
Abstract
Background:
Bites with tick-borne pathogens can cause various bacterial, viral, or parasitic diseases in humans. Tick-transmitted diseases are known as contributing factors to the increasing incidence and burden of diseases. The present article investigated the epidemiology of tick-borne diseases in South Korea.
Methods:
The incidence and distribution of common tick-borne diseases in Korea (Lyme disease, Q fever, and severe fever with thrombocytopenia syndrome [SFTS]) were investigated and analyzed, using data from the Korea Centers for Disease Control and Prevention (KCDC) infectious disease reporting system. A literature review was compiled on the current status of uncommon tick-borne diseases (Rickettsia, anaplasmosis, ehrlichiosis, bartonellosis, tularemia, tick-borne encephalitis, and babesiosis).
Results and Conclusions:
In South Korea, SFTS is an emerging disease, showing a rapid increase in reports since 2012, with high mortality. Likewise, reports of Lyme disease and Q fever cases have also been rapidly increasing during 2012–2017, although caution should be taken when interpreting these results, considering the likely influence of increased physician awareness and reporting of these diseases. Other tick-borne diseases reported in South Korea included spotted fever group rickettsiae, anaplasmosis, ehrlichiosis, tularemia, Bartonella, and babesiosis. Evidences on human infection with tick-borne encephalitis virus and Crimean–Congo hemorrhagic fever were recently unavailable, but both need constant monitoring.
Background
T
Methods
The authors analyzed the annual number of patients, mortality, and monthly distribution, including the regional distribution of Lyme disease, Q fever, and severe fever with thrombocytopenia syndrome (SFTS), using the Korea Centers for Disease Control and Prevention (KCDC) infectious disease reporting system (
Results and Discussion
Introduction and tick distribution in South Korea
Korea is located at the 124–132°E and 33–43°N and politically divided into North and South. In South Korea, 51 million people live in an area of 100,210 km2. South Korea consists of eight special/metropolitan cities and nine provinces. Figure 1A shows the geographical features and regional population of South Korea.
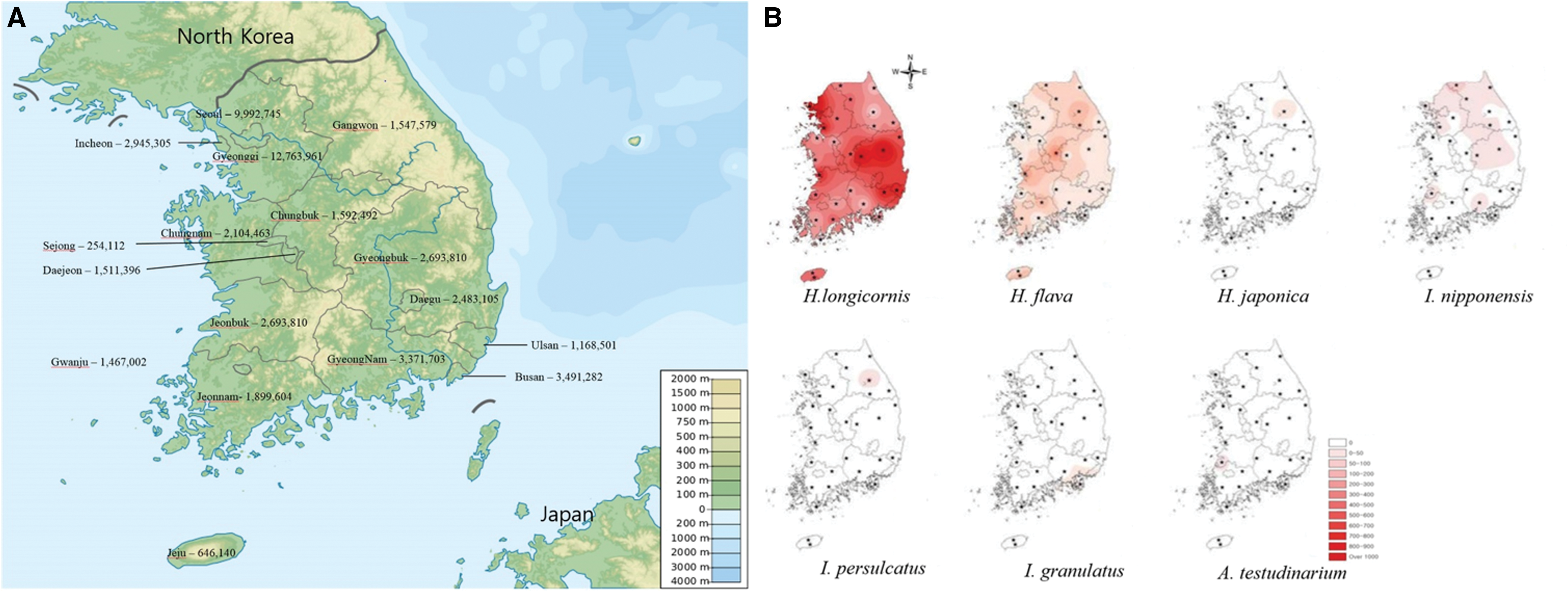
Overview of South Korea and tick distribution.
In the tick survey conducted by the KCDC in 2013–2015, a total of 29,992 ticks were collected in 29 sites nationwide (Song et al. 2017). Haemaphysalis longicornis was the most dominant species (88.9%), followed by Haemaphysalis flava (10.1%), Ixodes nipponensis (0.5%), Ixodes persulcatus (0.2%), Haemaphysalis japonica (0.2%), Amblyomma testudinarium (0.1%), and Ixodes granulatus (<0.1%). H. longicornis peaked in May to July (adult in July, nymph in May, and larva in September), and H. flava peaked in September to October (adult in September, nymph in October, and larva in September). H. longicornis and H. flava were distributed nationwide, while H. japonica and I. persulcatus were mainly found in Gangwon Province (east, mountain area). A. testudinarium was predominantly located in Jeonbuk Province (southwestern area of Korea) (Fig. 1B).
Tick-borne bacterial diseases in South Korea
Lyme disease
Lyme disease is a tick-borne bacterial disease caused by Borrelia spp., which occurs in all continents except Antarctica and South America. It is often characterized by nonspecific symptoms, such as fatigue, fever, headache, arthralgia, and lymphadenopathy. Erythema migrans lesions are commonly observed in 70–80% of patients (Mandell 2011).
Approximately 20 species belong to Borrelia burgdorferi sensu lato. The species differ according to the region and host characteristics, and clinical symptoms can vary by species. In Korea, Borrelia garinii and Borrelia afzelii were isolated from wild mouse and Ixodes (I. persulcatus, I. nipponensis, I. granulatus, and Ixodes ovatus) (Park et al. 1993, Kee et al. 1994). B. afzelii was also isolated from a patient in 2007 (Choi et al. 2007).
In Korea, Lyme disease was first reported in 1993 (Lee 1993). Since then, reports on Lyme disease have been increasing. According to the KCDC infectious disease reporting system, the number of patients (including suspected cases) in Korea has increased from 2 in 2012 to 54 in 2017. Increases in physicians' awareness of Lyme disease, as well as climate changes and popularity of outdoor activities, are considered as the major causes of the increased Lyme disease reports. Lyme disease is distributed all over South Korea and mainly occurs from May to November (Fig. 2). The mortality of Lyme diseases was 1.04% from 2011 to 2017.
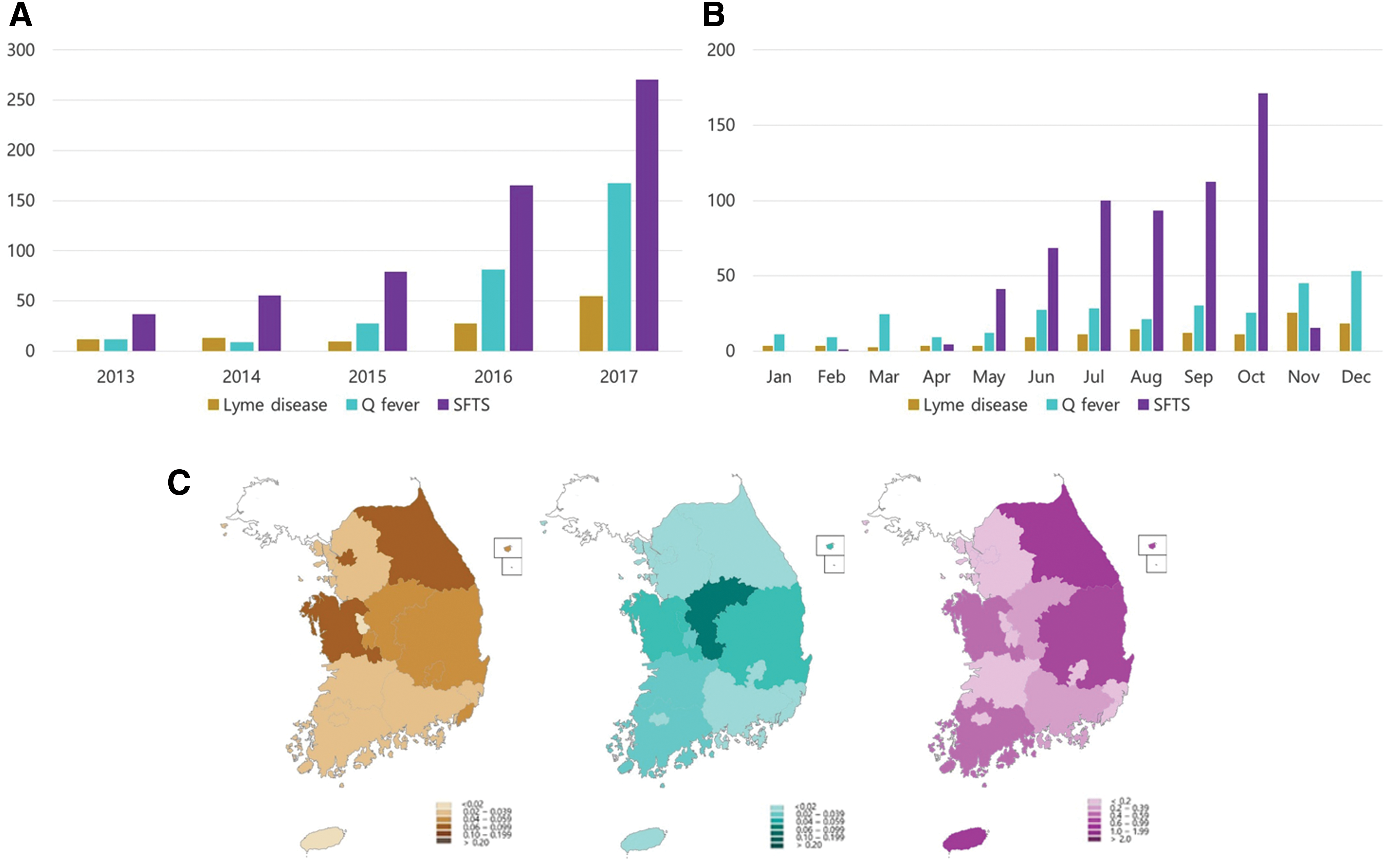
Reported cases of Lyme disease, Q fever, and SFTS in South Korea, 2013–2017.
Most of the reports on Lyme disease depend on serologic diagnosis, so a cross-reaction with Treponema, human immunodeficiency virus (HIV), leptospirosis, and rheumatic disease is possible (Magnarelli et al. 1987, Raoult et al. 1989, Shin et al. 1993). However, most febrile patients get serologic screening test for HIV and syphilis in Korea. Moreover, leptospirosis is also tested along with Lyme disease in patients suspected with acute fever during autumn. Furthermore, when positive or equivocal serology was found by KCDC, a secondary test is performed using Western blot. These tests can help diagnose Lyme disease more accurately.
Spotted fever group Rickettsioses
The spotted fever group (SFG) of diseases is caused by Rickettsia species associated with lice, fleas, mites, and ticks. Most of these diseases begin with nonspecific symptoms, such as fever, headache, myalgia, and nausea, at 2–14 days after a bite by the culpable vector. The appearance of a rash and other specific symptoms varies depending on the species. Mediterranean spotted fever (Rickettsia conorii infection) is characterized by a febrile rash with eschar. Japanese spotted fever (Rickettsia japonica infection) is associated with relatively small and shallow eschar formation, and Rocky Mountain spotted fever (Rickettsia rickettsii infection) is rarely associated with eschar formation and can have relatively high mortality. Siberian tick typhus (Rickettsia sibirica infection) causes a mild disease with lymphangitis expanding from the inoculation eschar to the draining lymph node (Parola et al. 2013).
SFG species are divided using the nucleotide homology of OmpA and OmpB. Although serological testing was not sufficient to distinguish species, it was suggested that SFG could exist in Korea. A serologic study of R. japonica (JFS) showed 19.88% seropositivity in 3401 acute febrile illness patients (Jang et al. 2004), and another noted 8% R. sibirica seropositivity and 14.34% R. coronii seropositivity in 3362 acute febrile illness patients (Jang et al. 2005). After the 2000s, advancements in molecular methods have led to the discovery of SFG species in S. Korea. In Korea, R. japonica was confirmed in H. longicornis by PCR (Lee et al. 2003, Noh et al. 2017), and R. rickettsii was also identified in H. longicornis (Kim et al. 2006). In 2006, the first SFG case, and the first identification of JFS (R. japonica), was in a patient in Incheon, South Korea (Chung et al. 2006). Moreover, Rickettsia monacensis, otherwise mainly reported in central Europe (Parola et al. 2013), was also isolated from a patient in South Korea (Kim et al. 2017). In a study that confirmed R. conorii infection in humans, partial nucleotide sequencing of rOmpB was conducted in a highly conserved gene region in Rickettsia spp. (Ma 2006). Thus, R. conorii could not be discriminated from other rickettsial species, such as R. sibirica. There have not yet been any reports of other species, such as Rickettsia africae and Rickettsia slovaca, in South Korea (Table 1).
HPS, hemophagocytic syndrome.
Ehrlichiosis and anaplasmosis
Ehrlichia and Anaplasma are members of the family Anaplasmataceae and infect human and animal blood cells. Ehrlichia and Anaplasma have similar genetic characteristics but differ in phenotype and host affinities. Based on 16S rDNA and groESL sequences, Ehrlichia, Anaplasma, Neorickettsia, Rickettsia, and Orientia evolved from a common origin (Ismail et al. 2010).
Ehrlichiosis was first described in the United States. Ehrlichia chaffeensis is mainly transmitted by ticks (Amblyomma americanum, Dermacentor variabilis, and Ixodes pacificus) and infects monocytic leukocytes, known as human monocytotropic ehrlichiosis. Ehrlichiosis can present with cardiovascular disease, aseptic meningitis, hemorrhagic fever, hepatic failure, and pneumonia (Mandell 2011).
In Korea, according to a study conducted in Gyeonggi Province (northern part of South Korea), 1.0% of 1618 ticks (H. longicornis, I. persulcatus, and I. nipponensis) were E. chaffeensis positive by PCR. Moreover, E. chaffeensis was isolated from H. longicornis collected from Gyeongbuk, Chungbuk, Jeonnam, and Jeju provinces (southern region of South Korea) (Kim et al. 2003, 2006, Chae et al. 2008, Yu et al. 2008, Lee et al. 2009a, Lee and Chae 2010, Kang et al. 2013b). It suggests that E. chaffeensis is distributed throughout South Korea. Serologic evidences were also found in acute febrile patients (Heo et al. 2002, Park et al. 2003). In 2000, there was a suspected case in a U.S. soldier dispatched to Dongducheon City, Gyeonggi (Sachar 2000). A febrile patient with cytopenia presented IgM antibody (titer, 1:256) of E. chaffeensis, while IgG antibody was not detected. No infectious etiological agent was identified, but the patient's seropositivity to E. chaffeensis and her absence from travel outside Korea could not exclude the presence of a newly identified reservoir of Ehrlichia in South Korea. In another study, Ehrlichia ewingii, Ehrlichia muris, and Ehrlichia canis were mainly isolated from H. longicornis, but also from I. persulcatus and I. nipponensis (Kang et al. 2013b) (Table 1). Although E. ewingii, E. muris, and E. canis have been known to cause human infection, definite reports were unavailable in Korea until recently.
Anaplasma phagocytophilum is endemic in the United States and some European countries. Its infection on granule-forming white blood cells is called human granulocytic anaplasmosis (formerly known as human granulocytic ehrlichiosis). Clinical symptoms of anaplasmosis are similar to ehrlichiosis, but with comparatively less skin rash and severity (Mandell 2011).
Serologic and molecular evidence of A. phagocytophilum in ticks and animals, from many parts of South Korea (Seoul, Gyeonggi, Gyeongbuk, Chungbuk, and Jeonnam), is abundant (Kim et al. 2003, Chae et al. 2008, Lim et al. 2010, Kang et al. 2011, 2013b, Bell et al. 2012, Lee et al. 2016a, 2016b, 2017, Yang et al. 2016) (Table 1). Serologic evidence from humans continues to be reported (Heo et al. 2002, Park et al. 2003), and in 2013 A. phagocytophilum was first isolated from a Korean patient in Chuncheon, Gangwon (Kim et al. 2014). In addition, in 70 Korean patients who underwent bone marrow examination (since 2006) due to fever and hemocytopenia, a retrospective examination revealed that 5 patients were PCR positive for A. phagocytophilum (Yi et al. 2017). It suggests that A. phagocytophilum has been relatively prevalent in Korea, even before 2006. Anaplasma platys has caused no human infections for some time, but recently some possible cases were noted, but were outside Korea (Maggi et al. 2013, Arraga-Alvarado et al. 2014). In Korea, the presence of A. platys is currently limited to ticks (H. longicornis, I. nipponensis, and H. flava) (Chae et al. 2008, Kang et al. 2013b) (Table 1). Anaplasma bovis has also been found in these three species, as well as I. persulcatus (Lee and Chae 2010, Doan et al. 2013, Kang et al. 2016), although A. bovis is not known to cause human infection.
Q fever
Q fever, a febrile illness caused by Coxiella burnetii, occurs worldwide. Acute Q fever progresses to chronic Q fever in 1–11% of patients, and the progress to chronic infection depends on host immunity. Acute Q fever is characterized by sudden high fever, headache, weakness, and atypical pneumonia, whereas chronic Q fever is manifested by endocarditis, hepatitis, and respiratory disease. The most common reservoirs are cattle, sheep, and goats. The bacteria can be found in urine, feces, milk, and birth products of mammals. Humans can be infected by consuming unpasteurized dairy products, inhalation of contaminated aerosols, and sexual contact and blood transfusion (Mandell 2011). In addition, infection through tick bites has been suggested. C. burnetii was detected in many kinds of tick species (mainly Ixodes, Rhipicephalus, Amblyomma, and Dermacentor), although its transmission is expected to be minimal (Duron et al. 2015).
Research on Q fever in Korean ticks is not active. Nonetheless, in a study of 105 Haemaphysalis ticks (89 H. longicornis, 8 H. flava, and 8 Haemaphysalis species), conducted in Cheongju City (Chungbuk Province) in 2004, 2 were PCR positive for Coxiella (Lee et al. 2004). In Korea, following the first case in 1993, the number of reported Q fever has continued to increase, particularly since 2014, mainly in Chungbuk Province (Fig. 2).
However, KCDC Q fever data should be carefully interpreted. Most Q fever diagnoses depend on serological evidence, which can be cross-reacted with Bartonella, Ehrlichia, and Rickettsia (Graham et al. 2000). We reported 23.7% of Bartonella seropositivity in Korean acute febrile patients (on submission), and the burden of ehrlichiosis and rickettsiosis is not well studied. In addition, in a study conducted by KCDC, only 23% of the reported 72 Q fever patients had high-risk occupations (e.g., slaughtermen and ranchers), from 2006 to 2011 (Kwak et al. 2013). Considering these factors, the epidemiology of Q fever should be studied further.
Tularemia
Tularemia is caused by the gram-negative coccobacillus, Francisella tularensis. Humans can be infected through arthropod bites (ticks and insects), contact with infected animals, or inhalation of contaminated aerosols. The main clinical symptoms are 3–5 days of latency followed by fever, chills, and fatigue. Depending on the infected site, tularemia presents six types of clinical illness as follows: ulceroglandular, glandular, oropharyngeal, oculoglandular, pneumonic, and typhoidal forms (Mandell 2011).
Tularemia is present in most countries of the Northern Hemisphere between the latitudes 30° and 70°N (Hopla 1974) and is especially endemic in Europe (Gurycova et al. 2001). In Korea, F. tularensis was detected in PCR assays performed in ticks in Jeonbuk, Jeonnam, Chungbuk, and Chungnam provinces (central and southwest of South Korea) (Takhampunya et al. 2017). And two human cases were reported in the southeastern region of South Korea (Gyeongbuk and Gyeongnam provinces) (Kim et al. 1998, Yeom et al. 2015) (Table 1). The incidence of tularemia can be underestimated, due to the variable and nonspecific symptoms. Consequently, continuous observation and caution are needed.
Bartonella spp. infection
Bartonellaceae are gram-negative bacteria, which have been isolated from humans and animals. There are more than 20 Bartonella species, and half of them have been confirmed as human pathogens. The clinical manifestations of Bartonella infection (bartonellosis) can vary based on species. Oroya fever and verruga peruana are caused by Bartonella bacilliformis, endocarditis and bacillary angiomatosis/peliosis by Bartonella quintana and Bartonella henselae, and cat-scratch disease by B. henselae and Bartonella clarridgeiae. The geographic distribution of Bartonella is influenced by the species and vectors. B. henselae and B. quintana are distributed worldwide, and B. bacilliformis is endemic in the Andes (Mandell 2011). Cats and dogs are known as reservoirs, and ticks are likely to transmit the disease to humans (Angelakis et al. 2010).
In Korea, serologic and molecular evidences for B. henselae and B. quintana were observed in tick and small animals (cats, dogs, and small rodents) (Chae et al. 2008, Kim et al. 2009b, Kang et al. 2013a, Yang et al. 2016). According to one study, Bartonella DNA was isolated from H. longicornis, H. flava, I. persulcatus, and I. nipponensis, and Bartonella elizabethae was identified in the spleen of striped field mouse (Kim et al. 2005). In other studies, the isolation of B. clarridgeiae from cats and dogs (Kim et al. 2009b) and Bartonella grahamii and Bartonella schoenbuchensis-related species from tick and Korean water deer have been evidenced (Kang et al. 2013a, Ko et al. 2013). In Korea, human infections of B. henselae and B. quintana were described (Lim et al. 2012, Im et al. 2013, Durey et al. 2016) (Table 1). The precise incidence of bartonellosis in Korea has not yet been investigated. However, among 300 healthy Korean individuals, a 15% seroprevalence of B. henselae was detected (Kwon et al. 2017), and in 31 patients with regional lymphadenopathies, 21 (67.7%) displayed positive titers of IgG to B. henselae and 64.5% to B. quintana (Chae et al. 2002), although both studies had the limitation on exclusively relying on a serosurvey. Nonetheless, these studies suggest that the burden of bartonellosis in Korea could be higher than expected.
Tick-borne viral diseases in South Korea
Severe fever with thrombocytopenia syndrome
Severe fever thrombocytopenia syndrome bunyavirus (SFTSV), a unique Phlebovirus of the family Bunyaviridae, is the etiological cause of SFTS, characterized by fever, digestive symptoms, thrombocytopenia, and multiple organ failure. SFTSV was first isolated in Northeastern China, and its incidence has increased in China, Japan, and Korea (Liu et al. 2014).
The major vector of SFTSV is H. longicornis and is distributed nationwide in South Korea. Rhipicephalus microplus, A. testudinarium, I. nipponensis, and H. flava are also known as vectors of SFTSV in South Korea (Yun et al. 2016).
In South Korea, SFTS mainly occurs in May–September, when tick activity is active, with infected patients reported until November. Gangwon (eastern, mountain area) and Jeju (a southeast isle) display a relatively high incidence (Fig. 2). The age of most patients (80%) is >50 years, and the proportion of agriculture and forestry workers is ∼70% of patients. The reported SFTS cases have been increasing annually, especially in 2017, reaching 172 cases. The mortality rate was >35% during 2012–2013, but decreased to 11.52% in 2016. During the introduction of infectious diseases, the mortality rate can be investigated by performing an examination only in severe patients, which decreases over time. Further observation is needed.
Tick-borne encephalitis in South Korea
Tick borne encephalitis virus (TBEV), of the family Flaviviridae, causes tick-borne encephalitis, characterized by biphasic fever and encephalitis. TBEV is distributed from central Europe to Far East Asia. Phylogenetic analysis revealed three subtypes as follows: western, Siberian, and far eastern (formerly known as the Russian spring-summer encephalitis virus) (Mandell 2011).
TBEV is mainly mediated by Ixodes ricinus in Europe and I. persulcatus in Siberia/Far East Asia. In a phylogenetic analysis performed in South Korea, the western TBEV subtype was isolated from H. longicornis, H. flava, and I. nipponensis in Gyeonggi, Gangwon, Jeonbuk, Gyeongnam, and Jeju provinces (Kim et al. 2009a, Ko et al. 2010, Yun et al. 2012) (Table 1). As yet, records of TBEV patients were unavailable in South Korea. However, it is expected that human infections in Korea will be reported soon, considering that patients have been consistently informed in China/Japan and TBEV is also detected in Korean tick surveillance (Yoshii et al. 2017). Other related flaviviruses in the TBEV serocomplex (Powassan virus, louping ill virus, Alkhurma virus, Kyasanur Forest disease virus, and Omsk hemorrhagic fever virus) have not yet been found in South Korea.
Tick-borne parasitic diseases in South Korea
Babesiosis
The genus Babesia (phylum Apicomplexa) causes babesiosis. Babesia was first discovered in animals by Babes in 1988, and >100 species have been identified. Babesia is mainly mediated by Ixodes ticks. Symptoms of babesiosis vary according to the species and immunity of the patient. Babesia microti is common in the Americas and is known to show mild symptoms, such as nonspecific fever, myalgia, nausea, headache, and weakness. Conversely, Babesia divergence, the most common strain associated with humans in Europe, can present severe illness (pulmonary edema, shock, and renal failure) (Mandell 2011).
In Korea, there was a first report on Babesia sp. from cattle. Another report mentioned that Boophilus microplus and H. longicornis could be considered as a predominant vector for transmission of Babesia in Korea (Han et al. 1966). There were some additional reports by morphological evidence (Lee and Choi 1976, Suh 1987), and molecular evidence of B. microti and Babesia ovata from mammals (cattle, raccoon, deer, and badger) was reported since 2000s (Cho et al. 2002, Han et al. 2010, Hong et al. 2017). In 2008, Babesia was first isolated from Korean patients, without overseas travel, in Gurae (Jeonnam province), similar to Babesia spp. detected from sheep in China (Kim et al. 2007). Babesia gibsoni and Babesia caballi were found in mammals and ticks in Korea, although these species are not known to cause human infection (Jia et al. 2009, Lee et al. 2009b, Kang et al. 2013b) (Table 1).
Conclusions
Various tick-borne diseases occur in South Korea, depending on the region and season. Lyme disease and Q fever have been increasingly reported in South Korea. However, most diagnoses of these diseases depend on serological tests and require careful interpretation. SFTS is also reported to be increasing rapidly, and the increased number of examination by increased perception of physicians can be considered as the main cause of increased SFTS reports.
Spotted fever, anaplasmosis, ehrlichiosis, tularemia, bartonellosis, and babesiosis have also been observed. Although no TBEV and Crimean–Congo hemorrhagic fever human infections have yet been documented in South Korea, their possible emergence should be cautiously monitored. Further research and surveillance are required.
Footnotes
Acknowledgment
This work was supported by a research grant from Inha University Hospital.
Author Disclosure Statement
No conflicting financial interests exist.