
Abstract
Anaplasma phagocytophilum—the causative agent of human granulocytic anaplasmosis (HGA)—is a tick-borne pathogen transmitted by Ixodid ticks infecting wild and domestic mammals as well as humans. Despite the availability of evidence regarding this emerging infection among vectors, host animals, and individuals in China, there is limited knowledge on the prevalence and distribution of A. phagocytophilum in the Yunnan Province. The aim of this study was to assess the seroprevalence of A. phagocytophilum in healthy adults and patients with acute undifferentiated fever from four regions in the Yunnan Province. The enzyme-linked immunosorbent assay and indirect immunofluorescence assay were used to detect immunoglobulin (Ig) G and IgM antibodies against A. phagocytophilum in sera obtained from 1185 healthy blood donors and 245 patients with acute undifferentiated fever, respectively. Demographic variables were assessed as potential risk factors using the chi-squared test. The rates of seropositivity rates were 7.59% and 4.49% in healthy donors and fever patients, respectively. Analysis of risk factors such as gender, age groups, and place of residence showed statistically significant differences. Infections with A. phagocytophilum occur widely among individuals residing in southwestern China. Our results indicate that there is serological evidence of HGA in this population and presence of acute A. phagocytophilum infections in patients with undifferentiated fever in the Yunnan Province.
Introduction
The tick is a common and dangerous insect carrying and transmitting viruses, bacteria, rickettsia, spirochetes, and protozoa (Choi et al. 2016). Tick-borne diseases are zoonoses, with pathogens maintained in natural cycles involving tick vectors and vertebrate hosts. Humans are occasional hosts of ticks without a role in maintaining tick-borne agents in nature (Socolovschi et al. 2009). In the previous three decades, tick-borne pathogens have emerged worldwide and become a great threat to human health (Dantas-Torres et al. 2012, Kilpatrick et al. 2012).
Anaplasma phagocytophilum is an obligate intracellular bacterium transmitted by hard ticks belonging to the Ixodes persulcatus complex (Woldehiwet 2010, Dugat et al. 2015) and causes human granulocytic anaplasmosis (HGA) (Parola and Raoult 2001) associated with severe febrile reaction and hematological disorders (Stuen et al. 2013). HGA was first reported in the United States in 1990 (Dumler et al. 2007) and has been identified in tropical, subtropical, and some temperate regions of the world (Jin et al. 2012, Kim et al. 2014, Yoshikawa et al. 2014). In China, the first case of HGA was identified in the Anhui Province in 2006. A total of 46 confirmed cases were diagnosed between 2009 and 2010, with a fatality rate of 8.1% (Zhang and Lv 2013). However, several seroprevalence studies suggested that the number of reported cases in China may be underestimated (Zhang et al. 2012a, 2014).
The Yunnan Province is located in the southwestern border of China and has a long borderline shared with Laos, Myanmar, and Vietnam. Due to its diverse topography and climate, the Yunnan Province is extremely rich in flora and fauna. Therefore, Pathogens and insects are widely distributed in this region, rendering the Yunnan Province a high-incidence area for insect-borne infectious diseases. The abundance and diversity of ticks contribute to the prevalence of tick-borne diseases in this region, severely affecting human health. Ixodidae—the A. phagocytophilum-related tick species—is present in most areas of the Yunnan Province (Guo 2015). In addition, several species of ticks have been shown to carry A. phagocytophilum in this region, while numerous kinds of domestic animals (e.g., dogs, goats, cattle, horses, and rodents) have been proposed to be reservoir hosts for A. phagocytophilum (Wang et al. 2012, Zhang et al. 2012a, 2015, Yang et al. 2016). Moreover, studies have found that the media ticks carry A. phagocytophilum in the countries sharing borders with the Yunnan Province (Parola et al. 2003, Taylor et al. 2016).
Serological evidence for human A. phagocytophilum infection in the Yunnan Province has been previously demonstrated (Zhang et al. 2014, Cui et al. 2015). A seroepidemiological study investigating nine provinces of China reported a seroprevalence of 0.6% against A. phagocytophilum among human in the Yunnan Province (Zhang et al. 2014). However, a study by Chang et al. (2010) involving farm residents (n = 237) in three sites in the Yunnan Province with different geographical characteristics failed to find any positive samples. Another investigation involving first-year students in Yunnan University discovered that the seroprevalence of antibodies against A. phagocytophilum was 12.5% (Cui et al. 2015).
Despite the availability of evidence regarding this emerging infection among vectors, host animals, and individuals in China, there is limited knowledge on the prevalence and distribution of A. phagocytophilum in the Yunnan Province. Furthermore, there is a lack of data regarding patients suspected of A. phagocytophilum infection, such as patients with acute undifferentiated fever. The present, cross-sectional serological investigation was performed to determine the seroprevalence of A. phagocytophilum infection in healthy adults and patients with acute undifferentiated fever from different geographical areas of the Yunnan Province.
Materials and Methods
Study design, site, entry criteria, and sample collection
This study was conducted in the hospitals of the four counties of the Yunnan Province, namely the Hospital of Yanshan County, Hospital of Binchuan County, Hospital of Hekou County, and Hospital of Zhaotong city (Fig. 1). According to the Hospital grading standard of China, all these institutions are of ≥2 grade and serve local residents. From April to September of 2017, during the tick active season, blood samples were collected from local healthy individuals and patients with undifferentiated fever from the four aforementioned regions. The three primary criteria for inclusion of fever patients were as follows: (1) age ≥12 years; (2) presence of documented acute fever ≥37.5°C by an axillary temperature measurement; and (3) absence of definitive diagnoses of malaria, dengue fever, or typhoid febrile diseases. Blood samples were collected in serum separator tubes and centrifuged. The sera were frozen in aliquots at −70°C until use.

Locations of sampling sites. Yunnan Province located in southwest of China is shown in yellow as seen on inset upper left. The red crosses represent four sampling sites in this study. All samples were analyzed in Kunming, capital of Yunnan Province, as shown by blue dot. Color images are available online.
Laboratory testing
The sera obtained from healthy individuals were tested using a commercially available immunoglobulin (Ig) G enzyme-linked immunosorbent assay (ELISA) kit (BYS13614-5B; Bioye, Shanghai, China) and an indirect immunofluorescent assay (IFA) kit (EEG-120; Fuller Laboratories, Fullerton, CA) for A. phagocytophilum, measuring the levels of IgG antibodies against the A. phagocytophilum antigen. Sera obtained from patients with fever were tested using the same kits for the detection of IgM antibodies against A. phagocytophilum. During testing, positive and negative control wells were included in each slide. Samples were initially screened at low dilutions. Following the confirmation of sample positivity, the screening involved titration to endpoint (titer). According to the instructions provided by the manufacturer, antibody titers ≥1:80 for IgG and/or ≥1:64 for IgM against A. phagocytophilum antigens denoted positivity.
Statistical analysis
Statistical analysis was performed using the SPSS Statistics version 20 (SPSS, Inc., Chicago, IL). The chi-squared test was used to explore the associations between seropositivity and study variables. A p values of ≤0.05 denoted statistical significance. Comparisons of ranked data were performed using the rank-sum test.
Results
A total of 1430 participants were enrolled. All selected candidates provided consent before their participation in the study. Of those, 700 (49%) and 730 (51%) participants were males and females, respectively. The mean age of participants was 39.5 years (range: 12–85 years) and the majority belonged to the 21–40 year age group (Table 1).
Distribution of Participants According to Gender and District
Among all participants, IgG against A. phagocytophilum was detected in 90 (7.59%) healthy adults and 11 (4.49%) fever patients. Using the chi-squared test, many of the demographic and regional variables showed significant baseline correlation with seropositivity (Table 2).
Baseline Correlation of Seropositivity with Different Variables
Chi-squared test was used to explore the association between A. phagocytophilum seropositivity and gender, district, and age.
p < 0.005.
IgG, immunoglobulin G; IgM, immunoglobulin M.
The prevalence of seropositivity to A. phagocytophilum appeared to increase with age. Among healthy donors, the 41–50 year age group showed the highest seroprevalence (i.e., presence of the IgG antibody). Of note, the differences between this age group and the 12–20 and 21–31 year age groups were statistically significant (p < 0.05). The rates of seropositivity were significantly different between males and females in both the healthy individual group and fever patient group. The Hekou district was linked to a significantly higher risk of exposure to A. phagocytophilum compared with other districts. Using the chi-squared test to compare differences between the two groups in the four districts, significant differences were both found in healthy individuals from Hekou district (p < 0.05) (Fig. 2).
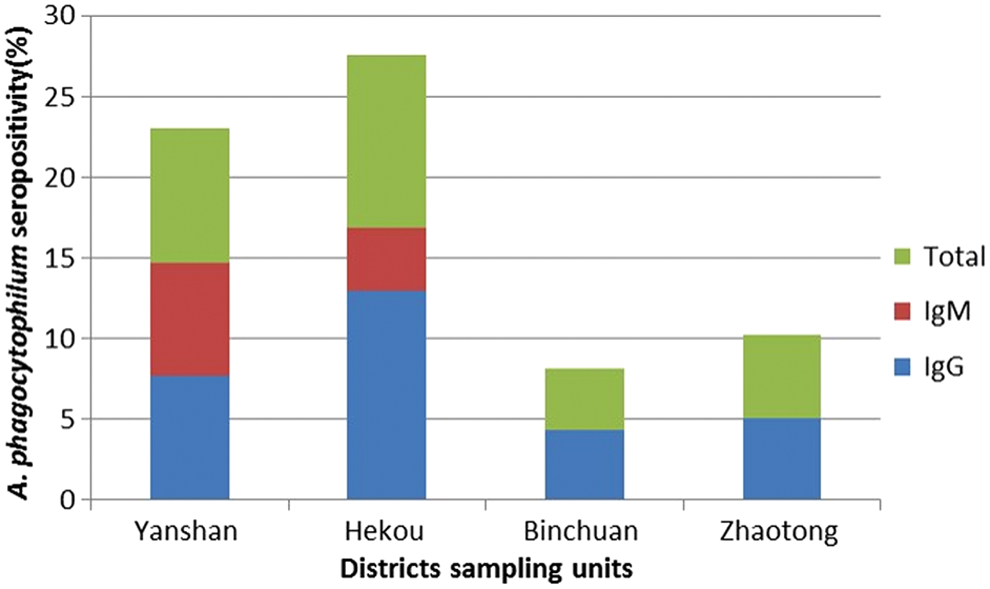
Prevalence of Anaplasma phagocytophilum seropositivity in different districts of the Yunnan Province. This histogram was produced using data from the seropositive individuals shown in Table 2 and Microsoft Excel. IgG, immunoglobulin G; IgM, immunoglobulin M. Color images are available online.
Discussion
This was the first multiregional seroprevalence study regarding the tick-transmitted agent A. phagocytophilum in the four counties of the Yunnan Province. The findings of this study may be used as baseline data for subsequent studies in this region.
The seroprevalence of A. phagocytophilum observed among patients with fever in this study was similar to that reported among patients with undifferentiated fever in northern and northwestern Thailand (5.3% and 3.7%, respectively) (Blacksell et al. 2015). This similarity is noteworthy, considering the proximity of these areas to the Yunnan Province. Therefore, the management of these infections may benefit from coordinated cross-border prevention and control activities between the neighboring countries. Compared with epidemiological data obtained in China, the seropositive rate for A. phagocytophilum in healthy donors from the Yunnan province (7.59%) was lower than those reported in Tianjin (8.8%) (Zhang et al. 2008b), Beijing (14.1%) (Zhang et al. 2012b), Henan (26.23%) (Zhang et al. 2013), and Shandong (26.7%) (Zhang et al. 2011). This finding indicates that the factors associated with the occurrence of A. phagocytophilum infection may differ across regions. Another explanation may be that examined populations differed considerably.
Analysis of the age distribution among participants showed that the prevalence of A. phagocytophilum seropositivity increased with age. Age >30 years was associated with a three-fold increased risk of A. phagocytophilum infection versus the younger age groups. Despite differences in seroprevalence, this result is consistent with that reported in a study performed by Zhang et al. (2014) investigating nine provinces in China. Of note, this trend was also observed in similar studies from Africa and Europe (Chochlakis et al. 2008, Elhamiani Khatat et al. 2016). The following reasons are suggested: (1) higher lifetime risk of exposure to pathogens; (2) the median age of adults where occupational exposure is higher, and there is a higher risk of coming into contact with host animals (e.g., goats, cattle, and dogs); and (3) higher incidence to medical attention in the middle-aged adult group. This mirrors the situation in endemic areas in which an increasing number of individuals may be exposed to the infection as they advance through life. This leads to an accumulation of middle-aged and elderly seropositive individuals in the community.
The sex distribution varied between the total population and the different areas investigated. Males were shown to be at a higher risk of infection with A. phagocytophilum than females. In addition, the difference in seroprevalence between the two sexes was statistically significant. Furthermore, other studies have demonstrated that the rate of seropositivity was significantly higher in males (Chochlakis et al. 2009, Zhang et al. 2014, Zukiewicz-Sobczak et al. 2014). This observation may be attributed to the higher involvement of males in outside activities, and labor, increasing the risk of contact with infected tick vectors and host animals.
Accumulating evidence indicates that differences in the climate and other environmental conditions determine the distribution of tick-borne pathogens (Wimberly et al. 2008). Moreover, we found a statistically significant difference in the rates of IgG acquisition between the four different districts (p < 0.01). The observed difference in the regional distribution of seroprevalence indicates that individuals in the southern and southeast Yunnan Province are more likely to have an IgG antibody against A. phagocytophilum than those in northern and western Yunnan Province. This may be attributed to the location of the southern areas of the Yunnan Province (i.e., tropical zone with high temperatures and humidity, and abundant rainfall, facilitating the breeding and survival of ticks in host animals). Thus, these populations have an increased risk of coming into contact with the pathogen, consequently leading to a higher infection rate.
HGA—a tick-transmitted rickettsial infection caused by A. phagocytophilum—is a common cause of undifferentiated fever in China (Zhang et al. 2013). Patients are often initially diagnosed with a mild viral infection, and thus may not be treated effectively and promptly (Bakken and Dumler 2015). Furthermore, as many as 3% of infected individuals may develop life-threatening complications and ∼1% expire due to the infection (Dahlgren et al. 2011). In addition to transmission through the ticks, the A. phagocytophilum infection may occur through close contact with the blood and secretions of patients with HGA (Zhang et al. 2008a). Understanding these processes may be helpful for medical workers involved in the screening and treatment of individuals in this region. In this investigation, a few cases of unexplained fever with IgM antibody against A. phagocytophilum were found. This result shows that there are patients with acute stage of HGA in the Yunnan province, but they were not diagnosed correctly in time due to insufficient understanding. Future studies will focus on the clinical observation and analysis of the infectious pathogen in these patient populations.
Our study was characterized by limitations. First, a single frequently used cutoff value was chosen (i.e., ≥1:80 for IgG and ≥1:64 for IgM) for the diagnosis A. phagocytophilum infection through the IFA kit. Second, the information regarding the participants and classification of samples was limited. Third, there is controversy regarding the presence of dual/multiple infections in an endemic setting or cross-reacting antibodies. In this study, antibodies in the sera of participants were detected using only one antigen (i.e., A. phagocytophilum). Finally, the unavailability of adequate data regarding local climatic conditions, as well as environmental and geospatial information at the primary sampling unit level did not permit the assessment of interdistrict differences in exposure to the infection.
Conclusions
This study found that infection with A. phagocytophilum is widely present among individuals residing in the Yunnan Province. Moreover, the sex, age, and regional distribution of seroprevalence were different from those of other areas in China. These differences may be related to the lifestyle, work, and behavior of local residents, as well as the condition of the infection, and distribution of ticks and host animals. Therefore, analyzing the risk factors and understanding the distribution of A. phagocytophilum infection are of crucial importance to control its occurrence and transmission. Considering the high risk of A. phagocytophilum infection in the Yunnan Province, appropriate measures should be taken to inform the local population and train the local medical personnel in the diagnosis and treatment of A. phagocytophilum infection.
Footnotes
Acknowledgments
The authors wish to acknowledge and thank all of the donors, technicians, and administrative personnel of the Yanshan County People's Hospital, Hekou County People's Hospital, Binchuan County People's Hospital, and Zhaotong City People's Hospital, who participated in this study.
This study was supported by grants from the National Natural Science Foundation of China (no. 31560051, 81560596 and 81860644), the Yunnan Applied Basic Research Projects (no. 2017FE467-001 and 2017FE467-124), and the Science Research Fund Project of Yunnan Provincial Department of Education (no. 20150041Y).
Author Disclosure Statement
No conflicting financial interests exist.