
Abstract
Anaplasmosis is a tick-borne disease that is primarily caused by the rickettsial bacterium Anaplasma phagocytophilum. Anaplasmosis is a febrile disease with common symptoms, including headaches, fever, and lethargy, but it can cause serious organ failure and even death if left untreated. Human infections are reported annually to the Centers for Disease Control and Prevention (CDC) through the National Notifiable Diseases Surveillance System (NNDSS). This report analyzed the cases of anaplasmosis reported by the NNDSS from 2012 to 2016. In total, there were 15,778 reported A. phagocytophilum infections, and the incidence rate was 7.27 cases per million persons per year, with the number of reported cases increasing each year. The demographic group most affected was middle-aged and elderly white males. Infections were most abundant in the coastal northeast and northern midwest regions. Our study provides useful results for a basic understanding of incidence, distribution, and severity of A. phagocytophilum infections.
Introduction
Contraction of anaplasmosis occurs most commonly when a mammal is fed upon for an extended period of time by an Ixodes scapularis (black-legged tick) that is infected with Anaplasma phagocytophilum, a gram-negative rickettsial bacterium (Rymaszewska and Grenda 2008). Prevention of anaplasmosis is only possible through avoidance of tick bites and prompt removal of attached ticks (Bakken and Dumler 2008), but treatment is possible by administering doxycycline to those who are infected (Wormser et al. 2006). In some cases, the immune system may be able to defend the body from the infection without the use of antibiotics, but if the immune system fails and the infection is left untreated, organ failure may occur and potentially, but rarely, lead to death (Brown 2012). A. phagocytophilum is somewhat unique in that it infects neutrophils (Sukumaran et al. 2005); thus, anaplasmosis can also be transmitted using a blood transfusion if the bacteria are present in the donor (Sukumaran et al. 2005).
In this study, we summarize the passive surveillance data on A. phagocytophilum infections reported to the Centers for Disease Control and Prevention (CDC) from 2012 to 2016 to increase awareness of recent anaplasmosis infection trends and to analyze these patterns. Specifically, we compare the number of cases reported annually from 2012 to 2016 with the number of cases reported during the previous 4 years (from 2008 to 2011). We also characterize the epidemiology of reported cases, including demographic profiles, incidence rates (IRs), and the spatial-temporal patterns of infections.
Materials and Methods
National Surveillance Systems
Individual states and territory health departments use the National Notifiable Diseases Surveillance System (NNDSS) to report surveillance data to the CDC using manually-completed Tick-Borne Rickettsial Disease Case Report Forms (CRFs) (
Case definition
A confirmed case of anaplasmosis has clinical evidence and confirmatory laboratory evidence; an undetermined ehrlichiosis/anaplasmosis case has clinical evidence, but only supportive laboratory evidence (Dahlgren et al. 2015). In general, there are several common fever-like symptoms found during the first week of clinical disease, making it difficult to diagnose as a rickettsial disease in early stages of infection (Biggs et al. 2016). Thrombocytopenia and leukopenia are usually observed (Dumler et al. 2005). Anemia generally occurs, and blood may also be present in urine if in the later stages of infection (Ismail et al. 2010). Damage to the liver may also occur, causing hepatic transaminases to experience mild-to-moderate elevations (Guzman and Beidas 2019). The characteristic erythema migrans rash associated with Lyme disease has also been reported in some cases, but this is only because some individuals contract both anaplasmosis and Lyme disease, as Anaplasma bacteria have not been shown to cause this rash (Bakken and Dumler 2008). The main procedural tests used for diagnosis of anaplasmosis are polymerase chain reaction, indirect immunofluorescence assay, and identifying the presence of intracellular morulae in stained blood smears (Jereb et al. 2012).
Analysis
Cases reported from January 2012 through December 2016 were included in the analysis. If the date of onset was not reported, the earliest known date associated with that particular case was used to represent that infection. IRs were calculated by year, state, and age, using U.S. Census Bureau population estimates. IRs were not reported for all race and ethnic groups because a large proportion of cases were missing these data. State populations were only considered at risk during the years in which anaplasmosis was reportable. The geographic distribution of total number of infections reported from 2012 to 2016 was summarized. This report does not include confidence intervals or results from statistical hypothesis testing since reported cases cannot be generalized to unreported cases or to other reporting time periods (Dahlgren et al. 2011, 2015, Mogg et al. 2020).
Results and Discussion
From the NNDSS, a total of 15,778 new cases of A. phagocytophilum infection were reported from 2012 to 2016. The mean IR during this period was 7.27 cases per million PY. The number (%) of confirmed anaplasmosis cases increased from 2012 to 2016, with 2,389 cases (92.60%) in 2012, 2,782 cases (92.67%) in 2013, 2,800 cases (93.46%) in 2014, 3,656 cases (95.33%) in 2015, and 4,151 cases (95.40%) in 2016. It is worth noting that the number of cases reported from 2012 to 2016 increased each year, and each year was higher than the number reported within the United States in any of the previous 4 years (Dahlgren et al. 2015) (Fig. 1). The number (%) of undetermined ehrlichiosis/anaplasmosis cases decreased from 2012 to 2016, with 191 cases (7.40%) in 2012, 220 cases (7.33%) in 2013, 196 cases (6.54%) in 2014, 179 cases (4.67%) in 2015, and 200 cases (4.60%) in 2016.
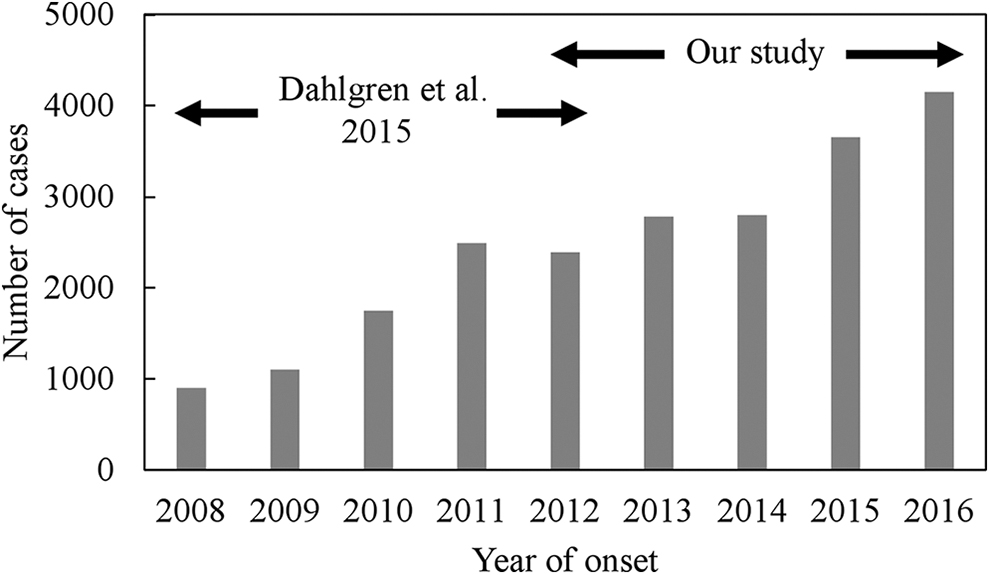
Number of cases of Anaplasma phagocytophilum infections reported annually in the United States from 2008 to 2016. Data from 2008 to 2012 are from Dahlgren et al. (2015), and data from 2012 to 2016 are from the Nationally Notifiable Diseases Surveillance System.
The primary demographic group affected by A. phagocytophilum infection was elderly white males (Table 1). More infections were reported in males (53.2%; IRs = 11.16) than in females (43.7%; IRs = 4.50), in whites (65.2%; IRs = 8.62) than in other races, and in individuals 40 to 64 years old (43.6%; IRs = 13.82) and over 65 years old (35.5%; IRs = 25.26) than in other age groups. The majority of reported infections were among non-Hispanics (60.6%; IRs = 7.62), although ethnicity was unknown in many cases (38.2%). These infection patterns likely result from socioeconomic levels and human activities (Kilpatrick and Randolph 2012), as well as age-specific physiological differences (Jin et al. 2012). Generally, outdoor recreational opportunities associated with wealth can result in increased exposure to vectors (Kilpatrick and Randolph 2012). Thus, white males may be more likely to spend time outside in areas where ticks are abundant, with middle-aged and elderly individuals more susceptible to infection than younger (18- to 40-year old) individuals with stronger immune systems. In addition, even though the immune systems of infants are less developed, infection rates are extremely low because this age group is unlikely to be in an environment where they are exposed to ticks (Bolgiano and Sexton 2018). Of course, these results also reflect an inherent reporting bias due to the unequal access to health care among demographic groups (Jones et al. 2012).
Demographic Profiles of Anaplasma phagocytophilum Infection Cases from 2012 to 2016 in the United States
The number of incidence cases is from the Nationally Notifiable Diseases Surveillance System, and the cases per million persons at risk (IRs) are calculated based on data from the Nationally Notifiable Diseases Surveillance System and the U.S. Census Bureau.
IRs, incidence rates.
The geographic distribution of A. phagocytophilum infections was concentrated in Minnesota (18.5% of the total number of infections reported from 2012 to 2016), Wisconsin (18.5%), Massachusetts (18.2%), upstate New York (16.8%), Maine (5.7%), Connecticut (3.6%), New Jersey (3.3%), Rhode Island (3.2%), Vermont (2.9%), and New Hampshire (2.8%) (Fig. 2A). The current distribution of I. scapularis, which is the primary vector of A. phagocytophilum, overlaps with the distribution of reported infections (Stuen et al. 2013). This distribution covers a large portion of the United States, with nearly the entire eastern half of the country being home to this tick (Brownstein et al. 2003). However, anaplasmosis infection is present within a much more limited geographic range, which leads to speculation that there must be environmental factors that affect transmission of the bacteria (Doudier et al. 2010). The seasonal distribution of onset of infections was concentrated in June (23.4%), July (22.2%), August (12.0%), and May (10.4%) (Fig. 2B). Survival and activity levels of off-host (host-seeking) life stages of I. scapularis depend on microclimate conditions, and abundances fluctuate seasonally depending on the availability of hosts (Mount et al. 1997). Thus, not surprisingly, the seasonal distribution of infections largely reflects the coincidence of months of high host-seeking activity levels of ticks with months of relatively high outdoor activity levels of humans (Kilpatrick and Randolph 2012).

Spatial
Of course, our findings are subject to the limitations of passive surveillance data. A. phagocytophilum infections are likely underrepresented because of the severity of illness, the level of endemic disease, and the resources available to clinicians and public health authorities as we described earlier (Dahlgren et al. 2015). For example, less severe cases may be less likely to obtain laboratory testing, and health care providers in low endemic areas may not be accustomed to treating anaplasmosis empirically without ordering laboratory tests. Thus, results from passive surveillance data cannot be generalized to unreported cases, and we cannot estimate how accurately surveillance reflects the underlying trends of A. phagocytophilum infections (Dahlgren et al. 2015). Nonetheless, our results provide a useful indicator of the general incidence, distribution, and severity of A. phagocytophilum infections.
Conclusions and Clinical Significance
This study has shown that anaplasmosis infection rates are increasing in the United States and are likely to continue increasing unless additional public health measures are exerted to increase awareness and decrease exposure. Reporting and surveillance data are invaluable to local and international public health organizations, but more importantly to the safety of the public itself. If not properly addressed by public health officials, anaplasmosis could become as widespread and damaging as Lyme disease is currently in the United States. The black-legged tick, which has become widely known for its ability to transmit the bacterium which causes Lyme disease, should also be noted for its ability to transmit the bacteria, which cause babesiosis and anaplasmosis (Eisen and Eisen 2018).
Effective treatment of A. phagocytophilum infections is readily available, and emphasis should be placed on conducting diagnostic tests on individuals prone to tick-borne infections. Unfortunately, symptoms characteristic of A. phagocytophilum infections are common to many illnesses, and it is unlikely that a physician would test for the disease during early stages of infection unless a tick-borne infection was already suspected. Thus, ongoing surveillance and reporting of A. phagocytophilum infections remain essential and useful to inform public health practice and guide disease treatment and prevention efforts (Heitman et al. 2016).
Footnotes
Acknowledgments
The study was supported by the Aggie Research Scholars Program and Aggie Research Leadership Program at Texas A&M University.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.