
Abstract
Human ehrlichioses are tick-borne diseases that have been increasing in incidence in the United States during recent years. Ehrlichia chaffeensis is one of the primary bacteria that cause ehrlichiosis in humans, which typically results in fever-like symptoms, but may also be fatal if left untreated. E. chaffeensis infections are reported to the Centers for Disease Control and Prevention (CDC) through the National Notifiable Diseases Surveillance System (NNDSS). This study analyzed the cases of E. chaffeensis infections reported by the NNDSS from 2012 through 2016. There were 6786 cases and the incidence rate was 4.46 cases per million persons per year. The demographic group most commonly infected was white males between the ages of 40 and 64. Infections were most abundant in the southeast and midwest, particularly in Arkansas, Missouri, Tennessee, and Oklahoma, as well as much of the east coast. The number of cases reported each year from 2012 through 2016 was higher than the number reported in any of the previous 4 years. Ongoing surveillance and reporting of tick-borne diseases are critical to inform public health practice and guide disease treatment and prevention efforts.
Introduction
Human ehrlichioses are tick-borne infections caused by bacteria of the Ehrlichia genus, including Ehrlichia chaffeensis and Ehrlichia ewingii (Heitman et al. 2016). A third bacterium, temporarily named Ehrlichia muris eauclairensis, has been observed to cause infections in patients who have spent time in the Minnesota-Wisconsin area (Johnson et al. 2015). If ticks carrying these bacteria feed on humans for an extended period (>24 h), flu-like symptoms can begin to appear after 7 to 14 days (O'Connell 2017). Symptoms include fever, body aches, nausea, vomiting, fatigue, headache, chills, loss of appetite, joint pain, confusion, and rashes (Kohanna 2016). Infections are potentially fatal if left untreated (Turkington and Ashby 2007). E. chaffeensis infections respond best to treatment with doxycycline, particularly within the first few days of infection (Ismail et al. 2010). Doxycycline is effective at preventing further complications, and there has been no documentation of resistance to doxycycline or relapses after sufficient treatment (Ismail et al. 2010). If fever symptoms do not respond to doxycycline, it is possible that E. chaffeensis is not the source of infection (Bakken and Dumler 2002).
E. chaffeensis infections are most commonly reported from the southeastern and south-central regions of the United States (Dahlgren et al. 2011). The geographical distribution of lone star ticks (Amblyomma americanum), which are known to carry the E. chaffeensis, overlaps broadly with that of reported infections (Paddock and Childs 2003). Lone star ticks are aggressive, with both nymphs and adults capable of transmitting infections (Killmaster et al. 2014). E. chaffeensis infects white blood cells circulating in the bloodstream, which also poses the risk of the pathogen being transmitted through blood transfusions (Paddock and Childs 2003).
In this study, we summarize the passive surveillance data on E. chaffeensis infections reported to the Centers for Disease Control and Prevention (CDC) from 2012 through 2016. We characterize the epidemiology of reported cases, including demographic profiles, incidence rates (IRs), and the spatial/temporal patterns of infections. We also compare the number of cases reported annually from 2012 through 2016 with the number of cases reported during the previous 4 years.
Materials and Methods
National Surveillance Systems
Individual states and territory health departments use the National Notifiable Diseases Surveillance System (NNDSS) to report surveillance data to the CDC using manually completed Tick-Borne Rickettsial Disease Case Report Forms (CRFs) (
Case definition
In general, there are several symptoms found during the first week of clinical disease (Paddock and Childs 2003). Thrombocytopenia is usually observed while leukopenia is always present (Rikihisa 2015). Anemia generally occurs, however, it begins to appear later than thrombocytopenia or leukopenia (McCollough 2018). These infections can damage the liver, causing hepatic transaminases to experience mild-to-moderate elevations (Sehdev and Dumler 2003). The optimal diagnostic test, with candidates including polymerase chain reactions (PCR), serologic tests, culture isolation and immunohistochemical (IHC) assays, and blood smear microscopy, depends on the timing relative to symptom onset and the type of specimens available for testing (Ismail et al. 2010). The type of infection can be determined based on where the infection occurs in the blood (Paddock and Childs 2003). E. chaffeensis mostly infects monocytes (Miura et al. 2011), while E. ewingii usually infects granulocytes (Regunath et al. 2017).
Analysis
Cases reported from January 2012 through December 2016 were included in the analysis. If the date symptoms began to appear was not reported, the earliest known date associated with that particular case was used to represent that infection. IRs were calculated by year, state, and age, using the U.S. Census Bureau population estimates. IRs were not reported for race and ethnic groups because a large proportion of cases had these data missing. State populations were only considered at risk during the years in which ehrlichiosis was reportable. This report does not include confidence intervals or results from statistical hypotheses testing since reported cases cannot be generalized to unreported cases or to other reporting time periods (Dahlgren et al. 2011, Heitman et al. 2016).
Results and Discussion
From the NNDSS, a total of 6786 new cases of E. chaffeensis infection were reported from 2012 through 2016. The mean IR during this period was 4.5 cases per million PYs (1128 cases in 2012, 1518 in 2013, 1475 in 2014, 1288 in 2015, and 1377 in 2016). The number of cases reported each year from 2012 through 2016 was higher than the number reported within the United States in any of the previous 4 years (Heitman et al. 2016) (Fig. 1).
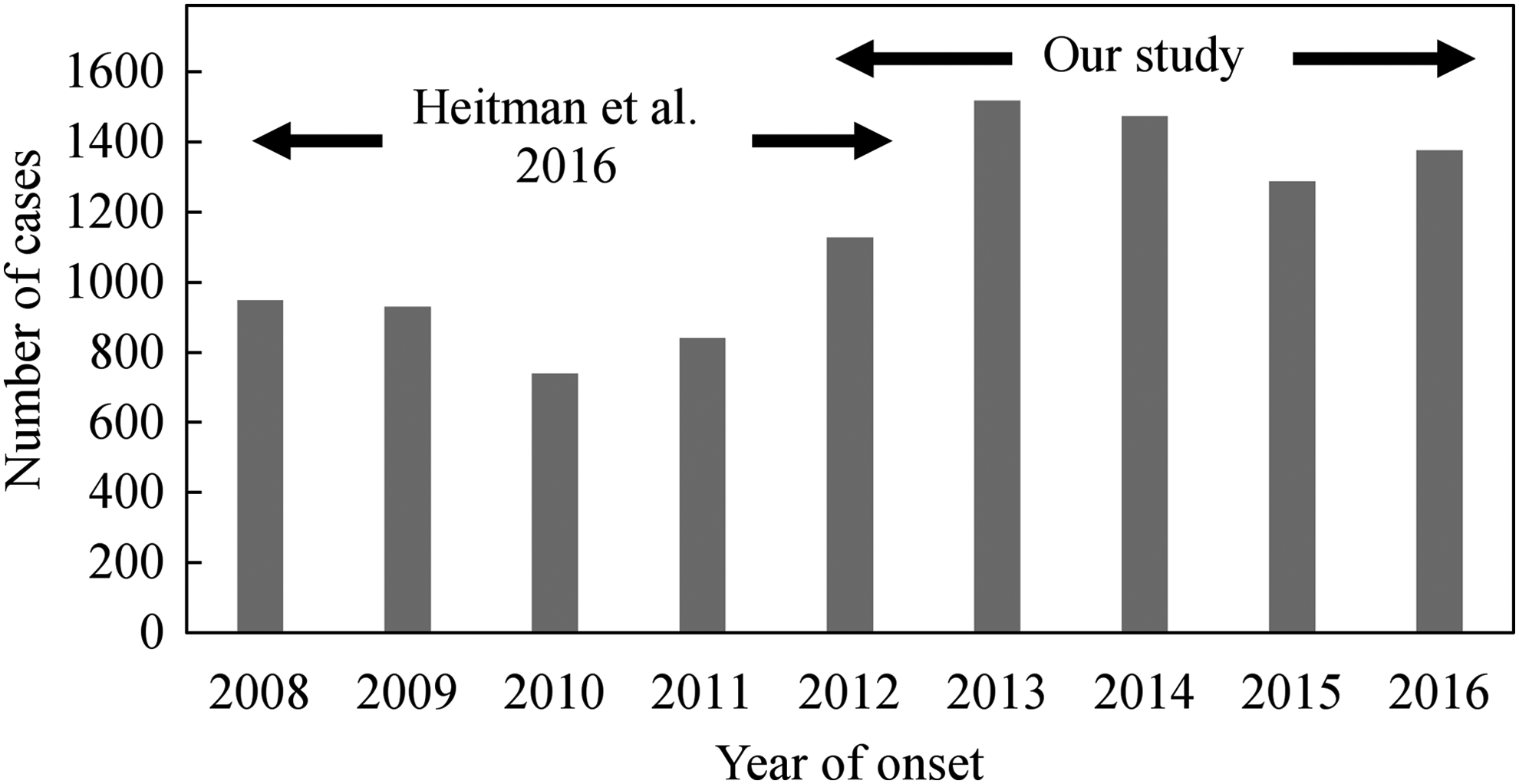
Number of cases of Ehrlichia chaffeensis infections reported annually in the United States from 2008 through 2016. Data from 2008 through 2012 are from Heitman et al. (2016), and data from 2012 through 2016 are from the Nationally Notifiable Diseases Surveillance System.
The primary demographic group affected by E. chaffeensis infection in the United States was elderly white males (Table 1). More infections were reported in males (55.1%; IRs = 4.96) than in females (44.4%; IRs = 3.94), in whites (67.5%; IRs = 3.86) than in other races, and in individuals 40 to 64 years old (45.0%; IRs = 6.16) and older than 65 years (33.2%; IRs = 10.34) than in other age groups. The majority of reported infections were among non-Hispanics (68.7%; IRs = 3.70), although ethnicity was unknown in many cases (29.4%). These infection patterns likely reflect behavioral differences among demographic groups, which affect outdoor activity patterns (Bayles et al. 2013), as well as age-specific physiological differences. White males may be more likely to spend time outside in areas where ticks are abundant, with middle-aged and, particularly, elderly individuals more likely to develop severe infection leading to hospitalization and application of diagnostic tests than younger (18- to 40-year olds) individuals with stronger immune systems. Of course, these results also reflect an inherent reporting bias due to the unequal availability of health care among demographic groups (Jones et al. 2012).
Demographic Profiles Among Ehrlichia chaffeensis Infection Cases, from 2012 Through 2016, United States
The number of incidence cases is from the Nationally Notifiable Diseases Surveillance System, and the cases per million persons at risk (IRs) are calculated based on data from the Nationally Notifiable Diseases Surveillance System and the U.S. Census Bureau.
IRs, incidence rates.
The geographic distribution of E. chaffeensis infections was concentrated in Missouri (19.5% of the total number of infections reported from 2012 through 2016), Arkansas (12.9%), Virginia (7.9%), upstate New York (7.6%), Oklahoma (6.4%), North Carolina (5.8%), Tennessee (5.6%), New Jersey (4.4%), Kansas (4.0%), and Kentucky (3.7%) (Fig. 2A). The current distribution of the lone star tick, which is the primary vector of E. chaffeensis, overlaps broadly with the distribution of reported infections, and the lone star tick will likely continue to expand its range (Yabsley 2010). The seasonal distribution of onset of infections was concentrated in July (22.0%), June (20.3%), August (16.0%), December (9.8%), September (9.3%), and May (9.2%) (Fig. 2B). Survival and activity levels of off-host (host-seeking) life stages of lone star ticks depend largely on weather conditions, including humidity and temperature, and availability of nonhuman hosts (Wang et al. 2012, 2015, 2016). Thus, not surprisingly, the seasonal distribution of infections largely reflects the coincidence of months of high host-seeking activity levels of ticks (see figure 4 in Wang et al. 2015) with months of relatively high outdoor activity levels of humans.
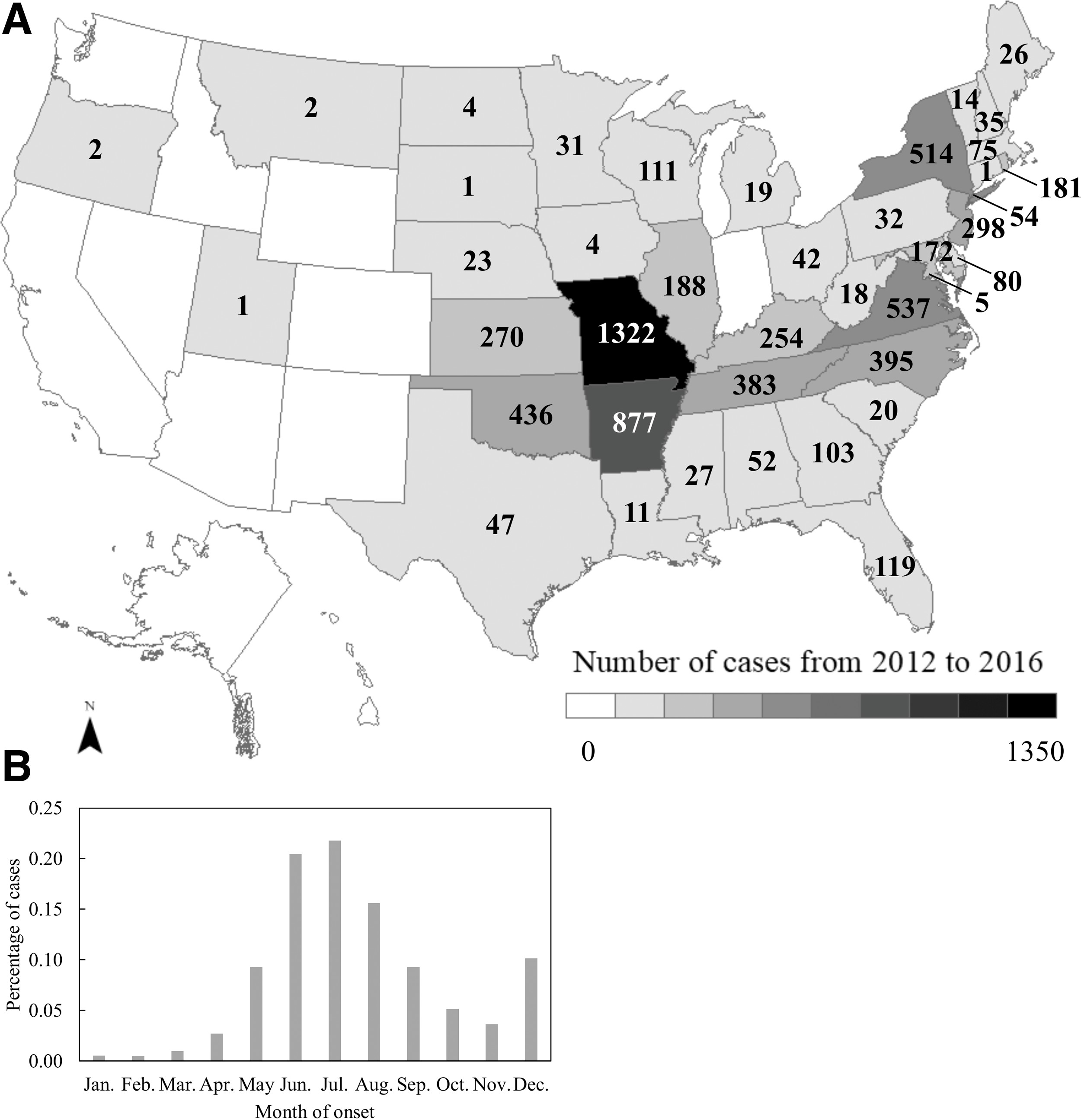
Spatial
Effective treatment of E. chaffeensis infections is readily available, and emphasis should be placed on conducting diagnostic tests on individuals prone to tick-borne infections. Since antibodies are not present early in the illness, serologic tests are useful for comparing acute and convalescent titers to document seroconversion. During the acute stage, molecular diagnosis and detection of E. chaffeensis DNA by PCR provide an effective diagnostic approach (Ismail et al. 2010). Unfortunately, symptoms characteristic of E. chaffeensis infections are common to many illnesses, and it is unlikely that a physician would test for the disease during early stages of infection unless a tick-borne infection was already suspected. Thus, ongoing surveillance and reporting of E. chaffeensis infections remain essential to inform public health practice and guide disease treatment and prevention efforts (Heitman et al. 2016).
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Acknowledgments
The study was supported by the Aggie Research Scholars Program and Aggie Research Leadership Program at Texas A&M University.
Funding Information
No funding was received for this article.