
Abstract
Toxoplasma gondii is a globally distributed protozoan that mainly causes health issues in the fetuses of pregnant women who have never been exposed to this parasite and patients with deficient immune systems. Except in these vulnerable populations, the primary infection generally goes unnoticed in most healthy individuals. Apart from transplant/transfusion, congenital transmission, direct contact with infected cats or their feces, and environmental contamination (i.e., oocysts in food, water, and soil) pathways, humans can acquire the parasite through consumption of animal tissues infected by T. gondii. This meta-analysis estimated the risk of acquiring T. gondii by consuming raw or undercooked meat, regardless of which animal species are eaten. Using a random-effect model, crude and adjusted pooled measures of association (risk and odds ratio) were estimated according to study design (cohort, case–control, and cross-sectional studies). The meta-analysis included measures of heterogeneity as well as quality rating scales for each study design. Our results suggest that individuals who eat raw or undercooked meat have, respectively, 1.2–1.3 times the risk and 1.7–3.0 times the odds of T. gondii infection compared to those who thoroughly cook meat, regardless of the animal species they consume. These results align with the current understanding that adequately cooking meat inactivates the parasite and decreases the risk of transmission. Seroprevalence ranged from 1.3% to 88.6%, while the proportion of individuals eating raw or undercooked meat fluctuated from 0.7% to 98.3% across the studies in the meta-analysis. These numbers reflect various preferences with regard to eating meat (i.e., eating tartar, sausages, or salamis) as well as individual, cultural and religious food habits, and personal awareness.
Introduction
Rationale
Approximately 30
Three life cycle stages of the T. gondii are infectious to humans: (1) sporozoites contained in oocysts shed by domestic or wild felids, the only known definitive hosts of the protozoon; (2) tachyzoites in the rapidly multiplying stage encountered during the acute phase of a primary infection in intermediate hosts (humans and animals); and (3) bradyzoites in latent tissue cysts within intermediate hosts (Dubey 2010). Humans can acquire the parasite through four main pathways: medical intervention (e.g., organ transplantation or blood transfusion), mother to fetus (congenital), and by ingestion of oocysts or consumption of animal-infected tissues (cysts) (Montoya and Lisenfield 2004). Ingestion of oocysts happens either directly by contact with felids or their stools or indirectly through environmental contamination (e.g., sandbox, gardens, cat litter, water, or fresh produce such as vegetables or fruits) (Dubey 1998, Jones and Dubey 2010). As for animals, most domestic or wild species are potential carriers of T. gondii (Dubey 2010). Most public health agencies promote strategies to inactivate the parasite in meat (by cooking and freezing) or to decrease the risk of acquiring it through manipulation of meat (e.g., washing hands, wearing gloves, not tasting meat while cooking, and so on) (Dubey et al. 1990, Kijlstra and Jongert 2008, Herrero et al. 2017). Not all individuals and cultures practice these strategies, however, as some prefer their meat undercooked or raw. European culinary culture includes steak tartar, for example, and Arctic Inuit communities prefer raw or aged meat (Blanchet and Rochette 2008).
Objective
The objective of this systematic literature review is to estimate the probability of being exposed to T. gondii by raw or undercooked meat consumption, regardless of animal species.
Methodology
Information sources, search strategy, and eligibility criteria
This study followed the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelines (Moher et al. 2015). No publication period was imposed and the literature search was last updated on February 6, 2020. Articles in languages other than English, French, Spanish, and Portuguese were excluded. Supplementary Table S1 describes the search strategies used for each bibliographic database. Exposure was defined as eating raw or undercooked meat, and outcome refers to the presence of antibodies against T. gondii. Meat was defined as muscular tissue from an animal (terrestrial or aquatic mammals or birds) or meat byproducts (e.g., sausages).
Data management
All references were imported directly to Endnote X8 software; duplicates were eliminated, and the final citations were exported into Excel software. Titles and abstracts were screened by two independent reviewers and classified as eligible (1), noneligible (0) or uncertain (?). An agreement value of 89.1% was reached and discrepancies were resolved by consensus after publications were further scrutinized for eligibility.
Selection process
A total of 3023 publications were identified, of which 779 duplicates and 1754 studies that, based on their abstract, did not cover risk factors associated with T. gondii were excluded (Supplementary Fig. S1). Then, combined with 18 additional studies found by examining other systematic reviews, 570 publications were reviewed to assess their eligibility. Data from 197 retained publications were extracted. As 18 of these publications presented 2 or more measures of effect (resulting from separate multivariate analysis for each population or study design), a database with 215 entries was obtained (Supplementary Fig. S1). The randomized trial portion from Desmont et al. (1965) was excluded from the meta-analysis based on ethical concerns and deficient methodology, while the data from the cross-sectional portion were maintained (Vergnes et al. 2010). Four additional studies were excluded from the meta-analysis because of null values that impeded the calculation of a measure of association. The final database contained 210 entries (Supplementary Fig. S1).
Data extraction
The following variables were extracted: first author's last name, year of publication, study design, country, seroprevalence, sample size, number of women and men, age, diagnostic tests, antibodies measured, type of statistical analysis,
Quality of studies and bias
The quality of studies was evaluated using a Newcastle-Ottawa Scale for each study design, containing specific criteria about selection of individuals, exposure, and outcome. The maximum points granted was nine, which represents the highest quality and lowest bias (Wells et al. 2019). The scale was customized for comparability criteria for a maximum of two points. One point was attributed if (1) multivariable regression models adjusted for a sociodemographic variable (age, gender, education, socioeconomic status, or residential area) as they can reflect unmeasured exposure to the parasite or knowledge of hygiene measures (Cutler and Lleras-Muney 2010); and (2) if authors controlled for other source of exposure to T. gondii other than raw meat. These other sources of exposure were regrouped as (1) having contacts with cats; (2) being exposed to soil; (3) consumption of unwashed fruits and vegetables; (4) traveling or eating outside the home; (5) occupational risk; and (6) medical interventions. In the absence of a validated questionnaire, two points were attributed if a pretesting phase or standardization occurred and one point was added if the questionnaire was available.
Statistical methods
Four pooled measures of associations were calculated: crude odds ratio (OR), prevalence ratio (PR), incidence ratio (IR), and adjusted odds ratio (aOR). All measures of association were transformed on the natural logarithmic scale to conserve symmetry during the analysis (Borenstein et al. 2009). Standard error of log-transformed measures were calculated using 95% confidence intervals (CIs) or with the variance, and measures of effect were converted back to their original scale. Random-effect computational models were used based on the assumption that studies would reflect variability in the force of association; T. gondii prevalence and parasite burden vary between animal species, concentration of cats in the environment and geographical areas (Belluco et al. 2016). The study-weights were based on the inverse of the within-study variance
Heterogeneity was evaluated with the observed variation between studies that reflects a real difference in effect size (
Results
Characteristics of eligible publications
All 210 entries retained were observational studies published from 1965 to 2019; most were cross-sectional (n = 196), followed by case–control (n = 11) and cohort (n = 3) (Supplementary Table S2). All studies included in the meta-analysis are referenced in the Supplementary Material. The T. gondii antibody seroprevalences reported ranged from 1.3% to 98.4%, while the proportion of those eating raw meat varied from 4.4% to 86.5%. The publications spanned 64 countries with the exception of 1 multicenter case–control study design based in 6 large European cities. The number of participants in the studies included in the meta-analysis ranged from 23 to 4436 individuals, while age of the participants varied from 6 months to 60 years.
Measures of effect between eating raw or undercooked meat and past exposure to T. gondii
The three prospective cohorts that measured incident cases included a total of 1218 individuals. The OR of 2.0 (95% CI; 0.7 to 5.8) overestimated the true association in a context of high seroprevalence such as with T. gondii compared to the IR of 1.3 (95% CI; 1.0 to 1.6) (Table 1 and Supplementary Figs. S2 and S3). The proportion of individuals eating raw or undercooked meat ranged from 8.6% to 41.9%, while the reported prevalence of antibodies against T. gondii varied from 6.2% to 67.1%.
Pooled Measures of Effect According to Study Design
All numbers highlighted in bold correspond to the pooled measure of effect.
For cohorts, the odds ratio are presented only for comparison purposes with the other study designs since they represent a biased estimation of the true effect in the context of Toxoplasma gondii seroprevalence above 10% (odds ratio can approximate the risk ratios only in the presence of the “rare disease assumption”). For this reason, only heterogeneity measures of the risk ratios are presented.
CI, confidence interval.
The 10 case–control studies providing data to estimate a pooled crude measure of effect encompassed 4438 individuals and yielded an OR of 3.0 (95% CI; 2.1 to 4.3), while the 7 case–control studies retained to estimate an adjusted pooled measure yielded an aOR of 2.9 (95% CI; 1.6 to 5.2) and included 2426 individuals (Table 1). All point-estimates of OR observed in these case–controls were above the null value (Fig. 1 and Supplementary Fig. S4). These studies targeted high-risk individuals, either patients with acute toxoplasmosis or pregnant woman with recent seroconversion. The proportion of individuals consuming raw or undercooked meat varied from 6.6% to 57.4% and prevalence of T. gondii antibodies in the study and reported by authors ranged from 6.3% to 74.5%.

Forest plota of case–control studies included in the estimation of the pooled aOR measuring the association between Toxoplasma gondii seroprevalence and eating raw or undercooked meat. aInterpretation of a forest plot: each gray box reflects the measure of association (aOR) in the study with its 95% confidence intervals represented by the black lines on each side whereas the size of the box reflects the weight of each study. The thick black line traversing the graphic from top to bottom represents the pooled aOR with the 95% confidence intervals depicted by the width of the diamond shape at the bottom of the graph. aOR, adjusted odds ratio.
Of all the cross-sectional entries, three pooled measures of effect were estimated: an OR of 1.6 (95% CI; 1.4 to 1.7), a PR of 1.2 (95% CI; 1.2 to 1.3), and an aOR of 1.7 (95% CI; 1.5 to 1.9) (Table 1). The forest plot for the aOR is presented in Fig. 2, and the others are available in Supplementary Figs S5 and S6. The number of individuals involved in the cross-sectional studies varied according to the estimated measures of effect (Table 1). The proportion of participants eating raw or undercooked meat ranged from 0.7% to 98.3%, while seroprevalence of antibodies against T. gondii varied from 1.3% to 88.6%.
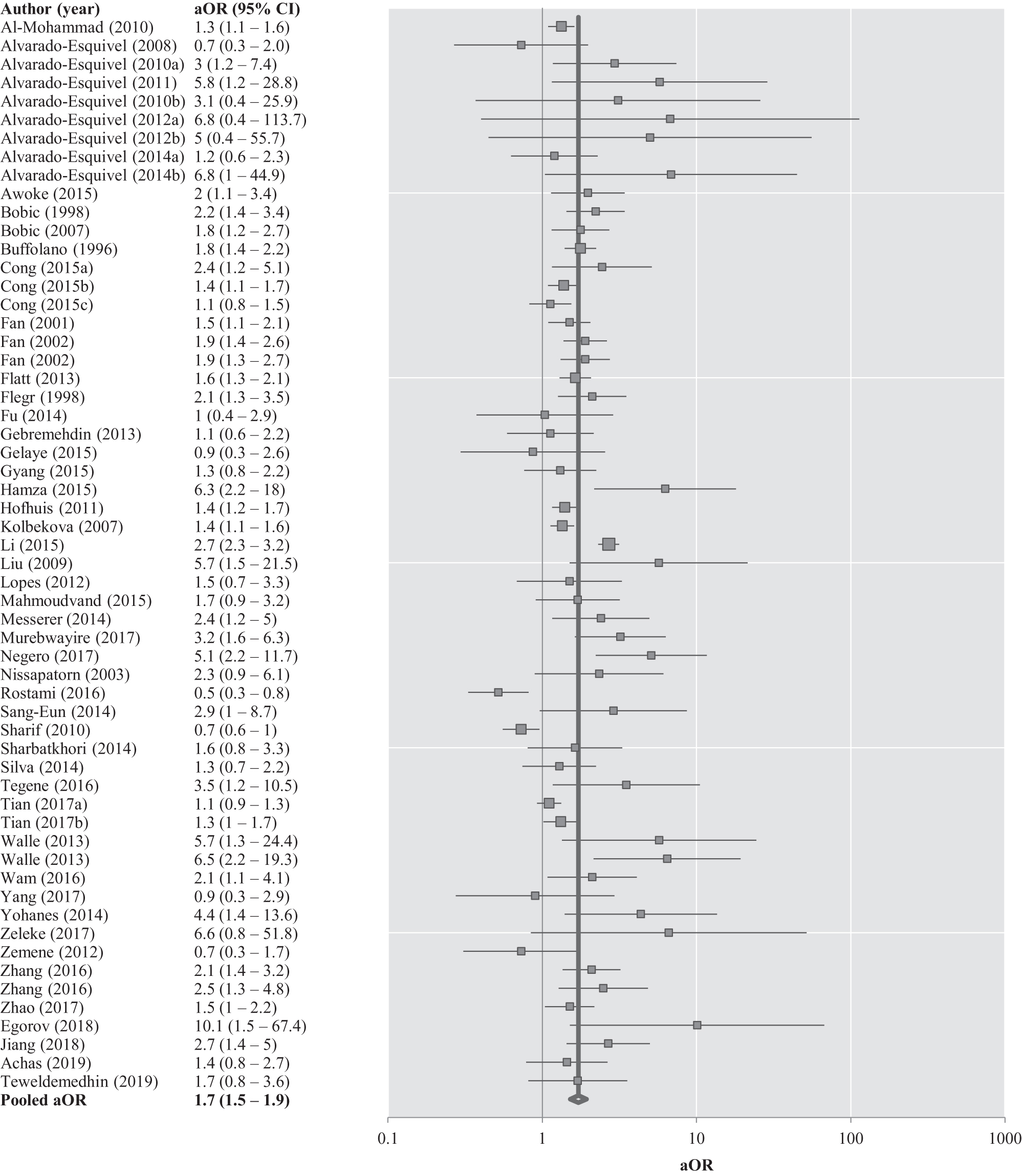
Forest plota of cross-sectional studies included in the estimation of the pooled aOR measuring the association between T. gondii seroprevalence and eating raw or undercooked meat. aInterpretation of a forest plot: Each gray box reflects the measure of association (aOR) in the study with its 95% confidence intervals represented by the black lines on each side whereas the size of the box reflects the weight of each study. The thick black line traversing the graphic from top to bottom represents the pooled aOR with the 95% confidence intervals depicted by the width of the diamond shape at the bottom of the graph.
None of the pooled measure of effect varied according to the quality score, climatic zone, human development index, serological test, or the type of immunoglobulins detected (results not shown). None of the exclusion sensitivity assessment yielded pooled measures of effect that changed the direction and strengths of the associations.
Heterogeneity bias
The within-study error (
Quality of studies
On a scale of nine points, cohorts ranked from six to seven points; case–controls ranked from zero to eight points (for crude measure) and from six to eight points (for adjusted measures), while cross-sectional studies ranked from one to seven points (crude measure) and from four to seven (adjusted measure) (Table 2). More detailed explanations of the quality of the studies are available in the Supplementary Data.
Evaluation of Quality of Publications According to Study Design
Sociodemographic variable (e.g., age, gender, education, socioeconomic status or residential area).
SD, sociodemographic variable.
Discussion
To our knowledge, this is the first systematic review and meta-analysis of the association between T. gondii past exposure and eating raw or undercooked meat, regardless of the animal species consumed. Our meta-analysis suggests that individuals who eat raw or undercooked meat have higher risks and odds of having antibodies against T. gondii, compared to those who thoroughly cook meat. These results align with the current understanding that adequately cooking meat leads to a decreased risk of transmission (Dubey 2000, Kijlstra and Jongert 2008, Herrero et al. 2017). Our results also align with the findings of another meta-analysis that used only case–control studies, which estimated the same type of association by animal species. Belluco et al. (2016) obtained an overall pooled OR of 3.4 (95% CI; 1.3 to 9.2) for consumption of raw or undercooked meat compared to well-cooked meat (2.2 for beef and of 3.9 for sheep).
The proportion of individuals who eat raw or undercooked meat fluctuated across studies and reflects various preferences of how to consume meat (e.g., as tartar, sausages or salamis) according to individual, cultural or religious food habits, and personal awareness (Buffolano et al. 1996, Kapperud et al. 1996, Bobic et al. 1998, Baril et al. 1999, Roghmann et al. 1999). These expected variations are reflected in the heterogeneity measures, demonstrating a wide dispersion of associations in the forest plots.
For our purposes, participants were dichotomized as eating raw or undercooked meat or not, which represents a crude assessment of exposure. Different recall periods and varying frequency of the consumption of raw or undercooked meat between studies impeded the use of a finer scale to measure exposure. The few studies that defined the terms “well-cooked,” “raw,” or “undercooked” meat usually referred to the color and/or the presence of blood in meat. Even when individuals are aware of possible foodborne illnesses in undercooked meat, few use a thermometer to assess the temperature of the middle of the piece of meat (Murray et al. 2017). Hence, a superior ratio of misclassification of exposure in our control group is expected compared to the exposed (eating raw or undercooked meat), which suggests that our pooled measures of association underestimate the true effect.
Evaluating past or recent exposure to T. gondii with antibody titers was preferred since serological testing serves as initial screening in most studies. These tests display higher sensitivity and specificity values for past exposure than molecular techniques to diagnose acute toxoplasmosis, its progressions, and the treatment efficacy (Liu et al. 2015). However, serology lacks information about the moment individuals were first exposed to the parasite (temporality). Typically, following a primary T. gondii infection, IgM will first rise, followed by IgG in the first to third weeks postinfection (Fricker-Hidalgo et al. 2013). IgM and IgG are most frequently measured compared to the other markers (i.e., IgA and IgE or IgG with avidity testing). However, atypical seroconversion patterns have been occasionally observed, which suggests that misclassification can occur (Fricker-Hidalgo et al. 2013). Different serological tests were used between studies; mostly enzyme immune-assay (68%) followed by agglutination (16%), fluorescent antibody (13%), Sabin–Feldman dye (3%), and skin antigen (1%) tests. Only rarely did studies provide information on sensitivity and specificity of their serological test. Therefore, it was not possible to validate their level of accuracy or the direction and strength of this potential information bias.
The main strength of this meta-analysis is that it includes all types of study design that evaluate the association between eating raw or undercooked meat and T. gondii infection. Crude or adjusted pooled measures of effect for each study design are consistently above the null value, indicating that eating raw or undercooked meat increased the probabilities of having antibodies against T. gondii. The adjusted measures of effect decrease the potential confounding bias and increase the validity of results compared to crude measures (Mickey and Greenland 1989).
Our meta-analysis also has limitations. First, many studies did not include the “eating raw or undercooked meat” variable in their multivariate analyses, leading to a potential selection bias when estimating the pooled adjusted measures of effect (Meireles et al. 2015). This type of bias was mainly observed with cross-sectional designs. The estimation of a pooled OR also overestimates the strengths of the association in the context of a disease of high seroprevalence such as T. gondii, and relative risks should be preferred when interpreting the results (Mickey and Greenland 1989). A few studies had significant associations with 95% CIs below the null value, indicating a lower seroprevalence in the exposed (eating raw or undercooked meat) compared to the control group. This suggests the presence of uncontrolled confounding or of random variability (Egger et al. 1998). These cross-sectional studies have potentially biased the pooled measures toward the null values, but the extent of this effect remains unknown. Finally, the different quality scales used to evaluate the studies did not capture all the features of internal and external validity—namely, information on validation of regression model postulates such as linearity, independence between subjects, collinearity, and extreme data. Violation of these assumptions can also bias the interpretation of the measure of association (Vittinghoff et al. 2005). Some studies may have ignored collinearity between variables, a reality that often occurs in nutritional epidemiology when collecting information about multiple food items (Elmsthal and Gullberg 1997).
Conclusion
The consistency of the estimates of measures of effect above the null value across all study designs suggests that eating raw or undercooked meat is frequently linked to the presence of antibodies against T. gondii. Our study supports the notion that more individuals who eat raw or undercooked meat have antibodies against T. gondii than those who thoroughly cook meat, regardless of what animal they consume. These pooled measures of association are believed to reflect that eating raw or undercooked meat contributes to exposing humans to T. gondii, despite the presence of limitations associated with this meta-analysis.
Support
The methodology follows the PRISMA-P 2015 (Moher et al. 2015). Details of the protocol have been registered on PROSPERO (No. CRD42015029253) and can be accessed at (
Authors' Contributions
J.D. and A.S. have elaborated the protocol, performed the systematic review, extracted, and analyzed the data. J.D. wrote the article, and all others have revised the text and made comments. The first author conducted this systematic review as a requisite for a doctoral course.
Footnotes
Acknowledgments
We thank Jacques Brisson and Hervé Tchala Vignon Zomahoun from Université Laval (Québec, Canada) for their ongoing support and feedback throughout the progress of this article. Many thanks also to Myrto Mondor and Elhadji Anassour Sidi for their guidance as biostatisticians and to Sara Carazo for her review of Spanish, Portuguese, and Italian articles. In addition, we offer a warm welcome to the following authors who generously wrote back with additional information about their studies: Digsu Negese, Abeer Mahgoub, Dominika Salamon, Olgica Djurkovic-Djakovic, Edwin Ogendi and Jorge Enrique Gomez Marin.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
Financial support was provided by the Fond de recherche du Québec—Santé, ArcticNet and the Nasivvik Research Chair in Ecosystemic Approach to Northern Health.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.