
Abstract
Background:
Crimean-Congo hemorrhagic fever virus (CCHFV) was detected for the first time in Mauritania in 1983 and several CCHFV outbreaks were reported in the following years. The last human case was diagnosed in 2015. However, no recent data exist about the prevalence of CCHFV in animals, although it is already described that prevalence studies in animals serve as good risk indicators. CCHFV can cause a severe hemorrhagic fever with a high case fatality rate in humans. Therefore, a precise risk assessment on the basis of updated data is very important. This article gives an overview about the current CCHFV prevalence in cattle in Mauritania.
Methods and Findings:
A seroprevalence study was carried out using 495 cattle sera from Mauritania, which were collected in the year 2013. The sera were analyzed by an inhouse CCHFV-IgG-ELISA. As second screening test, an adapted commercial CCHFV-IgG-ELISA was performed. Inconclusive sera were additionally tested by a modified commercial CCHFV-IgG-IFA. All assays showed high diagnostic sensitivity (>95%) and specificity (>98%). The overall prevalence of CCHFV-specific antibodies found in Mauritanian cattle was 67%, ranging from 56% to 90% in different provinces.
Conclusion:
This study shows a very high CCHFV-specific antibody prevalence in cattle in Mauritania. It is the highest seroprevalence detected in Mauritania so far. This strengthens the hypothesis that CCHFV is a serious and ongoing threat for public health in Mauritania.
Introduction
C
In contrast to humans, animals do not seem to develop obvious clinical symptoms and only a seroconversion is observed after a viremia of up to 2 weeks (Causey et al. 1970, Gonzalez et al. 1998, Gunes et al. 2011). However, the detection of CCHFV-specific antibodies in animals is a good indicator for CCHFV circulation in a region and can be used to define risk areas.
CCHFV was already found in many countries of Africa, Asia, and Europe (Hoogstraal 1979, Whitehouse 2004, Bente et al. 2013).
In Africa, CCHFV has been detected for the first time in Belgian Congo (today Democratic Republic of Congo) in 1956 (Simpson et al. 1967, Woodall et al. 1967). Since then, CCHFV was discovered in a number of African countries including Mauritania and its neighbor countries Senegal and Mali (Hoogstraal 1979, Saluzzo et al. 1985a, Traore et al. 2005). Only a few incidental seroprevalence studies were carried out in Mauritania in humans and animals in the context of human CCHF cases in 1983, 1988, and 2003 (Saluzzo et al. 1985a, Gonzalez et al. 1990, Nabeth et al. 2004), indicating overall prevalence rates of 9% to 32% in ruminants (Saluzzo et al. 1985b, Gonzalez et al. 1990, Nabeth et al. 2004).
Given the ongoing occurrence of CCHF cases in humans in Mauritania, we have determined the seroprevalence in 495 sera obtained from bovines from different regions in Mauritania in 2013. Sera were screened by an inhouse CCHFV-IgG-ELISA, an adapted commercial CCHFV-IgG-ELISA (VectorBest, Novosibirsk, Russia), and a newly modified commercial CCHFV-IgG-IFA (Euroimmun, Lübeck, Germany).
Materials and Methods
Ethic statement
Serum samples were collected according to fundamental ethical principles for diagnostic purposes in the framework of a governmental program for the national surveillance called “Mauritanian epidemiological survey network (REMEMA)” from 1998. This program focuses mainly on contagious bovine pleuropneumonia, Rift Valley fever, foot and mouth disease, peste des petits ruminants, rabies, and pasteurellosis in camels.
Study site and serum collection
Mauritania has a size of 1,030,000 km2, of which 90% are located within the Sahara. Most of the human population and livestock are living in the south. For the current prospective study, serum samples were collected in 2013 at different locations within 6 out of the 13 regions of Mauritania (Assaba [n = 80], Gorgol [n = 66], Guidimaka [n = 51], Hodh el Chargui [n = 50], Hodh el Gharbi [n = 65], and Nouakchott [n = 183]) by the Mauritanian State Veterinary Laboratory, the Centre National de l'Élevage et de Recherches Vétérinaires (CNERV). The serum samples were not specifically collected for our study but for routine diagnostic monitoring on the Mauritanian livestock by CNERV. A total of 222 out of 495 cattle sera originated from two slaughterhouses, Nouakchott abattoir (n = 183), and Hodh el Gharbi abattoir (n = 39), which were sampled in the course of the normal slaughtering process and assayed by CNRRV also for the purpose of getting insight into the general infection status of the national cattle herd.
Reference sera
The negative reference serum panel consisted of 113 cattle sera from Germany. Sera were considered to be negative as neither an established Hyalomma marginatum population nor human CCHF cases nor the virus itself is present in Germany. Positive reference sera were collected in Albania in 2013 (n = 15) and in Macedonia in 2011 (n = 20). These sera were considered to be positive if the commercial CCHFV-IgG-ELISA and the commercial CCHFV-IgG-IFA were positive.
Commercial CCHFV-IgG-IFA
The commercial CCHFV-IgG-IFA adapted for ruminant sera (Mertens et al. 2015) was used to test the gamma-irradiated cattle sera at 1/20 serum dilutions in Tris-buffered saline with 0.1% Tween 20 (TBST). Goat antibovine IgG-FITC (Sothern Biotech, Birmingham, AL) diluted at 1/200 in TBST, containing 0.005% Evans Blue, was used as detection system.
Seroepidemiological investigation
Samples were tested by the inhouse CCHFV-IgG-ELISA (Mertens et al. 2015) according to a flow chart for the “Interpretation of ELISA and immunoblot test results” (Mertens et al. 2009). In addition, all sera were tested in the commercial CCHFV-IgG-ELISA (Mertens et al. 2015). Samples were considered to be positive if they were reactive in both ELISAs or equivocal in one ELISA and positive in the other. Inconclusive results were clarified by commercial CCHFV-IgG-IFA.
Results
Adaptation of the commercial CCHFV-IgG-ELISA for testing West African cattle sera
The commercial CCHFV-IgG-ELISA is designed for human sera and was previously adapted for testing sera from European cattle (Mertens et al. 2015). As background staining reactions were slightly higher when sera from African cattle breeds were tested, a new cutoff was determined through receiver operating characteristic-based analysis and validated. In the newly adapted assay, OD values of 0.6 or lower were considered to be “negative” and OD values >0.6 were classified to be “positive.”
For this assay validation, 113 negative sera from Germany and 51 positive sera from Mauritania were used (Table 1). Owing to the absence of a gold standard in CCHFV serology, sera from Mauritania were defined as positive if they were reactive in the inhouse CCHFV-IgG-ELISA and in the CCHFV-IgG-IFA.
Confidence interval (95%) is shown in brackets.
CCHFV, Crimean-Congo hemorrhagic fever virus; D-SN, diagnostic sensitivity; D-SP, diagnostic specificity.
All negative sera were “true negative” and just one positive defined serum showed “false negative.” Overall, this leads to a diagnostic sensitivity (D-SN) of 98% and a diagnostic specificity (D-SP) of 100% (Table 1).
Modification and validation of the commercial CCHFV-IgG-IFA
The previously adapted commercial CCHFV-IgG-IFA (Mertens et al. 2015) was validated using positive sera from Mauritania (n = 50), Albania (n = 15), and Macedonia (n = 20) and negative sera from Germany (n = 48). Sera were considered “positive” if positive in the inhouse CCHFV-IgG-ELISA and in the adapted commercial CCHFV-IgG-ELISA. Reactive samples showed characteristic fluorescing granular structures in the cytoplasm of the cells, which are also described in the instructor's manual for human samples. GPC- and N-transfected cells show the same fluorescence picture (Fig. 1).
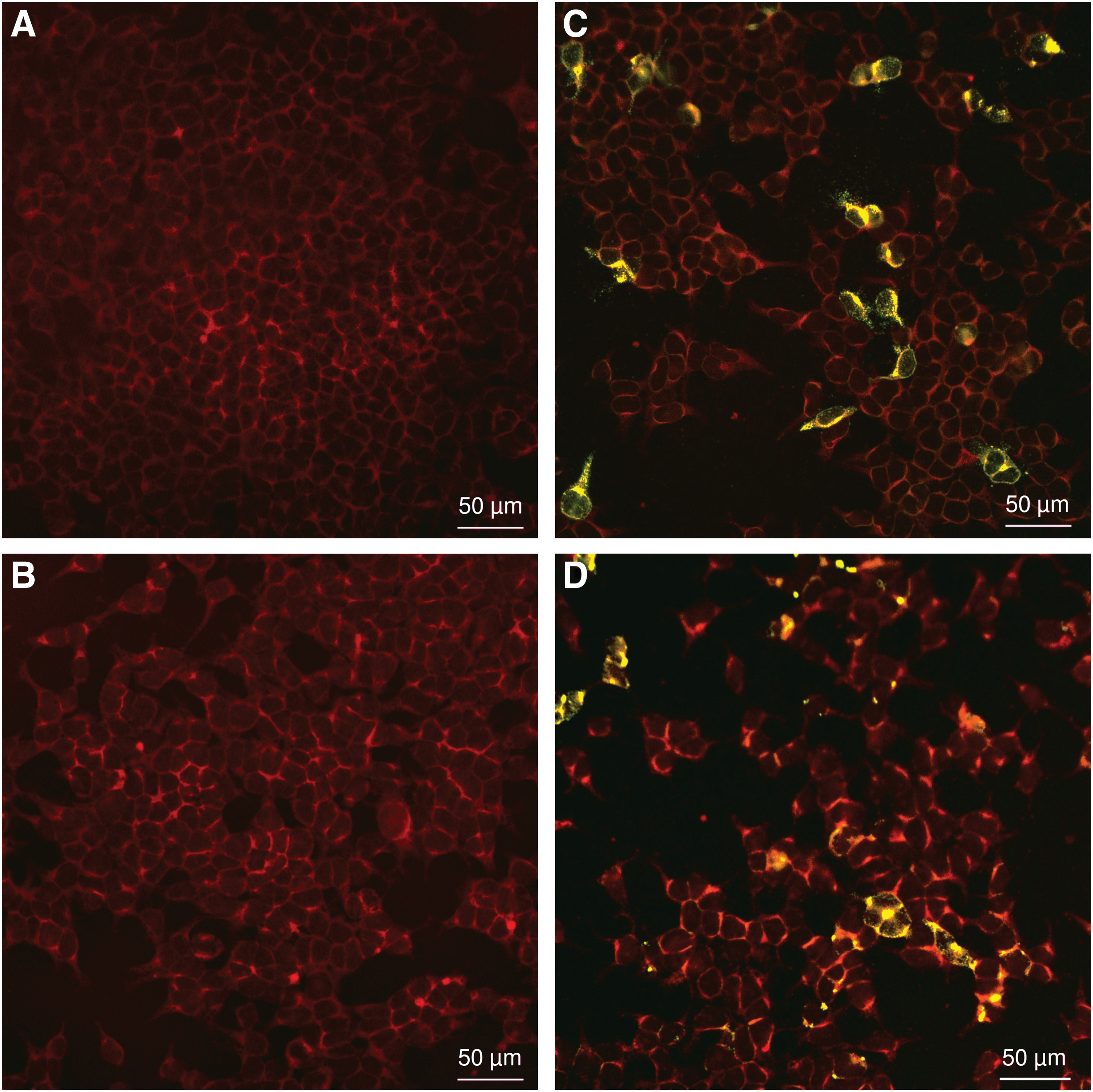
Commercial CCHFV-IgG-IFA. The commercial CCHFV-IgG-IFA was performed with sera from Europe and Africa. Negative sera (Germany) show no fluorescence for glycoprotein
Three samples from Mauritania and one sample from Albania gave a “false negative” result, one sample from Germany gave a “false positive” result and one sample from Mauritania gave an “equivocal” result (Table 1) so that the D-SN and D-SP were 95% and 98%, respectively (Table 1).
Seroprevalence study
A total of 333 (67%) out of 495 sera from Mauritania tested positive for CCHFV-specific antibodies. A total of 51 positive results (64%) were found in Assaba region, 37 (56%) in Gorgol region, 38 (75%) in Guidimaka region, 45 (90%) in Hodh el Chargui region, 17 (65%) in Hodh el Gharbi region, 23 (59%) in Hodh el Gharbi abattoir, and 122 (67%) in Nouakchott abattoir. The regional prevalence rates were, therefore, quite high and reached even up to 90% for Hodh el Chargui. Detailed results are shown in Figure 2 and Table 2.
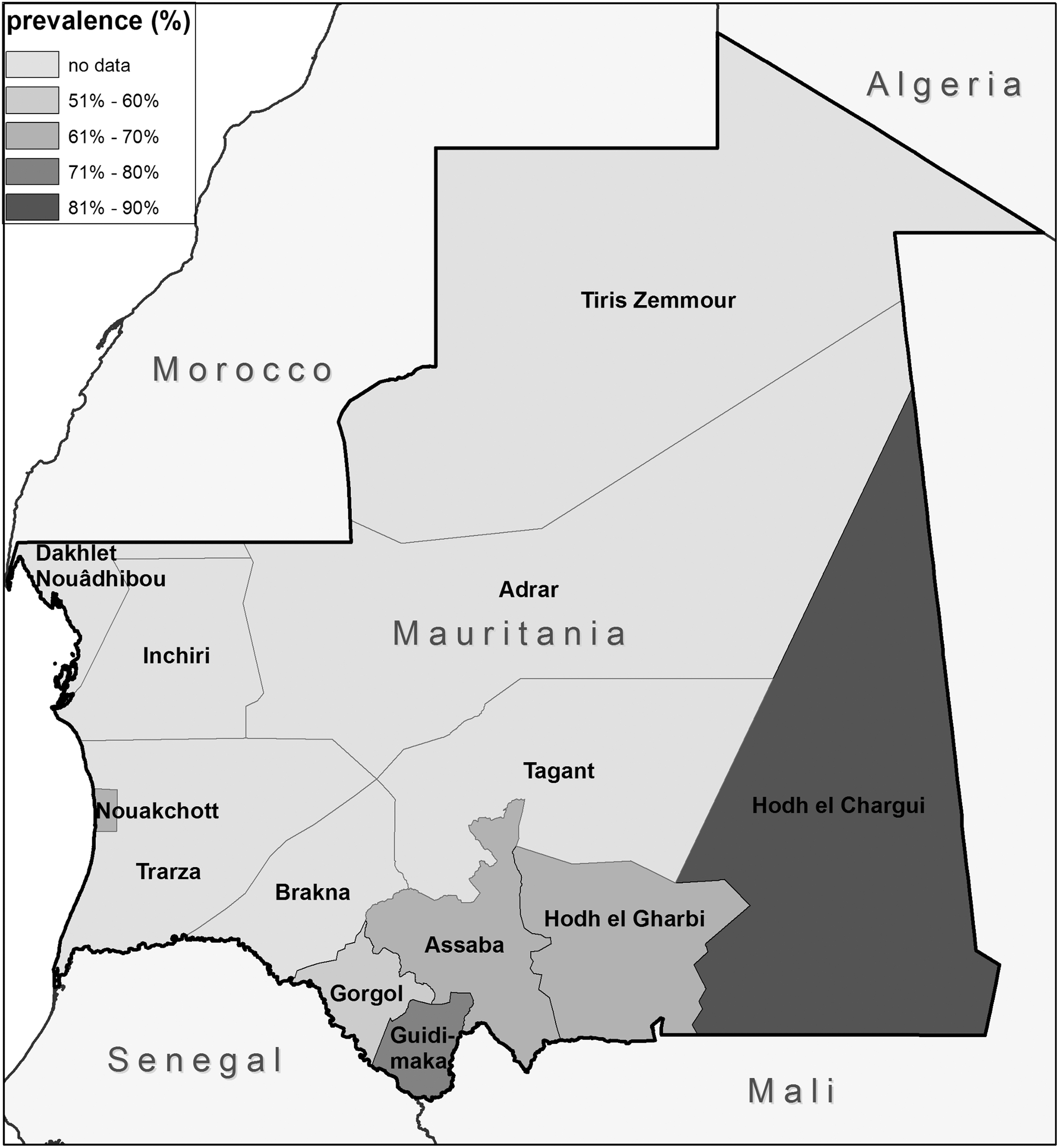
Map of Mauritania with sampled regions. All sera from Nouakchott and 23 out of 40 sera from Hodh el Gharbi were collected at the slaughterhouse. All other cattle sera were collected at different farms.
The confidence interval (95%) is shown in brackets.
n, number of samples; Pos, number of positive samples; Prev., prevalence.
Discussion
In this study, we investigated the prevalence of CCHFV in cattle in different regions of Mauritania. For this purpose, it was necessary to modify and validate the commercial CCHFV-IgG-IFA and to validate the commercial CCHFV-IgG-ELISA. Both modified assays showed a high D-SN and D-SP using defined positive and negative reference sera.
It is quite remarkable that using these assays we found a surprisingly high (67%) overall seroprevalence for the presence of CCHFV antibodies in cattle in Mauritania. In an earlier study from the 90s, seroprevalence rates in similar Mauritanian regions were found to be up to 26% and on average 18% (Gonzalez et al. 1990). A newer study, by Nabeth et al., included a relatively small number of samples (n = 97) from just two regions. It focused on animals from Nouakchott and Brakna in 2004 in direct surrounding of infected humans and showed a CCHFV-specific antibody prevalence of 18% (Nabeth et al. 2004). As no data were collected about Brakna region in this study, a direct comparison is difficult.
The sera from Nouakchott and part of the sera from Hodh El Gharbi were collected at the slaughterhouse and it was not possible to prove their primary origin. However, it is likely that these cattle came from surrounding pastry regions. Also, it is difficult to check the validity of the results of the former studies as only little or no data were given with regard to the D-SN and D-SP of the ELISAs used.
In general, only limited up-to-date studies on CCHFV distribution in African countries are available. Therefore, comparison of the results presented in this study with seroprevalence rates in other West African countries is only partly possible. Wilson et al. reported for the northernmost sampling site of Senegal a similar seroprevalence in sheep (75.7%) (Wilson et al. 1990). The prevalence rates could be linked to climatic conditions—especially rainfall—and he was able to show that the prevalence of IgG antibodies against CCHFV is highest in areas with warm arid clime, as is also present in Mauritania. The differences of the allover prevalence detected in Senegalese sheep are much lower than that detected in Mauritania in this study. Probably, one main influencing factor is the different vegetation and climate in South Senegal. In Niger, also similar seroprevalence rates were observed in the 1990s (Mariner et al. 1995); CCHFV-specific antibodies were present in 57.7% of 732 tested cattle.
In this study, we showed that 333 of 495 tested cattle have been infected by CCHFV, yielding seroprevalence even higher than those found in high endemic regions in Turkey, where about 1000 clinical human cases are seen every year of which up to 50 are of fatal outcome (Mertens et al. 2016). Cattle in slaughterhouses show similar high prevalence like the rest of the tested regions. This indicates the especially high risk for workers in this field.
Conclusion
The high CCHFV-specific antibody prevalence in Mauritania indicates an intense virus circulation in the human environment. This means an elevated CCHFV exposure risk especially for humans living and working outdoors in areas where Hyalomma ticks reside, for example, a large part of the pastoral and agricultural population in Mauritania. Surprisingly, human CCHF cases are reported in Mauritania only sporadically and it is not clear why this number is so low. The most likely reason may be a massive underreporting of cases, as the human population is inadequately informed about this potentially fatal disease. Educating medical personnel and risk groups such as veterinarians, slaughterhouse workers, and farmers is recommended in areas with a high seroprevalence. Another reason for the discrepancy between detected prevalence rates and reported human cases might be the circulation of a low or avirulent CCHFV strain. This can only be clarified through further characterization of circulating virus strains, prevalence studies in humans, and a better detection and reporting of human cases.
Taken together, this study will help to stress the importance of CCHFV infections in Mauritania and the need to implement public health measures for the prevention and diagnosis of CCHF.
Footnotes
Acknowledgments
This study was funded by the German Federal Foreign Office in the framework of the German Partnership Program for Excellence in Biological and Health Security (grant number 2513AA0374, URL:
Author Disclosure Statement
No competing financial interests exist.