
Abstract
Zoonotic diseases represent a significant public health concern worldwide due to the emergence/re-emergence of vector-borne diseases in the last decade. Ticks are the most important vectors in the northern hemisphere and can transmit diseases such as Lyme disease, human granulocytic anaplasmosis, and spotted fever rickettsioses, among others. Therefore, there is a growing need to develop better and faster diagnostic tools that can detect zoonotic human pathogens in clinical samples. In this study, we present the results for a new kit tick-borne bacteria flow chip (TBFC), which allows the simultaneous screening of seven different bacterial pathogens in human samples using a DNA flow technology platform (hybriSpot system). The analytical sensitivity and specificity of the TBFC were calculated spiking bacterial DNA in human DNA samples, and the results were compared with an in-house single PCR-reverse line blot (RLB) routinely used for diagnosis at the National Center for Microbiology in Spain. The analytical sensitivity and specificity of the TBFC were almost identical to the PCR-RLBs used in diagnosis. In addition, samples from patients (n = 212) with a wide range of clinical signs/symptoms consistent with multisystem disorders suggestive of a tick-borne infection were tested using the TBFC, and the results were compared with those obtained by PCR-RLB. The concordance of both methods using patient samples was 97.2%. The TBFC kit is a rapid new and cost-efficient diagnostic molecular tool capable of detecting tick-borne pathogens in clinical samples.
Introduction
The emergence of vector-borne diseases is primarily caused by anthropogenic factors that have contributed to the expansion of the geographical distribution of mosquito and tick-borne diseases (Kilpatrick and Randolph 2012). Epidemics of vector-borne pathogens have dramatically changed in recent years, as we have witnessed the introduction of Zika and West Nile viruses in the United States (Roehrig 2013, Metsky et al. 2017), Crimean–Congo hemorrhagic fever in southwestern Europe (Papa et al. 2008, ECDC 2016, Ramirez de Arellano et al. 2017), and the continuous emergence of Lyme disease (LD) throughout the northeast of the United States as well as throughout central Europe (Rizzoli et al. 2011, Nelson et al. 2015). In addition, the continuous increase of human cases of anaplasmosis, ehrlichiosis, and rickettsioses (Vouga and Greub 2016), as well as the description of new pathogens (Jado et al. 2007, Huber et al. 2010, Welinder-Olsson et al. 2010, Sarksyan et al. 2012, Pritt et al. 2016), further proves the resurgence of tick-borne diseases in the northern hemisphere.
Ticks are the most important vectors for infectious diseases in the northern hemisphere and second only after mosquitos worldwide. As a result, there is an increasing public health interest in tick-borne pathogens. Ticks play two critical roles in the epidemiology of tick-borne diseases. On the one hand, ticks are required to maintain active enzootic cycles, facilitating the transmission of the pathogen to a wide range of vertebrate hosts. On the other hand, ticks can also bite and transmit diseases to humans. Most notably, while some pathogens are vector specific, others can be transmitted by several tick species. Also, it is common that one tick species vectors more than one pathogen. One example of this is the Ixodes ricinus complex, a group of tick species distributed in almost all geographical areas of the world that can transmit several bacterial pathogens, including Anaplasma phagocytophilum, Borrelia burgdorferi sensu lato, and Rickettsia Helvetica, and it is suspected to also transmit Bartonella species (Rizzoli et al. 2014).
Many pathogens present in ticks, including Rickettsia spp., B. burgdorferi, A. phagocytophilum, and Ehrlichia spp., are recognized as important emerging vector-borne pathogens and other forms of transmission are rare. Another tick-borne pathogen such as Francisella tularensis, the agent of tularemia, can be transmitted by different means such as aerosols, ingestion, direct contact, and vectors, including flies and ticks (Petersen et al. 2009, Zellner and Huntley 2019). Despite that the transmission of F. tularensis is not not strictly associated with ticks, half of the cases of tularemia in the United States are associated with ticks (Eisen 2007, Rosenberg et al. 2018). Members of the genus Bartonella are typically considered to be transmitted by fleas but they have been detected in ticks and I. ricinus has been shown to be a competent vector (Cotte et al. 2008). Moreover, a case of bartonellosis has been associated with a tick bite (Angelakis et al. 2010).
Although human cases of Q fever are associated with aerosols, tick bites remain a potential risk for humans (Janbon et al. 1989, Maurin and Raoult 1999, Rolain et al. 2005). At least seven tick species have been shown to to be competent vectors for Coxiella burnetii (Duron et al. 2015). Moreover, the reference virulent strain C. burnetii Nine Mile was isolated from a guinea pig experimentally infested with Dermacentor andersoni (McDade 1990). Despite several studies having found a strong correlation between the presence of ticks and Q fever in cattle (Psaroulaki et al. 2006), the vector capacity of ticks under field conditions remains unknown (Duron et al. 2015). Similarly, C. burnetti has been detected in patients bitten by ticks (Carrascosa-Porras et al. 2007, Angelakis et al. 2010) and in patients with coinfections with other tick-borne pathogens (Janbon et al. 1989, Rolain et al. 2005). However, in these cases, exposure to aerosols cannot be ruled out.
Importantly, the onset of tick-borne infections in patients frequently presents as a febrile illness, which makes differential diagnosis difficult (Wormser 2006, Ismail et al. 2010, Bakken and Dumler 2015, Biggs et al. 2016). Furthermore, as the disease progresses, organs and tissues may be involved, triggering cardiac, neurological, respiratory, and organ failure complications (Parola and Raoult 2001, Dana 2009, Buckingham 2015). Therefore, a rapid differential early diagnostic tool is needed to treat patients promptly with adequate antibiotic therapy. However, many of the routine diagnostic tools available for the diagnosis of tick-borne diseases only target one pathogen. This represents a tremendous limitation in the diagnosis of a tick-borne infection, and often results in a time-consuming diagnosis. In addition, some of the gold standards for detection of tick-borne diseases are based on serology, which represents another limitation for an early diagnosis since antibodies can take up to 14 days to be detected (Brouqui et al. 2004, Dana 2009).
Molecular methods have been seen as an alternative for early diagnosis and detection of tick-borne diseases in human samples, as well as for epidemiological surveys in ticks and mammalian hosts. Most molecular methods are based on the amplification of conserved genes using PCR-based approaches. For the detection of pathogens in ticks, PCR-reverse line blot (RLB) approaches have been used extensively (Rijpkema et al. 1995, Toledo et al. 2009a, Jahfari et al. 2016) as well as real-time multiplex PCR (Wroblewski et al. 2017) or mass tag PCR (Tokarz et al. 2009) among others. Nonetheless, these molecular methods were designed to detect some, but not all, tick-borne bacteria or they need several steps to detect a pathogen, making them cumbersome and time-consuming for clinical use. Although most of the molecular methods have a reasonable detection limit, many fail to be tested using human samples to determine their sensitivity and specificity.
Here we present the results of a new diagnostic kit, TBFC, that can simultaneously detect seven different agents (Anaplasma, Bartonella, Borrelia, Coxiella, Ehrlichia, Francisella, and Rickettsia) using a DNA flow technology platform (hybriSpot).
Methods
Clinical sample collection
The study was retrospective and noninterventional. All clinical samples included in the study belonged to the collection reference number C.0004468 of the collections section from the official Biobank of the Institute of Health Carlos III (ISCIII), and were previously anonymized in compliance with Spanish law (Organic Law 15/1999 on personal data protection and law 14/2007 on Biomedical Research), respecting individual privacy rights. Samples included in the study were received by the Special Pathogens Reference Laboratory (Centro Nacional de Microbiología, ISCIII) for diagnostic purposes. No demographic data were included in the study.
All the samples included in the study came from patients (n = 212) who presented a broad range of clinical signs/symptoms consistent with multisystem disorders that could be suggestive of an infection caused by any of the pathogens included in the panel of the TBFC kit. On the contrary, human DNA used to spike positive controls came from CSF or biopsies from patients who tested negative to the pathogens included in the TBFC.
There were a wide variety of clinical samples from patients (Table 1), including fresh tissues (cutaneous, hepatic, cardiac, lymph node biopsies, skin lesions, and vascular lesions) and body fluids (blood, lymph node aspirates, CSF, and exudates).
Number of Clinical Samples Positive by Both PCR-Reverse Line Blot and Tick-Borne Bacteria Flow Chip
This column shows the number and percentage of samples that had conflicting results.
Conflicting results for Bartonella and Francisella (n = 2).
Francisella (n = 1).
Rickettsia (n = 1).
Bartonella (n = 1).
RLB, reverse line blot; TBFC, tick-borne bacteria flow chip.
DNA extraction
Samples were processed using either the QIAamp DNA blood mini kit (QIAGEN, Hilden, Germany) or the QIAGEN Tissue kit (QIAGEN) for DNA extraction from body fluids and fresh tissues, respectively. Samples were treated overnight with a proteinase K solution (20 mg/mL) followed by a final step of 15 min at 100°C for inactivation of the protease. The DNA concentration was measured using the NanoDrop ND-1000 spectrophotometer (NanoDrop Technologies, Wilmington, DE).
Around 200 ng of DNA from each sample was analyzed with a conventional in-house PCR followed by an RLB for diagnostics purposes, and the same amount of DNA from all samples was analyzed retrospectively with the commercial TBFC kit (Master Diagnostica, Granada, Spain).
Molecular detection
All the samples were tested with routine in-house single PCRs with specific biotinylated primers followed by an RLB for the specific detection of each of the pathogens included in this study. Primers and probes used are listed in Table 2.
Oligonucleotide Sequences of Primers and Probes Used for Single PCR-Reverse Line Blot for the Detection of Tick-Borne Bacteria
Probes are in bold.
BLU, B. lusitaniae probe; PAF, B. afzelii probe; PGA, B. garinii probe; PH, B. henselae probe; PQ, B. quintana probe; PSL, sensu lato probe; PSS, senso stricto probe; PVA, B. valaisiana probe.
Briefly, PCR amplifications for each bacteria genus were carried out individually using biotinylated primers in an MJ Research PCT-200 (Ecogen, Barcelona, Spain) as described previously (Toledo et al. 2009a). Subsequently, an RLB was performed hybridizing PCR products to specific probes with a C6 amino-link modification and detected using immunoenzymatic chemiluminescence (Super Signal West Dura Extended Duration Substrate; Pierce Biotechnology, Rockford, IL), as previously described (Jado et al. 2006).
The sensitivity of the PCR-RLBs was assessed by spiking B. burgdorferi, C. burnetii, and F. tularensis genomic DNA (103, 102, 10, and 1 genome equivalents [GE]) or plasmid copies (PCs) with inserts of synthetic DNA (in the case of A. phagocytophilum, Bartonella henselae, Ehrlichia ewingii, and Rickettsia conorii) in distilled water and human DNA (200 ng), as previously described (Jado et al. 2006, Escudero et al. 2008, Toledo et al. 2009a,b). The genes targeted for each pathogen as well as the primers and probes are summarized in Table 2.
TBFC kit
The TBFC is intended for the simultaneous qualitative detection of DNA from seven different genera of tick-borne bacteria, Anaplasma, Ehrlichia, Borrelia, Bartonella, Coxiella, Rickettsia, and Francisella, using a multiplex PCR followed by reverse dot blot automatic hybridization into a macroarray CHIP based on DNA-Flow Technology (hybriSpot). The primers and probes were designed to cover highly conserved gene regions (Table 3). This design allows the kit to detect a broad spectrum of species from each genus using species-specific probes as well as new variants not yet characterized by using generic probes. New species need to be confirmed by DNA sequencing.
Tick-Borne Bacteria Flow Chip Primer and Probe Sequences Used for the Detection of Tick-Borne Bacteria
Primers were divided into two multiplex reactions.
The kit offers the amplification of bacterial DNA by two multiplex PCRs containing all primers for the specific amplification of the seven bacteria genera and two sets of primers for the amplification of two internal controls. One internal control amplifies a fragment of human genomic DNA, and the other amplifies a synthetic fragment (already included in the PCR mix) (Anda et al. 2012, Quarsten et al. 2015) to detect the presence of PCR inhibitors (Table 3). After PCR amplification, the biotinylated PCR products are automatically hybridized to specific DNA probes for each genus (Table 3), and immobilized onto a nylon membrane (tick-borne bacteria chip). The hybridization signals are developed by a colorimetric immunoenzymatic reaction (streptavidin/alkaline phosphatase and NBT-BCIP chromogen). The substrate/chromogen reaction generates a dark purple precipitate signal in the position where the PCR amplicon hybridized with the specific probe. Subsequently, the signal spots are automatically captured and analyzed by the software hybriSoft (Anda et al. 2007, 2011, 2012).
Analytical sensitivity and specificity of the TBFC kit
To determine the limit of detection for seven different pathogens included in the TBFC panel, we spiked 104, 103, 102, and 10 GE (B. burgdorferi, C. burnetii, and F. tularensis) or PCs (A. phagocytophilum, B. henselae, E. ewingii, and R. conorii) in either water or water containing 200 ng of human DNA. The limit of detection was established using the concentration in the sample for which 100% of positive results were obtained when analyzed with hybriSoft software, establishing a threshold value of 4 (gray intensity) (Supplementary Table S1).
GE and PC for each pathogen were calculated as follows:
N = mass in ng
X = length of the plasmid or genome in bp
Similarly, the analytical sensitivity of the TBFC for the simultaneous detection of all pathogens was calculated by spiking 103–104 GEs and PCs from each pathogen in water containing 200 ng of human DNA (Fig. 1).
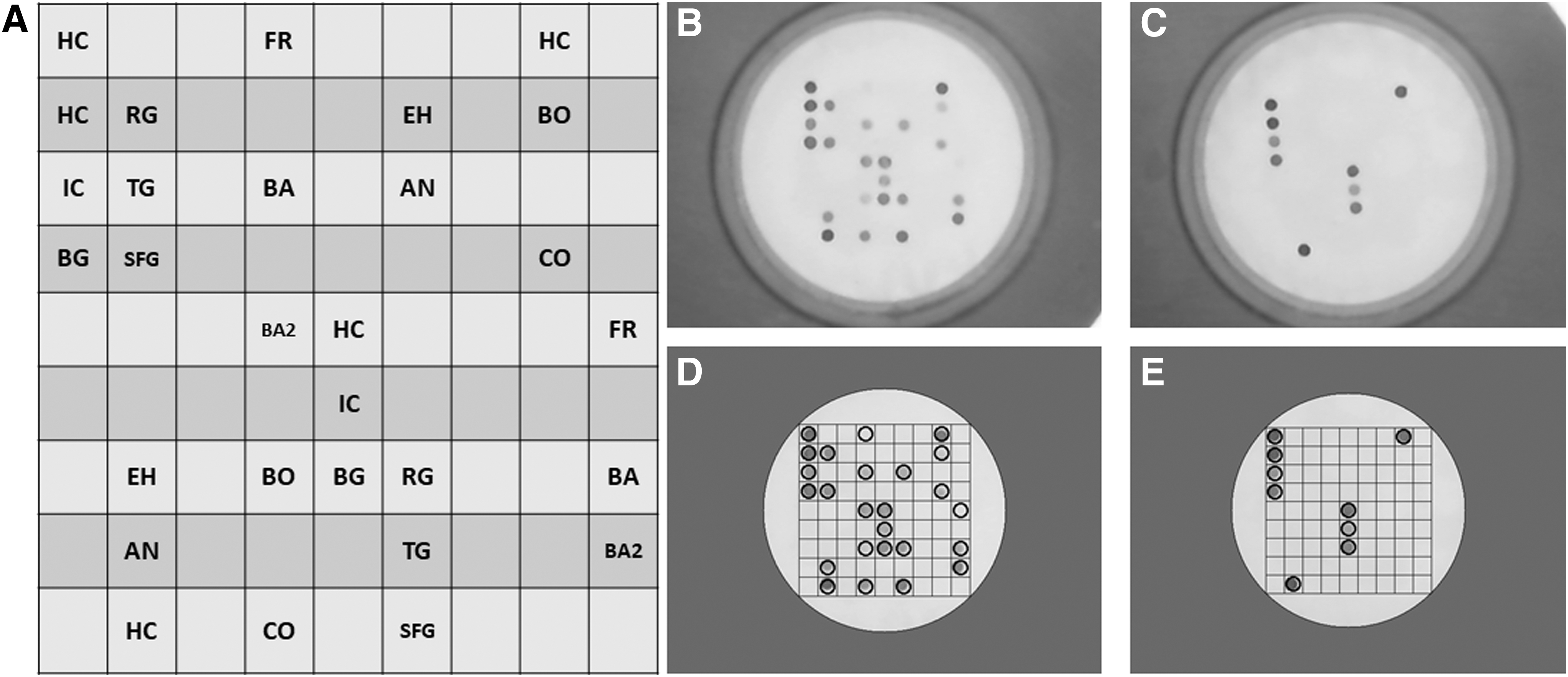
Simultaneous detection of Anaplasma spp., Bartonella spp., Borrelia spp., Coxiella burnetii, Francisella spp., and Rickettsia spp. on a TBFC.
The analytical specificity was tested against a comprehensive panel of bacterial species. Each probe was analyzed for potential cross-reactions against the other pathogens included in the kit as well as other nontick-borne bacteria (Legionella pneumophila, Mycoplasma pneumoniae, and Chlamidophila pneumoniae).
Conflicting samples were analyzed by a third independent molecular method
Samples with conflicting results (n = 6) for Bartonella spp., Francisella spp., and Rickettsia spp., were analyzed by a third independent molecular method. The sensitivity of these methods was similar to those used for single PCR-RLBs. Conflicting samples for Francisella spp. were analyzed by a multitarget real-time TaqMan PCR assay targeting the ISFtu2 and tul4 as previously described (Versage et al. 2003). Conflicting samples for Rickettsia spp. were analyzed with an unpublished in-house real-time PCR targeting 23S-5S rRNA intergenic spacer (Supplementary Table S2). Finally, a multilocus sequence typing (MLST) that targets eight different genes was used for the detection of Bartonella spp., as previously described (Gil et al. 2013). These results were further confirmed by sequencing.
Statistical analysis
For statistical analysis, we used Cohen's kappa coefficient (κ). This coefficient measures the agreement between observers, considering the possibility of agreement occurring by chance (Viera and Garrett 2005).
Results
Analytical sensitivity and specificity of the TBFC kit
In the Supplementary Tables S1 and S3, we summarized the results for the analytical sensitivity and specificity for each pathogen analyzed independently or simultaneously in a mixture containing DNA of the seven pathogens included in the TBFC kit. The limit of detection of the TBFC kit for each pathogen ranged between 1000 and 10,000 GEs or PCs in human DNA samples, whereas in water they were an order of magnitude lower, 100–1000 GEs/PCs (data not shown). Importantly, the sensitivity of the TBFC kit did not change when all pathogens were tested simultaneously (Fig. 1).
The analytical specificity was tested against a comprehensive panel of bacterial species. Each probe was analyzed for potential cross-reactions against the other pathogens included in the kit as well as other nontick-borne bacteria (L. pneumophila, M. pneumoniae, and C. pneumoniae [data not shown]). The results for the analytical specificity are summarized in Supplementary Table S1.
Results of TBFC kit using clinical samples
To test the use of the TBFC kit for clinical diagnosis purposes, 212 clinical samples from the collection reference number C.0004468 were analyzed by an in-house PCR-RLB and the TBFC kit. The results for both methods are summarized in Table 2 and Supplementary Table S3. Anaplama and Ehrlichia species are not reported in clinical samples due to the lack of positives in the collection.
Bartonella detection
A total of 32 samples were positive for Bartonella by both methods, which represents an agreement of 99.07% (κ = 0.964) (Supplementary Table S3). There were two positive samples for RLB that were negative for TBFC. These two samples were negative for Bartonella when analyzed by a third independent method; an MLST that targets eight different genes for detection (Gil et al. 2013). The positive samples analyzed include the following: biopsies (n = 18), exudates (n = 10), blood (n = 2), and lymph node aspirates (n = 2) (Table 1).
Borrelia detection
Both the TBFC and the RLB detected 16 samples positive for Borrelia. Among the type of samples analyzed, there were biopsies (n = 7), blood (n = 8), and CSF samples (n = 1) (Table 1). The positive agreement for both methods was 100% (n = 16); (κ = 1) (Supplementary Table S3). Also, these samples were compared, when available, with the results from the serology test (Supplementary Table S4).
Coxiella detection
A total of 24 cases of Q fever were detected by both methods, showing a 100% agreement (κ = 1) for the detection of C. burnetii (Supplementary Table S3). The samples analyzed include biopsies (n = 17) and blood (n = 7) (Table 1).
Francisella detection
Among the samples analyzed, 18 cases were positive for Francisella by both methods, with an agreement of 99.07% (κ = 0.942) (Supplementary Table S3). Two specimens were TBFC negative but positive by both RLB and the third method used to confirm discrepant results, a real-time PCR for a different gene target (ISFtu2) (Versage et al. 2003).
Rickettsia detection
Twenty-seven positive cases (n = 27) for Rickettsia were detected by both methods, with an agreement of 99.53% (κ = 0.979) (Supplementary Table S3). The only discrepant case was a CSF sample from a patient who had been diagnosed with encephalitis/meningoencephalitis and tested negative by PCR-RLB but positive by TBFC. The sample was confirmed negative by a third independent method, an unpublished in-house real-time PCR targeting 23S-5S rRNA intergenic spacer. The other samples tested were biopsies (n = 21), blood (n = 5), and CSF (n = 1) (Table 1).
In summary, the percentage of positive samples found by both methods for any of the seven bacteria included in the study was 55.1% (n = 118) (Table 1). Bartonella spp was the most common pathogen and was detected by both methods in 14.9% of samples, followed by Rickettsia (12.6%), Coxiella (11.2%), Francisella (8.4%), and Borrelia (7.5%) (Table 1). Multiple pathogens were not detected in any of the samples analyzed by TBFC.
The overall agreement between the two methods was 97.65% (κ = 0.952) (Supplementary Table S3). Five of the six discrepant results were evaluated by a third reference method. Discrepant samples were defined as positive when TBFC or PCR-RLB and an alternative third method were positive, while discrepant samples were defined as a negative when TBFC or PCR-RLB and an alternative third method were negative. Positives were confirmed by sequencing (data not shown). Two cases positive for Francisella with the reference method, but not detected with TBFC, were confirmed as positive, whereas the other three cases (two cases positive for Bartonella with the reference method and negative with TBFC and one case positive for Rickettsia with TBFC but negative with the reference method) were confirmed as negative. The final results of positivity with the TBFC kit, as well as the clinical specificity and sensitivity of the method, are summarized in Table 4.
Sensitivity and Specificity of the Tick-Borne Bacteria Flow Chip Kit Compared with the PCR-Reverse Line Blot After Analyzing Discordant Results with a Third Independent Method
Discussion
In this study, we present the results for a molecular diagnostic tool based on a multiplex PCR followed by a reverse dot blot automatic hybridization into a macroarray CHIP using a DNA-Flow Technology (hybriSpot). We first completed the analytical sensitivity and specificity of the kit to determine the limit of detection of the TBFC as well as potential cross-reactions with other pathogens. The sensitivity of the TBFC was tested for each pathogen independently in the presence of human DNA. Despite human coinfections with tick-borne pathogens being rare, one of the strengths of the TBFC is that it can detect them. To prove that the TBFC detects coinfections, we included positive controls (103–104 PC/GE) for each pathogen. The results confirmed that the TBFC could detect all the pathogens simultaneously without compromising its sensitivity. The limit of detection of the TBFC kit is comparable with the individual PCR-RLB used for diagnostic purposes at the National Center for Microbiology in Spain. These results are in agreement with a previous study in which the TBFC kit was compared with established real-time PCR protocols for the detection of A. phagocytophilum, Bartonella spp., C. burnetii, F. tularensis, and Rickettsia spp. in I. ricinus, obtaining almost identical results (Quarsten et al. 2015). Thus, taking all of this into consideration, the analytical sensitivity of the TBFC kit seems to be adequate for the detection of tick-borne pathogens.
The TBFC platform offers four significant advantages. First, it is rapid and automatized, significantly shortening the time for the diagnosis of tick-borne pathogens. The TBFC kit gives results in 3.5 h, while our in-house PCR-RLB takes 8.5 h for one pathogen. Second, it allows the simultaneous detection of multiple pathogens, which represents an excellent advantage for diseases that display similar symptoms early on. Third, the TBFC can analyze a wide variety of clinical samples with high sensitivity and specificity. Fourth, it is a valuable alternative to serology for early diagnosis.
The TBFC kit was first tested for the detection of each of the seven pathogens included in the panel by spiking bacterial DNA (GE/PC) for each pathogen in 200 ng of DNA extracted from human tissues to mimic patients' samples. This step is critical to prove that the presence of human DNA does not compromise the limit of detection of each pathogen.
The samples screened from patients displayed a variety of signs and symptoms compatible with a tick-borne disease, including fever, skin lesions, endocarditis, adenopathy, meningitis, encephalitis, and facial nerve paralysis among others and included biopsies and body fluids (Table 1). Importantly, these samples included patients negative for the pathogens included in the TBFC that displayed febrile-illness symptoms caused by undetermined etiologic agents or conditions. Because the diversity of unspecific clinical signs is quite common in patients suspected of having a tick-borne bacterial infection, making a differential diagnosis based solely on clinical signs is extremely difficult. As a result, clinicians often send different types of samples, which present a challenge for diagnosis. Therefore, it is crucial to test new potential diagnostic tools on a set of patient's samples to support their use in a clinical setting. The results obtained with the TBFC in clinical samples were compared with those obtained by an in-house PCR-RLB used for clinical diagnosis at the National Center for Microbiology.
Notably, the results obtained after screening 212 samples showed a high agreement value (κ = 0.952) between the TBFC kit and the individual PCR-RLBs. We only found a different result between the two methods in 5 (2.4%) of the samples tested (Table 1), which were reanalyzed using a third independent molecular method to solve the discrepancies and subsequently confirmed by sequencing. After solving the discrepancies, the TBFC showed a slightly higher specificity than the RLB for Bartonella (the two discrepancies were false negatives) and a slighter lower sensitivity than RLB for Francisella (the two discrepancies were false positives), which correlates with a lower limit of detection of F. tularensis by the TBFC kit (Supplementary Table S1). In addition, the discrepancy for the positive result of Rickettsia was confirmed as negative. Finally, the collection used in this study did not include positive samples for Anaplasma/Ehrlichia. Thus, the TBFC kit was tested with human samples for Bartonella, Borrelia, Coxiella, Francisella, and Rickettsia.
The study included samples from patients diagnosed with LD, which is the most prominent vector-borne disease in the northern hemisphere, and relapsing fever (RF) Borrelia. While LD Borrelia is transient in blood and uses the circulatory system to disseminate, RF Borrelia causes a distinct spirochetemia (Cutler 2015). Therefore, direct detection of spirochetes in blood is generally sufficient for the diagnosis of RF Borrelia, while serology is the preferred diagnostic method for LD Borrelia. The TBFC kit has the advantage of detecting both LD and RF Borrelia, but it cannot differentiate between them. Thus, additional clinical data or tests are required for a precise diagnosis despite both being effectively treated with doxycycline (Cutler 2015, Sanchez et al. 2016). In patients suspected of having LD, serology, which is the gold standard for diagnosis, is not recommended during the first 2 weeks of infection due to the lack of a consistent detectable antibody response. In this scenario, molecular tools can be an alternative. We compared the PCR-RLB and TBFC results with those obtained by serology when it was available (Supplementary Table S4). One of the positive samples by both molecular methods had a negative serology. This sample came from a patient with an erythema migrans, a skin lesion that is characteristic of early LD (Masters 1993) and sufficient for diagnosis (Aguero-Rosenfeld et al. 2005, Wormser 2006). Also, a blood sample that came from a patient with an early stage of LD was inconclusive by serology but was found positive by TBFC and PCR-RLB. These results highlight the advantage of molecular methods for the diagnosis of early LD when an erythema migrans is not present.
Although the TBFC can detect coinfections, none of them was detected in the samples tested. Coinfections with tick-borne pathogens are possible although their frequency depends on a variety of factors such as the vector competence of the tick species involved and the presence of infected vertebrate hosts, among others. Most of the samples analyzed came from patients from central Spain where the most prominent tick species, Hyalomma lusitanicum and Dermacentor marginatus, are not usually infected with more than one pathogen (Toledo et al. 2009a). Besides, some of the tick-borne pathogens included in the TBFC kit panel such as Bartonella, Coxiella, and Francisella are not strictly or frequently transmitted by a tick bite. Moreover, the primary vector for Bartonella spp. is the flea, and most human cases (caused by B. henselae) are associated with a cat bite or scratch (Windsor 2001), while Q fever (Coxiella) is associated with contaminated aerosol exposure (Maurin and Raoult 1999), and tularemia (Francisella) can be acquired by inhalation, direct contact, ingestion, or an arthropod bite (Foley and Nieto 2010).
Finally, one of the restrictions that RLB has is that detection relies on probes. Therefore, each pathogen requires a specific probe. For genus such as Rickettsia or Bartonella that includes several human pathogenic species and where the description of new species is common, this could represent a limitation. To circumvent this problem, the TBFC includes genus-specific probes for Bartonella, Borrelia, Francisella, and Rickettsia. Thus, the TBFC can potentially detect any, described or undescribed, pathogenic species within these genera, but it cannot determine the species, which would require sequencing.
Overall, the TBFC showed a sensitivity and specificity comparable with the in-house PCR-RLB used for diagnosis at the National Center for Microbiology (Spain) for all the bacteria detected in patients, but it is fully automatized, more rapid, and cost-efficient (the cost for the TBFC is half of the cost of a PCR-RLB for a single pathogen). Importantly, all the samples analyzed came from patients with symptoms compatible with a tick-borne disease, some of which were exposed to animals, bitten by a tick, or came from an endemic area. Therefore, the results obtained by TBFC underscore the importance of having a diagnostic tool that allows a differential diagnosis in patients suspected of having a tick-borne disease. In addition, the TBFC proved to be a robust method independent of the origin of the sample. All pathogens were detected without noticeable inhibition in both biopsies and body fluids, including lymph node aspirates, exudates, CSF, and blood. These results support the use of the TBFC kit for clinical diagnosis in a wide variety of samples.
Conclusions
The TBFC kit is a rapid and highly sensitive and specific diagnostic tool, capable of simultaneously screening multiple bacterial pathogens.
Footnotes
Acknowledgments
The authors thank Dr. Pedro Anda and Dr. Horacio Gil for their input and comments on the article.
Author Disclosure Statement
B.E. and E.L. are employees of Master Diagnóstica. R.E. and I.J. are inventors of the patent “Method and kit for the detection of bacterial species by means of DNA analysis” (EP 1895015 A1), in which the tick-borne bacteria flow chip is based. The other authors declare no conflicts of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.