical clinical presentations, presents a significant diagnostic challenge. Serology is further challenged by the requirement for sufficient time in order for the host to produce antibody responses to enable detection. Detection of the host response to infections provides a particularly attractive prospect for LB where organism loads are typically low. Indeed, levels of CXCL13 have shown promise for neuroborreliosis, but require further validation (Senel et al. 2010, Schmidt et al. 2011). It is possible that signature biomarker profiles might have value, but whether this would vary too much between individuals or indeed with differing genetic variants of borreliae awaits investigation. Another diagnostic approach under exploration is based on targeted proteomics. By selected reaction monitoring mass spectrometry, specific Borrelia proteins can be detected and quantified in skin biopsies (Schnell et al. 2015). The powerful new emerging technologies provide insights into our understanding of the dynamic interactions of borreliae with their vector, host, and other organisms, with the possibility of disclosing opportunities for future intervention.
Concluding Remarks
During these brief guidelines, we have attempted to highlight the strengths and limitations of various diagnostic methods used to diagnose borrelial infection. No single approach is suitably robust for this purpose, thus making interpretation challenging. Furthermore, laboratory diagnostics need to be viewed in conjunction with potential exposure and compatible clinical features.
Footnotes
Acknowledgments
This article was done under the frame of EurNegVec COST Action TD1303. W.J.C. and J.K. are funded by the Luxembourgish Ministry of Research (project Marlybor, REC-LNSI-20110308). W.J.C. and J.K. were supported by a fellowship from Aides à la Formation Recherche (grant no. 4660265 and no. 3986187) of the Fonds National de la Recherche, Luxembourg.
Author Disclosure Statement
No competing financial interests exist.