
Abstract
Objectives:
This article describes the epidemiology of malaria in Yulin, 1999–2016. We review also malaria control strategy in Yulin in the posteradication phase.
Materials and Methods:
We examined all malaria case records from Yulin prefecture reported to the Ministry of Health since 1999 and extracted malaria data between 1999 and 2003, the stage of malaria eradication, from the notifiable disease reporting records and case records of Guangxi. Malaria data between 2004 and 2016, the stage of malaria elimination, was obtained from the National Notifiable Disease Reporting System and National Malaria Reporting System. We collected mosquitoes with light traps in the vector-breeding seasons and did the distinguished work with optical microscope.
Results:
Malaria average incidence decreased to 0.085/100,000, peaking of 0.263/100,000 in 2006, and no cases in years 2001, 2009, and 2010. Peak seasons are in November and June with proportions of 16.48% and 14.29%, respectively. Pathogenic parasites differed in the two stages; Plasmodium vivax was prevalent between 1999 and 2010, and Plasmodium falciparum between 2011 and 2015. Most malaria cases in the last 18 years occurred in males between 20 and 50 years of age. Of the 91 malaria cases acquired outside Yulin between 1999 and 2016, 31.87% were acquired in other provinces of China, and 68.13% were acquired in foreign countries. Sporozoite-positive vectors were zero between 1999 and 2016.
Conclusion:
In Yulin, between 1999 and 2016, autochthonous malaria cases decreased to zero. The personal preventative measures of surveillance–treatment–follow-up have been demonstrated to be effective in the Yulin malaria elimination campaign between 1999 and 2016. The major threat of malaria reintroduction to Yulin lies in imported malaria, especially by returning employees working in epidemic areas such as Africa and Southeast Asia. Data concerning employees who have worked abroad should be gathered to enable the construction of a mathematic model to forecast future trends of malaria in Yulin. The antimalaria campaign has to work closely with local authorities.
Introduction
M
Human-infecting Plasmodium relies on two hosts: humans and certain species of female Anopheles mosquitoes. The conventional diagnostic technique involves microscopy of blood smears; this plays an important role in malaria diagnosis because of its ability to diagnose and differentiate each species of malaria, and so it is used as the gold standard against which any new detection tool or technique is measured (Wongsrichanalai et al. 2007, Tangpukdee et al. 2009, Alam et al. 2011, Batwala et al. 2011, Ouattara et al. 2011).
There were 241,430 malaria cases in mainland China between 2004 and July, 2013, including 184,785 (76.54%) cases of P. vivax, 20,115 (8.33%) cases of P. falciparum and another 36,530 (15.13%) cases of undiagnosed (Feng and Xia 2014). There were 204,613 cases arising locally between 2004 and 2012 in China, and these peaked in 2007 with the constituent ratio of 87.88% (44,069/50,148). Imported malaria cases and the constituent ratio of P. falciparum cases have increased considerably since 2008. For example, there were 2953 imported cases between January and July in 2013, including75.41% (2.227/2953) of P. falciparum; meanwhile, during this period there were 34 local cases. This is lower than in 2004, when 6294 imported cases and 32,678 indigenous cases were reported (Feng and Xia 2014).
Guangxi Zhuang Autonomous Region, a coastal province in the south of China, was one of four administration areas with the most severe malaria situation. It has an area of 23.67 km2 and a population of 50.49 million. Its subtropical monsoon climate, with an average temperature of 21.1°C and annual rainfall of 1835 mm, supports the breeding of mosquitoes. An estimation of malaria cases between 1952 and 1956 (Guo et al. 2013) was reported as between 125,000 to 540,000 (an incidence of 677/100,000 to 2809/100,000). The incidence of cases has decreased sharply in the past six decades, and the malaria incidence in Guangxi had fallen to 0.10/100,000 in 2011. Between 2004 and July 2013 in Guangxi, there were 2143 cases (of which only 35 were transmitted locally), including 30.05% of P. vivax (644/2143) and 63.74% (1366/2143) of P. falciparum. There were no indigenous cases in 2008 in the province (Feng and Xia 2014).
As the ancient China's Maritime Silk Road Beginning, Yulin is a big city with highest capital migrant workers overseas. Most of the workers work in malaria-endemic areas, such as Africa and South Asia. Also as a former epidemic area of malaria, Yulin is threatened by this communicable disease. The average incidence of malaria was 247.86/100,000 between 1950 and 1980. With the universal treatment of antimalaria medicine and the action of immersing mosquito nets in anophelifuge, the incidence decreased sharply to 10.9/100,000 between 1981 and 1990. Since 1999, there has been no locally transmitted malaria case in Yulin. Yulin stands out as a model city for malaria control in Guangxi. Epidemic features and risks have changed under this new situation, which should be analyzed, so that new strategies and measures may be developed.
Materials and Methods
Data acquisition
We examined malaria data from 1999 and 2003 obtained from the notifiable disease reporting records and case records of Guangxi and extracted malaria data between 2004 and 2015 from the National Notifiable Disease Reporting System (NNDRS) and National Malaria Reporting System (NMRS).
Methods
Malaria diagnosis
We defined cases of malaria based on detection of malaria parasite in their blood by microscopy, or using biotechnology such as RT-PCR. All the 91 cases between 1999 and 2016 were identified based on morphology by microscopy, and all the 76 cases between 2005 and 2016 were diagnosed by RT-PCR.
Data retrieval and verification
All the malaria case records since 1999 were kept in the Department of Epidemiology, Yulin Center for Disease Control. Malaria data between 1999 and 2003 were compared with the original records kept in the Center for Disease Control and Prevention of Guangxi Zhuang Autonomous Region, and have been verified for integrity and facticity. Data from between 2004 and 2016 were verified through the NNDRS and NMRS; these information reporting systems were opened in 2004. Data of indigenous infection and imported cases were collected from NNDRS; other details were obtained from NMRS, including case number, plasmodium varieties, and the distribution of gender, age groups, and areas. Plasmodium carriers and suspect cases were excluded, as well as cases originating in Hongkong, Macao, Taiwan, and foreign cases.
Mosquito vector surveillance
Every year between 1999 and 2016, at least three mosquito breeding spots have been identified as part of the Anopheles survey location, through random samples. Between May and October, two light traps were set up in a bedroom and cowshed in each breeding spot and were functional for 12 h, overnight, which worked from 7 PM to 7 AM the next day, four times per week. Mosquitoes collected during the 12 h were anesthetized and distinguished by the morphology method using a microscope.
Data analysis
We analyzed data with SPSS 19.0 software, for chi-squared test and correlation test.
Results
Survey of malaria between 1999 and 2016
Between 1999 and 2016, there were 91 nonfatal malaria cases, all of which were imported and diagnosed by laboratory tests. The average incidence over the 18 years was 0.085/100,000; the peak value of 0.263/100,000 occurred in 2006; there were no cases of malaria in 2001, 2009, or 2010 (Fig. 1).
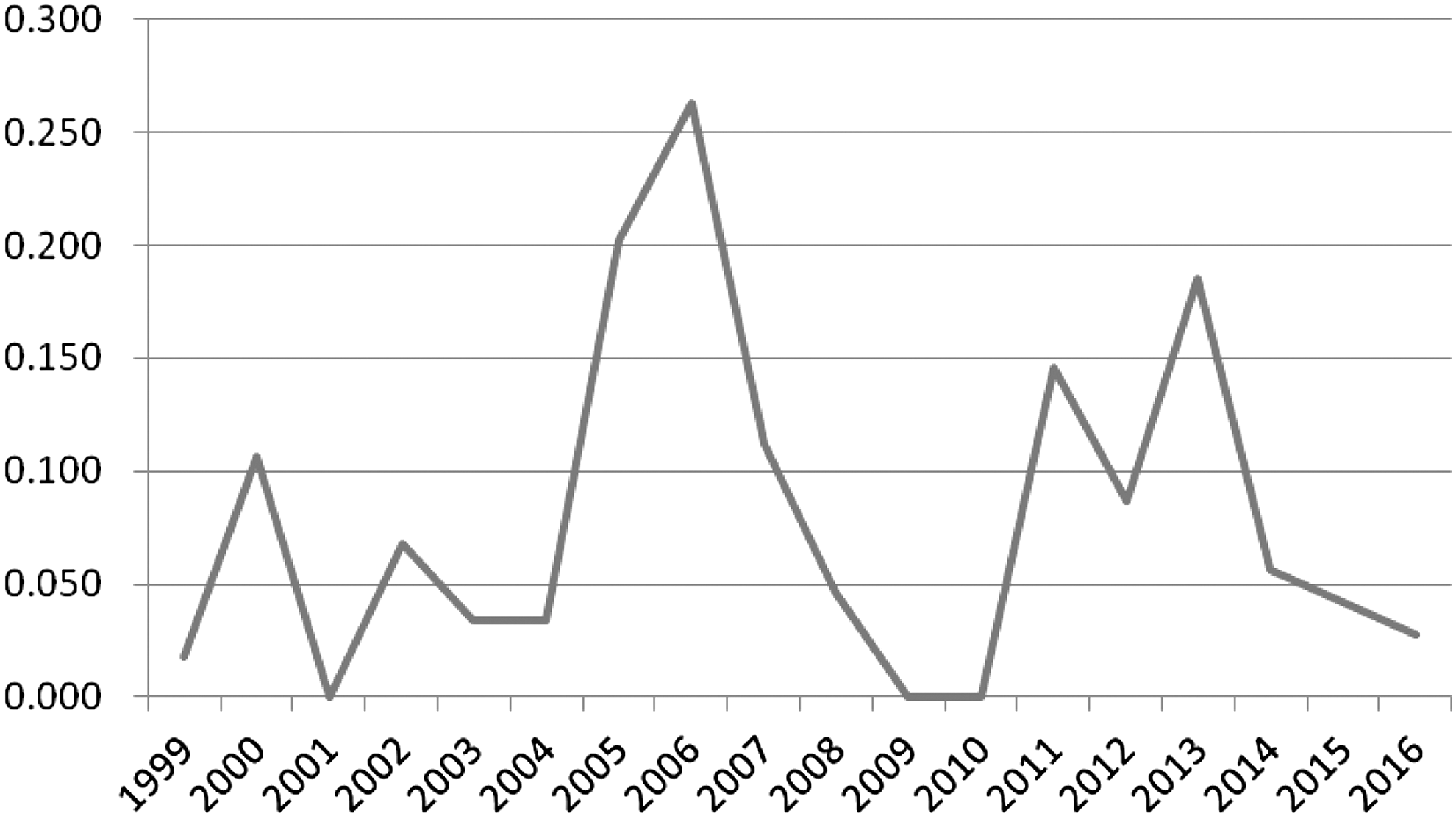
Incidence of malaria in Yulin between 1999 and 2016, by year.
Epidemic characteristics
Distribution by season
Malaria cases were reported throughout the whole year between 1999 and 2015, and most cases were reported in November and June with proportions of 16.48% (15/91) and 14.29% (13/91), respectively. The fewest cases were reported in March with a proportion of 3.30% (3/91).
Distribution by population
Malaria cases in different genders and age groups
Of the 91 malaria cases in Yulin between 1999 and 2016, 96.70% (88/91) were male. Eighty-six patients (94.51%) were between 20 and 60 years of age (Table 1).
Malaria cases in different occupational groups
In all the 91 malaria cases between 1999 and 2016 in Yulin, outdoor workers, such as miners, riflemen, construction workers, planters, and lumberjacks, had the highest risk of malaria infection, comprising 69.23% (63/91). Miners and riflemen constituted the highest proportion of 30.77% (28/91), followed by construction workers at 25.27% (23/91) (Table 1).
Malaria case origin
During the malaria elimination stage between 1999 and 2016, all the 91 malaria cases were imported, including 29 internally imported and 62 externally imported cases. There were 15 malaria cases between 1999 and 2004, comprising 12 internally imported cases from Hainan Province, Yunnan Province, Anhui Province, and Guangdong Province, and 3 foreign imported cases from Burma. During the malaria eradication stage between 2005 and 2016, 81.32% (74/91) of the cases were foreign imported and 18.68% (17/91) originated in other provinces that were known to be malaria-affected areas (Table 2).
Classification of pathogens
All 91 malaria cases in Yulin between 1999 and 2016 were diagnosed in a laboratory, using optical microscopy. Fifty-seven cases were caused by P. vivax; 32 cases, P. falciparum; 1 case, P. malariae; and 2 cases, P. ovale (including a mixed infection case of P. vivax and P. ovale in 2015). The pathogens were analyzed in two different stages; the proportions of P. vivax and P. falciparum were 94.34% (50/53) and 5.66% (3/53), respectively, in the malaria eradication stage between 1999 and 2010. Since 2011, in the malaria elimination stage, the ratios of P. vivax and P. falciparum were 17.95% (7/39) and 74.36% (29/39), P. malariae, P. ovale, and mixed infection cases were reported in the same stage.
Surveillance of vector mosquitoes, Anopheles
We observed vector mosquitoes in categories of geographic areas comprising urban, suburban, hilly regions, and plateau in Yulin, on 160 occasions between 2010 and 2016. All the mosquitoes captured were identified as Anopheles sinensis, Anopheles candidiasis, Anopheles dirus, Anopheles maculatus, or Anopheles tessellatus in Yulin. Anopheles minimus and Anopheles anthropophagus, known to be two of the major vectors for malaria ever, have not been detected since 2010 in Yulin (Table 3).
We collected 30% of the A. candidiasis, A. maculatus, and A. tessellatus, 1% of A. sinensis, and 10% of other varieties, with random sampling. The samples were digested and tested them with RT-PCR. We did not get any sporozoite-positive samples between 1999 and 2016.
Discussion
Epidemic characteristics in the two stages between 1999 and 2016
There were 91 malaria cases in Yulin between 1999 and 2016, all of which were diagnosed by optical microscopy and had been imported from outside Yulin. Case numbers peaked in 2005, 2006, and 2013; this was perhaps because of the increased numbers of international workers in those years, especially from malaria-endemic areas/countries. A typical situation occurred in 2013, called the Shangli Issue. A group of laborers who had been working in Ghana returned to Shangli County (a county of Guangxi Province) because of a local armed conflict in Ghana. Soon after, 1052 malaria cases were diagnosed and cured in Shangli, including 762 cases reported in June and July.
In Yulin, between 1999 and 2016, the peak months for malaria were June, September, and November. Most cases were reported in November, which is not the breeding season for mosquitoes. The peak months were probably related to the enhanced entry of international workers from epidemic countries and areas.
Malaria patients within the age group of 20 and 60 years accounted for 94.51% (86/91) of the cases; this is probably because men in this age group were most likely to work as international laborers in malaria-epidemic areas and countries. Approximately 75% of the malaria population was miners, riflemen, planters, and lumberjacks, which accords with this explanation.
The proportion of pathogen species differed between the two stages (1999–2010 and 2011–2016). In the malaria eradication prophase between 1999 and 2010, proportions of P. vivax and P. falciparum were 94.34% (50/53) and 5.66% (3/53), respectively; in the malaria elimination anaphase between 2011 and 2016, the ratios were 17.95% (7/39) and 74.36% (29/39), respectively. One case of P. malariae and two cases of P. ovale were reported in the malaria anaphase. The differing species of pathogen in the two stages may be related to the variety of countries and areas, with different prevalent parasites, in which the returning laborers had worked.
Xia et al. (2013) indicated that there were 2718 malaria cases in 2012 throughout China; the ratio of P. falciparum was 52.21%, whereas P. vivax was 39.74%. In the same year, there were 220 cases in Guangxi Province, of which P. falciparum caused 79.0%. During the malaria eradication stage, P. falciparum was the prevalent pathogen in Yulin City, Guangxi Province, or all through China. P. falciparum is the prevalent parasite in Africa, whereas P. vivax is prevalent in Southeast Asia (Coleman et al. 2006).
Influence of climate
Malaria is one of the communicable diseases that are influenced by climate; endemic and epidemic malaria present their own seasonal features (Coleman et al. 2006). The situation of malaria in Yulin was influenced far more by the imported cases, rather than by climate.
Influence of regional sources of malaria
Follow-up records indicated that international laborers always worked abroad as a team, returning to their hometown for various Chinese traditional festivals, such as the Double Ninth Festival, the Ghost Festival, and Tomb-Sweeping Day. They returned a month before the festivals to prepare something for the festivals and the malaria cases were detected. Patients who worked abroad returned with the prevalent pathogenic parasites of the source region and proportions of malaria species presented the pathogen structure.
The new strategy of surveillance–treatment: tracking was effective
Malaria incidence has been decreasing continually for decades. According to the World Malaria Report (World Health Organization 2015), between 2000 and 2015 its incidence decreased by 37%, and mortality by 60%. In Yulin, the incidence of malaria was 2456.27/100,000 in 1954, which was reduced to 1.09/100,000 in the 1980s. There were 91 imported, and no local, cases in the past 18 years during which period there were two stages; the malaria eradication prophase and the malaria elimination anaphase. Preventative strategies and measures need to adapt to changing malaria situations. Until the 1990s, accurate diagnosis and personal prevention was not appropriate for malaria control in Yulin because of its high incidence and mortality. In recent years, especially since the late 1990s, few indigenous malaria cases have arisen but several imported cases were reported. We have changed the old measure of extensive detection and treatment into a surveillance–treatment–tracking campaign, which has resulted in zero local cases and a block in local transmission. The new measure has worked.
Information regarding international labor should be published to analyze the relationship between malaria epidemic features and external labor flow
Yulin is a city from where many overseas workers originate. For over 100 years, many native Yulin men have worked abroad, most of them in Southeast Asia, which was one of the major malaria epidemic areas in the world. In recent years, increasing number of workers have gone to Africa and Southeast Asia for jobs, tourism, business, and for other reasons. The consequent increased international transient population has accompanied an increased trend of imported malaria cases. It would seem desirable to acquire the information regarding this population flow to analyze its relationship with malaria trends, to enable regression analyses that may forecast trends of malaria in Yulin.
Travel medical requirements for overseas workers, particularly those working in Africa and Southeast Asia, are pressing; meanwhile, the vaccine supply is ideal but impossible in the near future
Immunization is an effective method of disease prevention, including for infectious diseases and chronic noncommunicable diseases. Since there is no efficacious malaria vaccine which has been verified by extensive clinical trials, providing travel medical requirements is the one of the most effective methods, as well as using mosquito nets and spraying mosquitocides. The Health Section of Entry–Exit Inspection and Quarantine Bureau, Guangxi Zhuang Autonomous Region provides health education and yellow fever vaccine to workers traveling to Africa. Furthermore, employers have their own clinics to provide health education and treatment for malaria, but these provisions are nonstandard. Workers who contracted malaria overseas were always treated with antimalaria in a nonstandard way at any time. In summary, the etiology surveillance, tracking, and intervention for returning overseas workers are the key factors to keep a zero local malaria status.
Conclusion
Globally, around 3.2 billion people are estimated to be at risk of developing malaria, including 1.2 billion who are at high risk. According to the latest estimation, over 200 million cases of malaria occur worldwide annually, and the disease leads to over 500,000 deaths each year. Countries have kept fighting to achieve the goal of worldwide malaria elimination. On 5th September, Sri Lanka was certified by WHO as having eliminated malaria, which had long affected the island country. Since October 2012, Sri Lankan indigenous cases have been zero and, for the past three and a half years, no locally transmitted cases have been recorded. Throughout China, the program of malaria elimination 2011–2020 has been in place; this has included Yulin, a large city with over 7 million inhabitants in South China. As in Sri Lanka, an island country in Southeast Asia, there have not been any indigenous transmitted malaria cases in Yulin since September 1998. To maintain eradication and ensure the parasite is not reintroduced to the city, the antimalaria campaign is working closely with local authorities and partners to maintain surveillance and response capacity and to screen high-risk populations entering the city. The effectiveness of the measures taken (surveillance–treatment–follow-up) is consistent with the initial hypothesis, and no indigenous malaria cases have been detected for over 17 years. With the current situation, the measures of surveillance–treatment–follow-up will be continued.
Footnotes
Acknowledgments
The authors are grateful for the support provided for this work by the Excellent PhD Student Fund of the Guangxi Education Department, and Innovation Project of Guangxi Graduate Education (project no. YCBZ2015033).
Author Disclosure Statement
No conflicting financial interests exist.