
Abstract
Background:
Pet-related tick-borne infections constitute an emerging problem in human and veterinary medicine worldwide. In Chile, two pathogens of the Anaplasmataceae family, Anaplasma platys and Ehrlichia canis, have been identified in recent years in dogs and vectors. This epidemiological survey aimed to determine the human and canine seroprevalence of Anaplasma spp. in urban and rural areas of different regions in Chile and to analyze the factors associated with seropositivity.
Methods:
We performed a cross-sectional household-based study in four regions, where healthy adults and their household dogs were included. Households were chosen by double stratified random sampling in urban areas and by convenience sampling in rural areas. Anaplasma seroreactivity was determined by a commercial microimmunofluorescence assay using Anaplasma phagocytophilum antigens. A questionnaire survey was applied to assess risk factors for Anaplasma seropositivity.
Results:
A total of 1105 persons and 905 dogs were included. The overall seroprevalence in humans was 9.4%, ranging from 5.6% in central Chile to 13.7% in the extreme north; in dogs the overall prevalence was 44.0% and ranged from 37.2% in the northern region to 61.1% in central Chile. Risk factors for human seropositivity were lower education and external deworming of dogs, whereas canine seropositivity was associated to urban site, mixed-breed, older animals, and tick infestation.
Conclusions:
This cross-sectional study suggests a broad exposure of both dogs and dog owners to Anaplasma or related agents in Chile. Further epidemiological and clinical studies are necessary to understand the complete spectrum and epidemiology of tick-borne zoonotic infections in the different ecoclimatic regions of Chile.
Introduction
The One Health philosophy has led to a growing recognition of zoonotic human diseases worldwide (Day 2011). Among those are various tick-borne infections caused by intracellular bacteria of the Anaplasmataceae family, which includes several pathogenic Ehrlichia and Anaplasma species as well as new species of uncertain clinical-epidemiological relevance (Kernif et al. 2016). Reasons for the emergence of these infections are multifactorial, most important are advanced molecular diagnostic techniques and increased clinical awareness, but possibly also environmental and climatic changes (Parola et al. 2005, Perez-Osorio et al. 2008, Doudier et al. 2010, Richards 2012, Dugat et al. 2015).
Until recently, the prevalence and distribution of members of the Anaplasmataceae family in Chile were unknown. Since 2006, two important pathogens, Anaplasma platys and Ehrlichia canis have been identified in dogs from Chile (Abarca et al. 2007, López et al. 2012). Both are transmitted by Rhipicephalus sanguineus sensu lato (s.l.), which is widely distributed in Chile, both in urban and rural areas (González-Acuña and Guglielmone 2005, Abarca et al. 2016, Poo-Muñoz et al. 2016, Díaz et al. 2018). In addition, new genotypes and species of Anaplasma, Ehrlichia, and Neoehrlichia have been detected in rodents, birds, and ticks (Müller et al. 2018, Muñoz-Leal et al. 2019a, 2019b).
Human infections caused by pathogens of the Anaplasmataceae family have not been reported so far in Chile, although serological studies indicated that dog owners are exposed to Anaplasma and/or Ehrlichia (López et al. 2003, Abarca et al. 2008). However, the lack of clinical cases has to be interpreted with caution, since infections are notoriously underdiagnosed, for their unspecific nature and difficult diagnosis (Parola et al. 2013). In Chile as in most other South American countries, systematic epidemiological data are lacking and diagnostic tools for this group of pathogens are not widely available. The distribution, prevalence, and clinical relevance of infections with Anaplasmataceae in humans and animals are therefore unknown. The here presented cross-sectional serosurvey first examined humans and their pet dogs of different regions in Chile for their seroreactivity against Anaplasma spp. and identified factors associated with seropositivity.
Materials and Methods
Study population
Samples derived from a field project studying various vector-borne zoonotic infections in humans, canines, and vectors in Chile (Abarca et al. 2012, 2013, 2016). The study was conducted in four regions (Fig. 1) and included the following areas: (1) in Arica y Parinacota Region, the city of Arica and surrounding rural areas (18°28′S, 70°18′W), with dry climate, arid landscape and few vegetation, and human and dog populations of 180,879 and 32,887, respectively; (2) in Coquimbo Region, the city of Coquimbo (29°57′S, 71°20′W) and surrounding rural areas, with semi-arid climate and human and dog populations of 203,036 and 36,916, respectively; (3) in Metropolitana Region, the municipality of Puente Alto (33°37′S, 70°34′W) with 492,915 inhabitants and 11,612 dogs, and the nearby semi-rural municipality of Pirque with 24,180 inhabitants, with Mediterranean climate and extended dry season; and (4) in Araucanía Region, urban and rural areas of Angol (37°48′S, 72°43′W) with a transitional climate from humid mild Mediterranean to markedly rainy, 42,000 inhabitants, and a dog population of 7636. The survey was performed between September 2010 and January 2011 in the Arica y Parinacota and Metropolitana Regions and between October 2011 and February 2012 in the Coquimbo and Araucanía Regions.
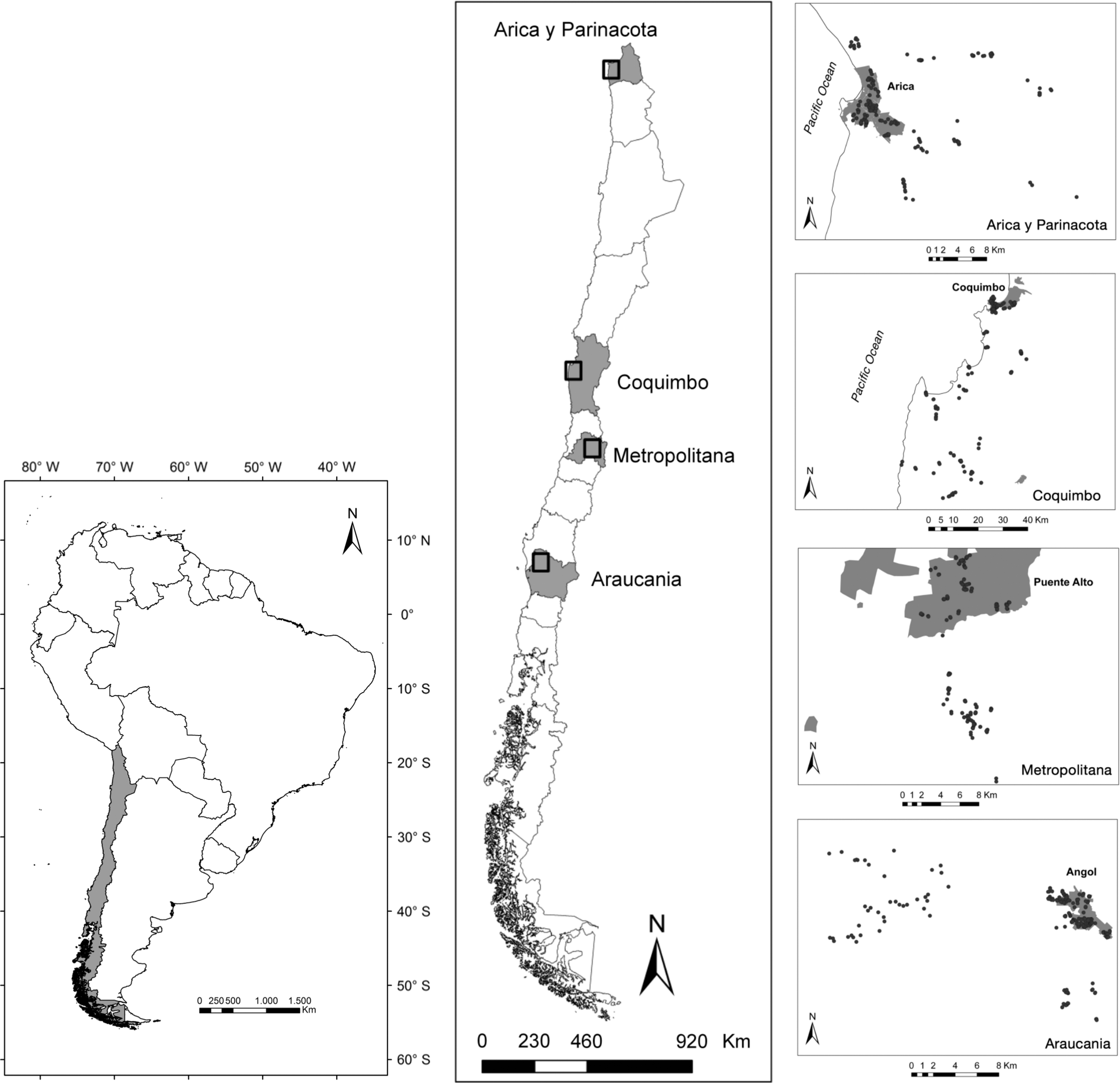
Geographical locations of study sites. The left panel displays the South American continent and Chile (gray shading). The middle panel shows the study localities (black squares) within four different regions (gray shading). The right panels display details of the four study sites, including urban areas (gray shading) and included households (black dots).
Sample size
Population sizes were estimated using national census figure from 2002 (
Study design
In urban areas, double stratified random sampling per building block and household was performed, while in rural areas, convenience sampling was used, until 97 households with canine pets were completed. Households were revisited, if no household member were available at first visit. Individuals were informed about the study, and after written consent was obtained, whole blood was drawn from up to two adults and one dog per household. Geographical locations were recorded using a GPS device. A questionnaire survey was applied to assess risk factors for vector exposure. Questions were related to the household (“site” [urban/rural], “number of people per household,” “number of dogs per household”); to the pet owner (“age,” “sex,” “level of education,” “occupation,” “sleeping with dogs,” “removing ticks,” “past tick bites,” “presence of ticks on clothes”), and to the household's dog (“age group,” “sex,” “purebred,” “allowed to roam freely,” “veterinary controls,” “external deworming”). In addition, dogs were examined by a veterinarian, classifying the level of “tick infestation” as previously described (no ticks, mild 1–10, moderate 11–30, high more than 30) (Tinoco-Gracia et al. 2009). Whole blood specimens from human and dogs were centrifuged on the same day; serum was separated, aliquoted, and kept at −20°C until further analysis.
Serological studies
Human and canine serum samples were examined for IgG antibodies against Anaplasma spp. by a commercial immunofluorescence assay based on Anaplasma phagocytophilum whole-cell antigen (Fuller Laboratories, Fullerton). The test was performed and interpreted according to the manufacturer's instructions. In brief, the antigen containing wells were covered with 10 μL of 1:80 phosphate-buffered saline (PBS)-diluted serum, incubated at 37°C for 30 min in a humidity box, rinsed twice for 10 min in PBS, and incubated with the corresponding fluorescein isothiocyanate-labeled conjugate for 30 min. Slides were then washed again, mounted with buffered glycerin under coverslips, and read using an epifluorescence microscope BX60 (Olympus, Tokyo, Japan) at 400 × magnification.
Statistical analysis
The associations between potential risk factors and Anaplasma seropositivity were estimated using a Generalized Lineal Mixed Model with binomial errors using region as random effect to control for regional differences and “lsmeans” package for estimating p-values (R-Development-Core-Team 2018). Multivariable models were constructed after an initial unconditional univariable analyses. In humans, we used the following explanatory variables: “site,” “number of people per household,” “number of dogs per household,” “age,” “sex,” “education,” “occupation,” “sleeping with dogs,” “removing ticks,” “past tick bites,” “presence of ticks on clothes,” “allowed to roam freely,” “veterinary controls,” “external deworming,” and “tick infestation.” In dogs, the analyses were based on the variables: “site,” “number of people per household,” “number of dogs per household,” “age,” “sex,” “education,” “allowed to roam freely,” “purebred,” “veterinary controls,” “external deworming,” and “tick infestation.”
Ethical approval
The study protocol was reviewed and approved by the Comité Ético Científico (approval no. 12-170) and by the Comité de Bienestar Animal of the Faculty of Medicine (approval no. 12-033), Pontificia Universidad Católica de Chile in Santiago, Chile, and the respective health authorities of the four study regions.
Results
Study population
The study included a total of 921 households, in which 1105 persons and 905 dogs were sampled, which represented 99% and 100% of the calculated sample sizes, respectively. Among the sampled humans, 65% were female; the median age was 46.5 years (Table 1). Participating households owned an average of 2.2 dogs. Most sampled dogs were adults and predominantly male, especially in rural areas (Table 1).
Demographic Characteristics of Human and Canine Study Population in Four Regions in Chile
Seroreactivity
The overall human seroreactivity rate to Anaplasma antigens was 9.4% (90% CI 8.1–11.0), ranging from 5.6% in the central Metropolitana Region to 13.7% in the Arica y Parinacota Region in northern Chile. Human seroprevalence was slightly higher in urban (9.9%) than in rural sites (8.9%) (Table 2). The overall canine seroprevalence was 44% (90% CI 41.3–46.7) with geographical differences ranging from 37.2% in the Coquimbo Region to 61.1% in the Metropolitana Region. In the latter, the prevalence was significantly higher than in all three other regions. Seroprevalence was higher in dogs from urban areas (48.4%) compared with those from rural sites (39.6%) (Table 2).
Prevalence of Anaplasma Antibodies in Humans and Dogs in Four Regions in Chile
CI, confidence interval.
Risk factor analyses
Multivariable analysis by generalized linear mixed models revealed a positive correlation of human Anaplasma seroreactivity with a lower level of education and with external deworming of dogs in the household (Table 3). Canine seropositivity, on the contrary, was positively correlated with urban setting, mixed-breed, older dog age, and infestation with ticks (Table 3).
Multivariable Analysis by Generalized Linear Mixed Models with Binomial Errors of Factors Associated with Anaplasma Seropositivity in Humans and Domestic Dogs
Within past 3 months.
OR, odd ratio.
Discussion
The presented work represents the first systematic study of human and animal exposure to Anaplasmataceae in Chile. In South America, the spectrum, epidemiology, and clinical relevance of most members of this group of human and veterinary pathogens are only vaguely understood (Kernif et al. 2016). Seroprevalence studies constitute the first approach to study magnitude and distribution of exposure to emerging infectious agents (Parola et al. 2013). The study was designed as a representative household-based survey of humans and dogs from four regions in Chile, covering a variety of ecoclimatic conditions and a latitudinal distance of over 2100 km. In tick-borne zoonoses such as anaplasmosis or ehrlichiosis, domestic dogs are not only affected by the diseases but also serve as sentinels, as they are more frequently exposed to the vectors (Cleaveland et al. 2006, Salb et al. 2008, Nicholson et al. 2010). Canine ticks are widely distributed in Chile; the most prevalent is R. sanguineus s.l., which is endemic in all of the study regions (González-Acuña and Guglielmone 2005, Abarca et al. 2016, Poo-Muñoz et al. 2016, Díaz et al. 2018). Furthermore, Amblyomma tigrinum has been described in rural locations in central and northern Chile and Anaplasma triste in rural areas in the extreme north (Abarca et al. 2012, 2016).
With 44%, the study showed a high rate of canine sero-reactivity to Anaplasma spp., which was present across all sites. Similar canine seroprevalence rates have been reported from some southern European countries such as Bulgaria, Spain, and Italy, while in most other countries in Europe and North America, prevalence rates are lower (Amusategui et al. 2008, Ebani et al. 2014, Farkas et al. 2014, Perez Vera et al. 2014, Pantchev et al. 2015, Cetinkaya et al. 2016, McMahan et al. 2016, Evason et al. 2019). In South America, canine anaplasmosis is mainly caused by A. platys and has been reported from all countries except Bolivia (Maggi and Kramer 2019); systematic epidemiological studies, however, are scarce. A study of street dogs from different cities in Colombia reported an Anaplasma seroprevalence of 11% (McCown et al. 2014). Epidemiological studies based on PCR showed canine infection rates of 7.2% in Argentina, 9.1–14.1% in Brazil, and 10.7% in Paraguay (Lasta et al. 2013, Witter et al. 2013, Cicuttin et al. 2016, Perez-Macchi et al. 2019).
In Chile, A. platys has been diagnosed in dogs with canine cyclic thrombocytopenia in the Metropolitana Region (Abarca et al. 2007). This region is highly endemic for the vector of this pathogen, R. sanguineus s.l. (Abarca et al. 2016). Our serosurvey showed that over 60% of dogs of the Metropolitana Region were seroreactive to Anaplasma antigens, suggesting an ubiquitous exposure to Anaplasma, most probably A. platys, in central Chile. The clinical incidence might be significantly lower, since A. platys often causes subclinical infection (Maggi and Kramer 2019).
Canine Anaplasma seroprevalence was second highest (40.2%) in the extreme north of Chile. In this region, E. canis has been identified in dogs with canine ehrlichiosis (López et al. 2012), which is presumably transmitted by the tropical lineage of R. sanguineus (Cicuttin et al. 2015). This lineage has recently been identified in this region (Díaz et al. 2018). Due to the possible cross-reactivity with Anaplasma antigens, E. canis infections might partly be responsible for the detected seroprevalence (Centers for Disease Control and Prevention 2009, Wass et al. 2018). A. platys, however, which is likely transmitted by temperate and tropical lineages of R. sanguineus (Cicuttin et al. 2015), has also been detected by our group in this region (unpublished observations).
The pathogen(s) causing canine seroreactivity rates of about 37% in the Coquimbo and Araucanía Regions are unknown. Since only the temperate lineage of R. sanguineus is endemic in these regions (Díaz et al. 2018), E. canis infections are improbable. A. platys was found in R. sanguineus s.l. in both regions (unpublished observations) and is therefore the most probable source of exposure. Still, other unknown Anaplasmataceae members, as discovered recently in ticks in Argentina and wildlife in Chile, might also be present (Müller et al. 2018, Monje et al. 2019, Muñoz-Leal et al. 2019b, 2019c).
Few data on human Anaplasma exposure and seroprevalence in South America are available. Among 75 rural workers in northern Colombia, 20% were seropositive to A. phagocytophilum antigen, whereas in a similar study with 160 adults from four study sites in Peru, no Anaplasma seroreactivity was found (Máttar and Parra 2006, Moro et al. 2009). The human overall Anaplasma seroprevalence in our study was 9.4%. Interestingly, it was lowest in the Metropolitana Region, which had the highest canine seroreactivity. Since human infections with Anaplasmataceae have yet not been documented in Chile, the cause of the detected seroreactivity remains uncertain. However, a previous seroepidemiological study from the Metropolitana Region in Chile suggests that canine pathogens are the responsible agents. This study demonstrated that the Anaplasma seroprevalence rate was significantly higher in individuals, who were in contact with dogs clinically diagnosed with canine ehrlichiosis/anaplasmosis (Abarca et al. 2008). To our opinion, the most probable explanation of human seroreactivity in the study regions was therefore exposure to A. platys and/or E. canis. The zoonotic role of these two canine pathogens remains uncertain, but human infections with both agents have been reported from USA, Costa Rica, and Venezuela (Maggi et al. 2013, Arraga-Alvarado et al. 2014, Bouza-Mora et al. 2017).
The analysis of risk factors revealed that human Anaplasma seroreactivity was associated with a lower level of education and external deworming of the household's dogs. The first factor might indicate an increased risk of tick exposure due to socioeconomic conditions. The second factor might be associated to the presence and management of tick-infested dogs in the family. Heavy tick infestation on the other hand has been identified as a risk factor for canine infection with Anaplasma spp. in a study from Mexico (Movilla et al. 2016).
Higher canine seroprevalence was found in mixed-breeds, older dogs, and those infested by ticks. In accordance to studies from Brazil, prevalence was higher in urban than in rural areas (Costa-Junior et al. 2013, Vieira et al. 2013). However, the relationship between Anaplasma exposure and urbanicity is not conclusive. A study from central Italy, for example, demonstrated a higher seroprevalence in rural areas (Ebani et al. 2014). Most probably, exposure to Anaplasma varies locally and seasonally, depending on the ecology of transmission in each setting. For our study sites, an analysis of R. sanguineus infestation demonstrated that dogs in the Araucanía Region were heavier infested in urban than in rural areas, while this was reverse in the Arica y Parinacota and Coquimbo Regions (Abarca et al. 2016). The higher Anaplasma seroprevalence in adult and elder dogs most probably reflects a constant force of infection. Similar pattern have been reported for other pathogens in dogs in Chile (Acosta-Jamett et al. 2011). A higher prevalence was observed in mixed breeds compared to pure-breed dogs, the reasons for this are uncertain.
A methodological limitation of the study is the lack of specificity of serological testing for Anaplasmataceae. The A. phagocytophilum antigen used in the study not only cross-reacts with A. platys (Allison and Little 2013) but also with Ehrlichia chaffeensis, E. canis, and Neoehrlichia species (Centers for Disease Control and Prevention 2009, Wass et al. 2018), and possibly with Coxiella burnetii (Santos et al. 2009) and Orientia species (Park et al. 2003). The importance of E. canis in the study site in the extreme north of Chile has been mentioned above. The possible cross-reactivity to Orientia spp. might be relevant in the southern sites, since this pathogen has recently been detected in this region (Weitzel et al. 2019), and dogs showed seroprevalence rates of 11–30% in southern Chile (Weitzel et al. 2018). Another limitation is the focus of our study on canine zoonoses and ticks. Other animals such as birds and rodents, which have been identified as competent reservoirs for A. phagocytophilum (Keesing et al. 2012), might also play a role in the epidemiology of other Anaplasmataceae.
Conclusions
Our study provides first systematic data on the seroepidemiology and risk factors for infection with Anaplasma spp. in healthy adults and their dogs in Chile. The results of the cross-sectional study indicate a broad exposure of both dogs and dog owners to Anaplasma or related agents. This highlights that Chilean physicians and veterinaries should include Anaplasma infections in the differential diagnosis of patients with respective symptoms and that laboratory diagnosis, including molecular and serological test, should be made available. Further studies are necessary to understand the complete spectrum and epidemiology of tick-borne zoonotic infections in the different ecoclimatic regions of Chile.
Footnotes
Acknowledgments
We thank all participants for their support to the study and Teresa Azócar for her laboratory work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the Comisión Nacional de Investigación Científica y Tecnológica (CONICYT), grants FONDECYT no. 1100809 and no. 1130817.