
Abstract
Orientia tsutsugamushi is an obligate intracellular bacterium that causes scrub typhus in humans. Formerly thought to be confined to the “tsutsugamushi triangle” within the Asia–Pacific region, scrub typhus was recently identified in the Western Hemisphere. Moreover, a new species of Orientia bacterial genus was isolated from a patient in Dubai. This study investigated Orientia exposure in an African country, the Democratic Republic of Sao Tome and Principe. Two sets of samples were analyzed in the study: 240 dried blood spots (DBSs) collected in 2016 and 863 serum samples from 570 pregnant women in 2003. Antibodies against O. tsutsugamushi were examined by immunofluorescence assay (IFA) and enzyme-linked immunosorbent assay (ELISA). The positive samples were further confirmed by Western blot. The results of IFA showed that 5.8% (14/240) of DBSs and 20.4% (116/570) of the serum samples contained reactive antibodies, whereas IgG ELISA yielded a positive rate of 15.4% (88/570) for the serum samples. These findings provided serologic evidence of potential Orientia exposure even though case of scrub typhus has never been diagnosed in the nation. Further studies are needed to determine the epidemiology and the burden of this neglected tropical disease in Africa.
Introduction
Orientia tsutsugamushi is an obligate intracellular Gram-negative bacterium that causes scrub typhus in humans. The natural vector is trombiculid mite (genus Leptotrombidium) that also serves as the reservoir to maintain the microorganisms through trans-stadial and transovarial transmission (Paris et al. 2013). Humans contract scrub typhus by being bitten by infected chiggers, the only parasitic stage of the mite's lifecycle. An eschar containing high bacterial load was reported appearing at the site of chigger feeding in 7% to 80% of patients (Rajapakse et al. 2017). Otherwise, scrub typhus typically manifests as a nonspecific febrile illness, with symptoms similar to other rickettsioses, including rash, headache, muscle pain, cough, and gastrointestinal symptoms (Tilak and Kunte 2019). The severity of clinical outcome varies depending on the strains of infection, the hosts' immune status, drug susceptibility, accessibility to health care systems, etc. Without appropriate antimicrobial treatment, scrub typhus could be life threatening with a mortality rate of 6% (median, range 0–70%) (Taylor et al. 2015). Treated scrub typhus was associated with a median mortality rate of 1.4% (range 0–33.3%) (Bonell et al. 2017). It is estimated that over a billion people are at risk globally and 1 million cases occur each year (Kelly et al. 2009).
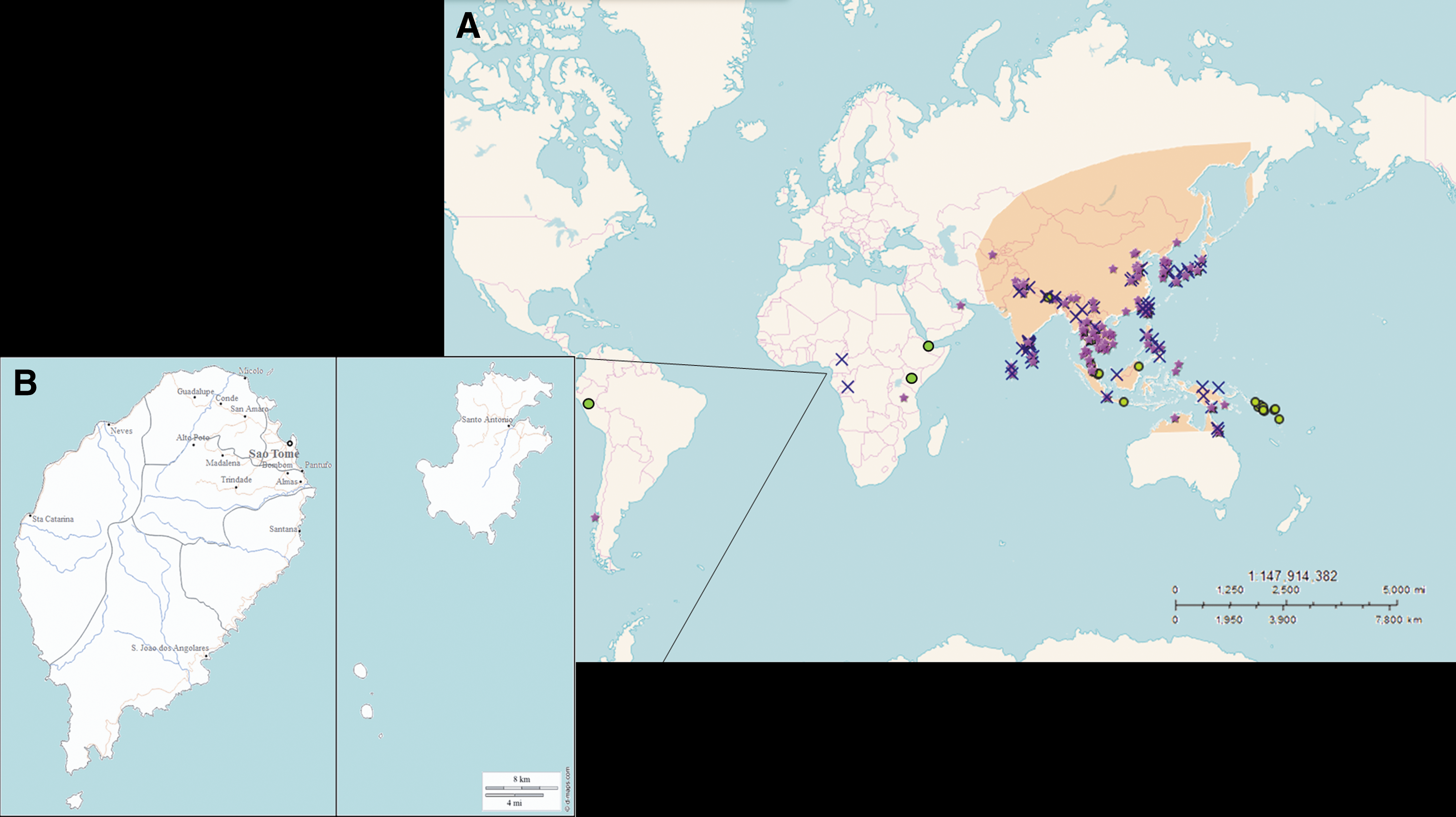
Scrub typhus is endemic in regions of Asia and the Pacific islands known as the “tsutsugamushi triangle.” It is an area extending from Pakistan in the west to Japan in the east, far eastern Russia in the north, and Australia in the south, covering >8 million square kilometers (Xu et al. 2017). Until 2006, scrub typhus was thought to be restricted to Asia and caused by only Orientia species, O. tsutsugamushi. However, these concepts were challenged as infections were reported in Chile and Peru, and a new species of Orientia, O. chuto, was isolated from Dubai (Izzard et al. 2010, Balcells et al. 2011, Weitzel et al. 2016, Kocher et al. 2017). Yet in Africa, the concern about malaria overshadowed other febrile illnesses in most countries. Although several reports published in 50–70s have proposed Orientia exposure in Ruanda, Congo, and Nigeria (Giroud 1951, Giroud and Jadin 1951, Emejuaiwe and Njoku-Obi 1978), the suspicion of the presence of the pathogen was raised only by case reports of international travelers in the later three decades before recent studies in Kenya and Djibouti gave a clue to the likely wider distribution of scrub typhus (Osuga et al. 1992, Ghorbani et al. 1997, Thiga et al. 2015, Horton et al. 2016, Maina et al. 2016). This study, as part of an investigation to determine the risk of exposure to vector-borne and zoonotic pathogens other than Plasmodium circulating in the region (Yen et al. 2016), detected Orientia-reacting antibodies in samples from healthy donors in the Democratic Republic of Sao Tome and Principe (DRSTP), an island nation in the Gulf of Guinea (Fig. 1). Our goal is to raise public awareness as well as to provide more information about the global burden of this neglected tropical disease.
Materials and Methods
Ethics statement
This study was approved by the Research Ethics Committee of National Taiwan University Hospital (Reference No. 201110023RD) and the Ministry of Health of the DRSTP (Official No. 29/P0CNE/2013 and 19/P0CNE/2016).
Dried blood spots collection, 2016
Human subjects were recruited during the proactive mass screening of malaria conducted from January to March in 2016. Dried blood spot (DBS) samples were collected by finger prick and preserved on Whatman 903 filter paper (Whatman plc, Springfield Mill, United Kingdom). The filter paper was then air dried, sealed in zipper storage bags, and transported to the laboratory in Taiwan. A total of 240 samples were randomly selected from 8 age groups for further analyses (Table 1). To elute the samples, 6-mm disks were cut by a cardpunch and immersed into 250 μL sterile phosphate buffered saline (PBS) overnight. DBSs have been used as alternative specimens for plasma to assess antibodies against Orientia spp. (Phetsouvanh et al. 2009, Vallée et al. 2010). The eluted sample is equivalent to a 1/25 dilution of original serum.
Detection of Orientia Antibodies in Dried Blood Spots by Immunofluorescence Assay
Archive serum samples, 2003
Banked serum samples collected from pregnant women who attended local clinics for regular prenatal examinations from 2003 through 2004 were also tested for antibodies against O. tsutsugamushi retrospectively. Identifiable information of these serum samples was removed except for age, gestational age, gravida, and the sampling site. Eight hundred and sixty-three samples from 570 donors were collected in this study. These women were 15–47 years of age (mean 26 years). All of them were negative for HIV and malaria.
Immunofluorescence assay
Antibodies against O. tsutsugamushi were screened by indirect immunofluorescence assay (IFA) as described with slight modifications (Demma et al. 2006). Whole-cell antigens of the Karp strain of O. tsutsugamushi were coated on slides, fixed, and permeabilized with ice-cold acetone, and stored at −70°C until use. The samples were initially screened at a dilution corresponding to 1:32 of original serum. Fluorescein isothiocyanate-conjugated goat antihuman IgG (Chemicon; Merck KGaA, Darmstadt, Germany) or IgM (ThermoFisher Scientific, Inc., Camarillo, CA) was then used as secondary antibody. The slides were read at a magnification of 400 × with a fluorescence microscope (Leica Microsystem, Singapore) by two technicians independently. The endpoint titers of the positive samples were further determined by twofold serial dilutions with a final titer of 1:1024. A titer ≥1:64 of the original serum was considered seropositive and indicated potential exposure to O. tsutsugamushi (Demma et al. 2006, Zhang et al. 2010).
Enzyme-linked immunosorbent assay
A set of serum samples was sent to Naval Medical Research Center in the United States for further evaluation of antibodies against O. tsutsugamushi by enzyme-linked immunosorbent assay (ELISA) (Chao et al. 2011, 2017). Three recombinant 56-kDa antigens derived from the prototype strains of Karp and TA763 (chimeric r56C1), Kato (r56Kt), and Gilliam (r56Gm) were mixed to coat the plates. Serum samples were applied at a dilution of 1:100 and followed by the addition of secondary antibody (Santa Cruz Biotechnology, Inc., Paso Robles, CA) and substrate (Kirkegaard & Perry Laboratories, Gaithersburg, MD). The plates were read at 405–650 nm on an UVmax kinetic microplate reader (Molecular Devices, Sunnyvale, CA). The cutoff values were determined by the optical density of negative controls and the upper prediction limit at 99% confidence interval.
Western blot
To further confirm the specificity of the reactive samples, Western blot was performed using whole-cell antigens (Karp strain) and recombinant 56-kDa proteins (chimeric r56C1 or r56Gm). In brief, 1 μg per well of the antigens was loaded in a Mini-PROTEAN TGX Stain-Free Precast Gel. Electrophoresis and blotting were carried out with a Mini-PROTEAN Tetra Cell Systems and the Mini Trans-Blot module (Bio-Rad Laboratories, Inc., Hercules, CA). Then 5% skim milk was used to block nonspecific bindings of the polyvinylidene difluoride (PVDF) membrane. DBS elutes or serum samples were added to probe the antigens at a dilution corresponding to the original serum of 1:200. Mouse monoclonal antibodies were also used to identify the 47- and 56-kDa antigens (Yao-Hong Biotechnology, Inc., Taipei, Taiwan). The antibody against Orientia antigens was detected by horseradish peroxidase-conjugated antihuman IgG or antimouse IgG and Immobilon ECL substrate (both from Merck KGaA). Chemiluminescence signal was captured by a ChemiDoc-It Imager (UVP, LLC, Upland, CA).
Statistical analysis
All statistical analyses were done using SAS v9.1.3 (SAS Institute, Cary, NC). Categorical variables were compared with chi-squared tests, continuous variables were analyzed with t-tests; p ≤ 0.05 was considered statistically significant.
Results
Human serosurvey, 2016
Of 240 DBSs analyzed, 14 (5.8%) were seropositive for scrub typhus by IFA (Table 1). Ten samples had IgG antibody reactive to O. tsutsugamushi at titers ≥1:64, three samples were at titers ≥1:128, and one sample from a 38-year-old woman had a titer more than 1:1024. Orientia antibodies were only detected in participants >15 years old (median 44.5 years, 22–72 years). A higher positive rate (10/120, 8.3%) was observed in females although the result was not significant (p = 0.98435, chi-squared test).
Human serosurvey, 2003
Serum specimens collected from pregnant women during 2003, in contrast, showed much higher prevalence of Orientia-reacting antibodies. Seropositive rates were 20.4% (116/240) by IFA IgG (Table 2). Six samples (1.1%) showed concurrent IgG ≥1:512 and IgM ≥1:64, which can be considered as evidence of possible recent exposure. Three women became reactive against Orientia antigens (IgM ≥1:64) at their second visit to the clinics, which took place 4 weeks after the first visit, and a ≥4-fold increase in IgG titer was found in the paired samples of another woman. Considering no human cases of scrub typhus has been recognized in the nation to date, the serum samples were sent to Naval Medical Research Center in the United States, and antibodies against Orientia antigens were examined by ELISA. As a result, Orientia-reacting IgG and IgM were detected in 15.4% (88/570) and 18.8% (107/570) of the serum samples, respectively. Thirty two samples (5.6%) yielded positive results by both IgG ELISA and IgM ELISA. Of the 570 participants, 75 (13.2%) were positive and 441 (77.4%) were negative by both IFA and IgG ELISA. The sensitivity and specificity of IgG ELISA were 64.7% and 97.1%, respectively, when using IFA as the reference standard, and the sensitivity and specificity of IgM ELISA were 89.6% and 92.3%, respectively. Fifteen serum samples tested positive by IFA and IgG ELISA were randomly selected and subjected to further Western blot analysis. The existence of Orientia antibodies was confirmed by the results that at least one reactive band was observed against Orientia antigens in each sample (Fig. 2). The corresponding positions of the 47- and 56-kDa antigens were identified by mouse monoclonal antibodies.

Western blot analysis using whole-cell antigens and recombinant 56-kDa protein. The specificity of the serological tests was further confirmed by Western blot. Reactive samples were applied to probe migrating Orientia-specific antigens on the PVDF membrane. *Indicates 47-kDa protein; arrow indicates 56-kDa protein. The 47- and 56-kDa antigens were identified by mouse monoclonal antibodies. w, whole-cell antigens; r56, recombinant 56-kDa protein.
Detection of Orientia Antibodies in Banked Serum Samples by Immunofluorescence Assay and Enzyme-Linked Immunosorbent Assay
ELISA, enzyme-linked immunosorbent assay; IFA, immunofluorescence assay.
Discussion
Two sets of samples collected 13 years apart were examined for the presence of antibodies against O. tsutsugamushi in this study. The DBS samples collected in 2016 exhibited a seropositive rate of 5.8%, a result rather similar to the studies conducted in Kenya and Djibouti (Thiga et al. 2015, Horton et al. 2016, Maina et al. 2016). However, general population, instead of febrile patients, was involved in this study, suggesting the possibility of a higher positive rate if samples from febrile patients were used. In contrast with Taiwan and Japan (Bang et al. 2008, Kuo et al. 2011), our research reported that adult females were more likely to be seropositive, and the same trends were observed in the study in Kenya, probably due to the traditional lifestyle in the area: women are responsible for gathering food in the field while men go out fishing. Regularly passing through the grasslands made women more vulnerable to chigger bites. The sampling method of nonproportional randomization was utilized in this study to increase our chance to detect positive samples, but it also led to less representative data since the sampling size was too small. Our findings revealed that Orientia exposure was likely to occur in the nation where no relative microbe was ever reported. The extent of exposure and its associated disease require further epidemiological investigation.
In contrast, relatively high prevalence of antibodies (20.4% by IFA) was found in serum samples of pregnant women. IFA results of IgG ≥1:512 and IgM ≥1:64 and ELISA results of concurrent positive IgM and IgG antibodies were suggestive of recent (for the sampling time in 2003) exposure to Orientia bacteria. Seroconversion was observed in a woman with repeated samples collected 4 weeks apart as well. These positive banked serum samples indicated that the potentially pathogenic bacteria have been present in the nation for at least a decade but unrecognized. Malaria used to be the prevailing vector-borne disease in the DRSTP, patients presented with febrile illness were presumably treated as malaria. Moreover, the antibiotic treatment of scrub typhus, doxycycline, is also recommended as an antimalarial prophylactic drug. Both misdiagnosis and the collateral benefit of antimalarial treatment would contribute to the neglect of scrub typhus. Further studies should be carried out to explore Orientia infection among febrile illness patients.
The current gold standard assay for the detection of scrub typhus antibodies is IFA. However, the criteria used to determine seropositive results were lack of consensus. With studies differentiated by purpose, 1:50 seemed to be the most widely used value in seroepidemiologic studies although a range of cutoff values (1:10–1:400) have been reported (Blacksell et al. 2007). Our study employed the criterion of a dilution of 1:64 as the cutoff value for IFA, and as a result, a higher seropositive rate of 20.4% was observed comparing with IgG ELISA. Considering the latter assay was performed at a dilution of 1:100, a rather similar result could be found in the extensive dilution for IFA. The sensitivity and specificity of IgG ELISA were also increased to 89.0% and 96.9% when using a cutoff value of 1/128 dilution of the original serum for IFA. Having no clue to the circulating serotype, the study used Karp strain-infected whole cell antigens to coat the IFA slides for the detection of Orientia antibodies. It is not uncommon to take advantage of the antigenic cross-reactivity to examine rickettsial infections; in fact, it was the base of the first serological test for rickettsiosis, the Weil–Felix test (Wilson 1920, Raoult and Dasch 1995). Different degree of cross-reactivity has been reported between serotypes and species of Orientia. Although Karp-like strain provided broader antibody cross-reactivity, Gilliam-like strains and Shimokoshi serotype appeared to be less cross-reactive than the others (Izzard et al. 2010, James et al. 2016, Sando et al. 2018). The difference of seropositive rates determined by IFA and ELISA might also be due to the selection of antigens. This study utilizing only Karp strain of Orientia for IFA could overlook infections of other serotypes. Additional isolation of the pathogens and molecular analysis would provide better understanding of the antigenic and genetic properties of the Orientia sp. circulated in the DRSTP.
Since early 90s, sporadic reports have described scrub typhus-like illness in returning travelers from the countries around the Gulf of Guinea (Osuga et al. 1992, Ghorbani et al. 1997). The detection of Orientia sp. DNA in rodents in Senegal gave supportive proof of the pathogen lurking in West Africa (Cosson et al. 2015). Our findings of Orientia exposure in the DRSTP provided additional evidence for a possibly wider distribution of scrub typhus. Further investigation regarding the natural transmission cycle of Orientia sp. in the DRSTP should be conducted. Scrub typhus is a treatable disease. Early access to health care systems and proper antibiotic treatment would greatly reduce the mortality. It is our hope that the results of this study will raise awareness of the threat and eventually benefit better diagnosis.
Conclusions
Orientia-reacting antibodies were detected in samples from the DRSTP. The positive rates were 5.8% for DBSs collected in 2016 and were 20.4% for archived serum samples from pregnant women in 2003 by IFA. The study provided serologic evidence of Orientia sp. in West Africa and offered referential value for disease prevention and diagnosis for travelers and physicians.
Footnotes
Acknowledgments
We thank the Taiwan Anti-Malaria Advisory Mission for its enthusiastic participation and the project leader, Dr. Jih-Ching Lien, for his professional and technical assistance. This study was supported by Taiwan Ministry of Foreign Affairs. We are also grateful to Dr. Maria de Jesus Trovoada dos Santos and Mr. João Viegas d´Abreu for their efforts in communication with the local participants and laboratory workers. This study was financially supported by grants from the Ministry of Science and Technology Council (103-2314-B-002-036-MY2 to K.H.T.), the Henry M. Jackson Foundation (contract #898796 to K.H.T.), and Naval Medical Research Center Work Unit 6000.RAD1.J.A0310.
Authors' Contributions
K.H.T. and T.Y.Y. participated in the design of the study and drafted the article. Z.Z., C.C.C., and W.M.C. provided r56-kD recombinant proteins and performed ELISA. P.Y.S. and K.H.T. provided guidance for the experiments. T.Y.Y. performed the IFA assay. L.F.T. and A.V.A.C. were involved in the recruitment of the study subjects and the collection of human samples. K.H.T., T.Y.Y., C.C.C., W.M.C., L.F.T., and P.Y.S. reviewed the data and the article. All authors critically reviewed and approved the final article.
Disclaimers
The use of these samples was approved (PJT-13-13) by the Naval Medical Research Center Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human subjects. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of Navy, Department of Defense, or the U.S. Government. Wei-Mei Ching and Chien-Chung Chao are employees of the U.S. Government. This study was prepared as part of their official duties. Title 17 U.S.C. §105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. §101 defines a U.S. Government work as a work prepared by military service member or employee of the U.S. Government as part of that person's official duties.
Author Disclosure Statement
No competing financial interests exist.