
Abstract
For more than 95% of acute febrile jaundice cases identified through surveillance for yellow fever, a reemerging arthropod-borne viral disease, no etiological exploration is ever done. The aim of this study was to test for other arthropod-borne viruses that can induce the same symptoms in patients enrolled in the yellow fever surveillance in the Democratic Republic of the Congo (DRC). Of 652 patients included in the surveillance of yellow fever in DRC from January 2003 to January 2012, 453 patients that tested negative for yellow fever virus (YFV) immunoglobulin M (IgM) antibodies were selected for the study. Real-time polymerase chain reaction was performed for the detection of dengue, West Nile, Chikungunya, O'nyong-nyong, Rift Valley fever, Zika, and YFV. The average age of patients was 22.1 years. We reported 16 cases (3.5%; confidence interval [CI]: 0.8–5.2) of dengue (serotypes 1 and 2) and 2 cases (0.4%; CI: 0.0–1.0) of Chikungunya. Three patients were co-infected with the two serotypes of dengue virus. Three cases of dengue were found in early July 2010 from the city of Titule (Oriental province) during a laboratory-confirmed outbreak of yellow fever, suggesting simultaneous circulation of dengue and yellow fever viruses. This study showed that dengue and Chikungunya viruses are potential causes of acute febrile jaundice in the DRC and highlights the need to consider dengue and Chikungunya diagnosis in the integrated disease surveillance and response program in the DRC. A prospective study is necessary to establish the epidemiology of these diseases.
Introduction
Y
Along with yellow fever virus (YFV), several arthropod-borne viruses (“arboviruses”) transmitted by the Aedes mosquitoes such as Dengue virus (DENV), Chikungunya virus (CHIKV), Rift Valley Fever virus (RVFV), and Zika virus have emerged, causing outbreaks of febrile illness in many sub-Saharan African countries these last years.
CHIKV caused large epidemics in the DRC from 1999 to 2000 (Muyembe-Tamfum et al. 2003), in the Republic of Congo in 2011 (Moyen et al. 2014), in Senegal in 2015 and 2016 (WHO 2016b), and in Kenya in 2016 (WHO 2016a). Simultaneous outbreaks of Chikungunya and dengue were reported in Cameroon in 2006 (Peyrefitte et al. 2007), and in Gabon in 2007 and 2010 (Leroy et al. 2009, Caron et al. 2012). Moreover, Zika virus was found retrospectively in both human sera and mosquitos collected during the 2007 outbreak in Gabon (Grard et al. 2014). In eastern Africa, an outbreak of Rift Valley Fever spread from Sudan to South Africa causing disease in both humans and animals from 2006 to 2008 (Bird et al. 2009). In 1998, an outbreak caused by West Nile virus (WNV), arthropod-borne virus transmitted by Culex mosquitoes, was reported in DRC (Nur et al. 1999).
All these arboviruses cause a broad spectrum of disease, ranging from asymptomatic infection to severe undifferentiated fever. They can also progress to more complex secondary conditions, such as encephalitis, icteric hepatitis, or hemorrhagic diathesis, confounding the yellow fever diagnostic (Labeaud et al. 2011).
In the DRC, a central African country, yellow fever outbreaks were first reported in 1920 and 1928 (Matadi, Bas-Congo province), then in 1958 (Gemena, Equateur province and Doruma, Oriental province) (Courtois et al. 1960, Panthier et al. 1962). There was then a long period of silence during which no outbreak was reported until the late 1990s when notification of suspected cases of yellow fever resumed, reaching between 350 and 400 cases annually.
Considering this resurgence, the Direction de Lutte contre la maladie of the Ministry of Health set up yellow fever surveillance activities, following WHO recommendations. This surveillance facilitated the early identification and control of three laboratory-confirmed outbreaks in 2010 (Oriental) (WHO 2010), 2013 (Kasai-oriental) (WHO 2013), and 2014 (Oriental and Katanga) (WHO 2014), using an extensive case definition of suspected yellow fever. The surveillance also identified the recent YF outbreak imported from Angola in 2016 using the same strategy (Woodall and Yuill 2016). However, the number of laboratory-confirmed cases remains very low (less than 5%) even during outbreaks, and no etiological investigation is ever conducted in patients for whom yellow fever is not confirmed. Although other arboviruses may induce the same symptoms as yellow fever, the presence of these viruses is never tested in patients identified through the program. Moreover, little is known about the circulation of arboviruses in the DRC, although mosquito vectors have already been identified (Nur et al. 1999).
To identify other arboviruses of public health importance and potentially responsible for symptoms observed in suspected cases of yellow fever, we tested for the presence of DENV, WNV, CHIKV, RVFV, O'nyong-nyong virus (ONNV), Zika virus, and YFV in patients who tested negative for the YFV antibodies through the yellow fever surveillance in the DRC, between 2003 and 2012.
Materials and Methods
Patients and samples
In the yellow fever surveillance program, health zones and health facilities are responsible for reporting suspected cases of yellow fever. Suspected YF cases are defined as patients with an acute onset of fever followed by jaundice within 2 weeks of the first symptoms, and who test negative for malaria by thick blood smear or fail to respond to appropriate antimalarial treatment. Blood samples are collected from those patients in one10-mL dry Vacutainer tube (VWR International, France) and sent at +4°C to the Institut National de Recherche Biomédicale (INRB), the national public health laboratory. To confirm the yellow fever diagnosis, serum was obtained by centrifugation (10 min, 2000 g) and was tested using the immunoglobulin M (IgM)-capture ELISA test following the Centers for Disease Control and Prevention (CDC) protocol. Positive samples were sent to the regional reference laboratory for yellow fever at the Institut Pasteur in Dakar, Senegal for confirmation with more specific tests (i.e., plaque-reduction neutralization test).
From 2003 to 2012, 652 serum samples were collected from suspected cases of yellow fever in 10 of the 11 DRC provinces and were sent to the INRB. Of these samples, only five tested positive for yellow fever IgM antibodies. We selected 453 that tested negative for yellow fever antibodies and had a volume sufficient for further diagnostic exploration. The majority of patients were from the two northern provinces, including 168 (37.1%) patients from Oriental and 110 (24.3%) patients from Equateur (Fig. 1). In the other provinces, the number of patients ranged from 5 to 52. The mean age of patients was 22.1 years (range 4 months-77 years). The male-to-female ratio was virtually 1:1 with 239 (52.8%) men and 214 (47.2%) women (Table 1). We highlighted an increase of suspected cases in 2010 (175 cases, 38.6%) (Fig. 2), resulting from the yellow fever epidemic that hit the city of Titule in Oriental from July to September (location detailed in Fig. 1). In 2006, 32 (78%) patients were enrolled in August from Gemena town in Equateur. During the rest of the study period, there were no obvious concentrations of cases.

Map of arboviruses distribution in provinces of the Democratic Republic of the Congo. The specific health zones in which positive cases were detected are shaded in yellow for Chikungunya and blue for dengue viruses. Pie charts show positive (red) and negative (gray) samples tested in each province, with the exact number also specified. The city of Titule, where three cases of dengue were recorded in July 2010, is identified on the map. Color images available online at
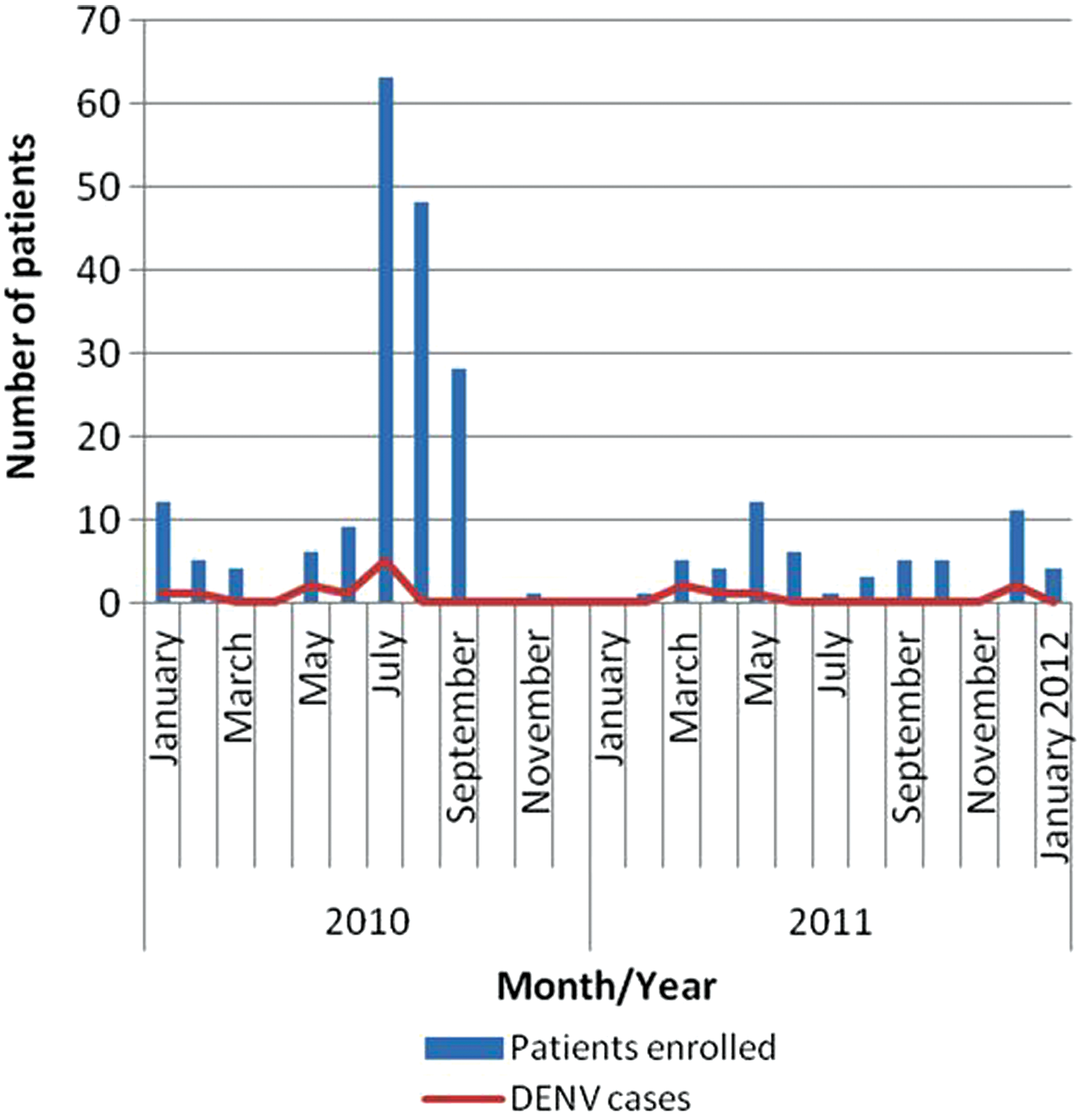
Evolution of the detection of dengue cases over time, from January 2010 to January 2012. Blue bars show the number of enrolled patients during each month. The red line connects the corresponding points of the number of dengue cases detected each month. Color images available online at
Molecular investigations
RNA extraction, reverse-transcriptase polymerase chain reaction and real-time polymerase chain reaction
Total viral RNA was extracted from 200 μL of serum and eluted in 120 μL of elution buffer using the EZ1® Advanced XL Biorobot (Qiagen, CA) with the EZ1 Virus Mini Kit v2.0 (Qiagen) according to the manufacturer's instructions. To synthesize cDNA, 50 μL of RNA extract was mixed with 50 μL of High Capacity cDNA Reverse Transcription Kit (Applied Biosystems™, Foster City, CA) and incubated in a 2720 thermal cycler (Applied Biosystem) according to the manufacturer's instructions.
Semi-quantitative TaqMan polymerase chain reaction (PCR) was performed on freshly obtained cDNA to detect DENV, WNV, CHIKV, RVFV, ONNV, Zika virus, and YFV (Table 2) (Drosten et al. 2002, Pastorino et al. 2005, Lanciotti et al. 2008, Leparc-Goffart et al. 2009). In a final volume of 25, 5 μL of cDNA were mixed with the TaqMan Universal PCR Master Mix (Applied Biosystems, NJ) and 0.2 μM of each primer and probe, except for RVFV for which we used 0.5 μM of each primer. The mixture was incubated in a 7500 Real-Time PCR thermal cycler (Applied Biosystems) for 40 cycles according to the manufacturer's protocol and the TaqMan PCR products were identified by comparison with standard curves using 7500 system SDS software. To type DENVs, the same protocol was performed with specific serotype primers and probes as described elsewhere (Leparc-Goffart et al. 2009). The probes used here were labeled with FAM-reporter and TAMRA-quencher (Applied Biosystems). Negative and positive controls were added in each run and all samples that tested positive were retested in duplicate to validate the results.
Ethical considerations
The study was conducted with the authorization of the DRC Ministry of Health and the WHO to supplement yellow fever surveillance data in the DRC. Data collected from the INRB laboratory database of yellow fever surveillance remained confidential, and results were made available to the Ministry of Health at the end of the study.
Results
Virological findings
Two viruses were detected in the sera collected from suspected cases of yellow fever. DENV was found in 16 (3.5%) samples and CHIKV in 2 (0.4%) samples. None of the other five arboviruses (YFV, WNV, RVFV, ONNV, and Zika virus) were detected. The dengue serotype-specific PCR assay has identified two serotypes (1 and 2) of DENV. Eleven patients were infected by DENV-2, two patients by DENV-1 and three patients by both serotypes.
Spatial and temporal distribution of cases
Most of the dengue cases were located in the north of the DRC, in Oriental (8 cases) and Equateur (4 cases). Four health zones were affected in each of these two provinces (Fig. 1). The remaining 4 cases were from western and central provinces. We reported two cases in Bas-Congo and one case each in the provinces of Kasai-Occidental and Kasai-Oriental. DENV-2 was found in all five provinces whereas DENV-1 was found only in the two northern provinces.
DENV was detected only in patients enrolled from 2010 (10 patients) to 2011 (six patients) (Fig. 2). Three of those from 2010 were enrolled from the town of Titule in Oriental, during the yellow fever outbreak there in July. CHIKV was detected in March 2011 from Equateur and Bandundu.
Discussion
Several arboviruses have emerged in recent decades, causing outbreaks in sub-Saharan Africa particularly. Most of these arboviruses share the same vector and the same symptoms with YFV. However, undiagnosed patients in the DRC's yellow fever surveillance system are never screened for other arboviruses. Our objective was to investigate other viral arthropod-borne diseases common in the tropics that can confound the clinical diagnosis in patients enrolled in yellow fever surveillance. In this study, we reported 16 cases of dengue and 2 cases of Chikungunya out of 453 samples collected between 2003 and 2011.
DENV was detected in a significant number of samples from this study. The presence of this virus might explain the clinical manifestations observed in these patients. Indeed, acute febrile jaundice is often reported in patients infected by DENV, especially in Southeast Asian countries where this virus is endemic (Syhavong et al. 2010). This syndrome has been associated with fulminant liver failure and thereby, it is an important indicator of severe dengue (Anand and Garg 2015, Samanta and Sharma 2015).
In the DRC, dengue infection is rarely diagnosed and not routinely tested, likely because no epidemic has ever been reported to draw attention to the infection, and because most laboratories do not have diagnostic resources for this disease. The only report of dengue in the DRC is related to the detection of anti-DENV antibodies in travelers returning home after a visit (Amarasinghe et al. 2011), and in one patient during the 1998 WNV epidemic that affected a military camp in Kisangani (Oriental) (Nur et al. 1999). Our results suggest that dengue is probably under-diagnosed in DRC, especially as Aedes mosquitos, the vector for DENV transmission, are present in DRC and have been associated with the transmission of CHIKV and YFV (two DENV related viruses) (Nur et al. 1999). Anti-DENV-2 antibodies were also found in forest buffalo sampled in 1994 in Garamba National Park, in Oriental (Kading et al. 2013). Due to the lack of symptom specificity, most dengue cases are likely mistaken for other several febrile illnesses of public health concern in the tropics such as malaria (Gould et al. 2008, Baba et al. 2013, Jaenisch et al. 2014, Moyen et al. 2014). This finding has been facilitated by increased awareness due to the occurrence of dengue outbreaks in neighboring countries and access to better diagnostic tools (Amarasinghe et al. 2011, Jaenisch et al. 2014).
There are five closely related, but antigenically distinct, dengue virus serotypes (DENV-1 to DENV-5) (Mustafa et al. 2015), which can produce a spectrum of clinical illness, ranging from a nonspecific viral syndrome to severe and fatal hemorrhagic disease or shock. Severe dengue is usually associated with circulation of different DENV serotypes, when infection by one DENV serotype is followed by subsequent infection by a different DENV serotype (Meltzer et al. 2012). In this study, we identified two serotypes of dengue virus (DENV-1 and DENV-2) and we reported that three patients from two different provinces were infected with both serotypes. This finding indicates that there is a risk of developing severe forms of dengue disease in Congolese people (Recker et al. 2009, Rodenhuis-Zybert et al. 2010, Chen and Vasilakis 2011). Therefore, there is an absolute need to organize dengue surveillance activities in the DRC.
During the yellow fever surveillance, samples came mostly from the two northern provinces (Equateur and Oriental) followed by the innermost parts of the DRC (Kasai occidental and Kasai oriental). This observation is corroborated by previous reports in the country. Indeed, sporadic cases of yellow fever and outbreaks are frequently reported in these provinces (Ministry of Public Health 2005, WHO 2010, 2013, 2014). Evident in our samples, an epidemic broke out in the city of Titule (Oriental) in late June 2010 leading to an increase in reporting of suspected cases of yellow fever between July and September (Fig. 2). Interestingly, we detected three dengue cases in samples collected in early July 2010 from Titule. This finding indicates that there was probably simultaneous circulation of YFV and DENV in this town during the outbreak period. Yellow fever transmission was detected and controlled by systematic surveillance. However, dengue transmission has been overlooked.
In the DRC, CHIKV was isolated for the first time in 1958, during the yellow fever outbreak of Doruma (Courtois et al. 1960). Since then, CHIKV has caused several outbreaks in the country. The most important epidemic occurred between 1999 and 2000 in the capital city of Kinshasa, when 44 cases were confirmed to have occurred after massive rainfalls (Filipe and Pinto 1973, Pastorino et al. 2004). In our study, we found two cases of Chikungunya detected in March 2011 in two different provinces. This result indicates that CHIKV is responsible for sporadic infections that are probably misdiagnosed in the DRC. In its classical form, the clinical symptoms are characterized by an acute febrile illness associated with myalgia and polyarthralgia, easily confused with other tropical febrile diseases (Nkoghe et al. 2012, Moyen et al. 2014). Jaundice has been reported in patients with CHIKV infection, but this clinical pattern is uncommon (Woodruff et al. 1978). Similar findings have been reported in Sudan where a sero-survey set up after yellow fever epidemic found CHIK cases among patients that would have been reported as suspected cases of YF (Farnon et al. 2010).
In this work, we focused on arboviruses causing yellow fever clinical picture. However, the differential diagnosis in this case can be very wide, including viral, bacterial, and parasitic diseases. We showed in a recent study that viral hepatitis A, B, C, and E are important causes of jaundice in suspected cases of yellow fever in the DRC (Makiala-Mandanda et al. 2017). Malaria, the main parasitic cause of jaundice syndrome, was excluded in the surveillance. In the same perspective, Salmonella typhi sepsis and hepatic leptospirosis, which is a public health problem in East Africa, should also be ruled out if blood culture was achievable.
However, this work allowed the detection of dengue and Chikungunya genetic material retrospectively on a serum bank initially intended for serological diagnosis. This result confirms that several arboviruses may contribute to the yellow fever clinical syndrome and laboratory diagnosis is the only way to differentiate them. Therefore, the surveillance concept should be reviewed and potentially converted into a laboratory-based syndrome surveillance, for greater efficiency, as proposed by Kasper et al. (2012). This surveillance strategy consists of identifying patients with clinical syndromes and then screening for an array of different causes in the laboratory. This strategy requires more technical resources and funding, but it can be helpful to increase the number of accurate diagnosis captured by the surveillance program.
In addition to identifying individual viruses, systematic screening for multiple viruses in these samples would also help to identify the incidence of concomitant infections, which may help to explain differences in disease symptoms and outcomes among patients (Chong et al. 2017). Our study specifically excluded those already identified as having YFV antibodies; given that arthropod-borne pathogens may co-infect patients due to heterogeneity in vector exposure or reduced immunity (Dellagi et al. 2016, Singer 2017), this caveat limits any conclusions concerning the (likely under-estimated) rates of co-infection that can be drawn.
In conclusion, this study showed that dengue and Chikungunya viruses are potential causes of acute febrile jaundice in the DRC. We reported two serotypes of DENV circulating in the country and emphasized the risk for occurrence of severe forms of dengue. Dengue and Chikungunya are likely under-recognized in DRC, because of limited diagnostic capacity and challenging differential diagnostic criteria. These findings highlight the need to consider dengue and Chikungunya diagnosis in the yellow fever surveillance and response program.
Footnotes
Acknowledgments
We thank the Ministry of Public Health of the DRC, particularly the head of the Direction de lutte contre la maladie for allowing us to work on samples from the yellow fever surveillance program. We are also grateful to the medical staff who participated in the yellow fever surveillance program in the DRC, without whom we could not have obtained the samples included in this study. We also acknowledge the Agence universitaire de la francophonie for contributing funds to this project. This study was supported by the Centre International de Recherches Medicales de Franceville (CIRMF), which is funded by the Gabonese Government, Total Gabon and The French Foreign Ministry in collaboration with the the Institut National de Recherche Biomédicale (INRB) of Kinshasa, DRC. Postdoctoral support for J.L.A. was provided by ANR JC “STORY” granted to Benjamin Roche.
Author Disclosure Statement
No competing financial interests exist.