
Abstract
Purpose:
Lyme borreliosis (LB) occurs throughout Europe. No clinical and seroprevalence studies for LB in Kosovo have been publicly available thus far. Therefore, this study aimed to investigate LB from a tick bite perspective in the Pristina region, Kosovo.
Methods:
This single-center prospective observational study enrolled consecutive adult participants (≥18 years of age) with tick bite (embedded tick in the skin), who were examined at the Clinic of Infectious Diseases, Pristina, between January 2015 and August 2018. At the first visit related to the index tick bite, ticks (the complete ticks or parts of the ticks) were removed from the skin, blood samples were taken for serological tests, and antibiotic treatment was started when deemed necessary. The complete, undamaged ticks removed were proceeded for entomological identification. Participants were followed up at 2 months (serological tests were repeated) and 6 months after the index event for the development of clinical manifestations of LB and/or seroconversion against Borrelia burgdorferi.
Results:
A total of 380 subjects were included in the study. Most cases were seen in May and June in all study years. All 117 preserved ticks were identified as Ixodes ricinus. Immunoglobulin G seroprevalence among subjects during the first visit in the study was 28/380 (7.4%). Erythema migrans (EM) was clinically diagnosed in 74/380 patients (19.5%, 95% confidence interval 15.6–23.8). Only 15 clinically diagnosed EM (in seronegative patients) were serologically confirmed with seroconversion (2 months later), 3.9% of all subjects included in the study. There were three cases with clinical manifestation between the second and third visit: EM recidivans, multiple erythema, or several nonspecific systemic symptoms. Doxycycline and amoxicillin were mainly used for the treatment of borrelial skin lesions.
Conclusion:
This assessment can help indicate the need for disease awareness and reinforce the importance of primary prevention measures, early diagnosis, and appropriate treatment.
Introduction
Lyme borreliosis (LB) is the most common human vector-borne disease occurring in the northern hemisphere (Lindgren and Jaenson 2006, Dehnert et al. 2012, Steere et al. 2016, Stone et al. 2017). It is a potentially chronic multisystem disease caused by the spirochete Borrelia burgdorferi sensu lato and transmitted by hard ticks of the genus Ixodes (Stanek et al. 2012, Barrett and Portsmouth 2013, Stanek and Strle 2018). B. burgdorferi can attack various organs/systems such as skin, joints, nervous system, and heart (Weber 2001, Stanek et al. 2012, Stanek and Strle 2018). Erythema migrans (EM), which appears early in the course of the disease, is the most common clinical manifestation (Steere 2001, Stanek et al. 2012, Steere et al. 2016, Stanek and Strle 2018).
LB in Europe is a frequent disease with increasing incidence (Sykes and Makiello 2017, Stanek and Strle 2018). There are 65,000–85,000 estimated annual LB cases (Lindgren and Jaenson 2006, Barrett and Portsmouth 2013, Stone et al. 2017, Sykes and Makiello 2017, WHO 2017). The highest incidence of LB has been reported from Austria, Germany, Slovenia, and Sweden (Mehnert and Krause 2005, Fryland et al. 2011, Stanek et al. 2011, Dehnert et al. 2012, Esposito et al. 2013).
Epidemiological data pertaining to LB in the southern Balkans region and Kosovo in particular are scarce. Crimean–Congo hemorrhagic fever is a well-known emerging and life-threatening disease in this area (Sherifi et al. 2018, Ahmeti et al. 2019). However, little is known about the LB in Kosovo, and no clinical and seroprevalence studies have been publicly available thus far. On the other hand, the presence of Ixodidae ticks—the main vectors of LB in Europe—has been confirmed in Kosovo's natural environment as well (Sherifi et al. 2018). This study, therefore, aimed to investigate LB from a tick bite perspective in the Pristina region, Kosovo.
Materials and Methods
Study outline
This single-center prospective observational study enrolled consecutive adult participants (≥18 years of age) with tick bite (complete ticks embedded in the skin or parts of the ticks), who were examined at the Clinic of Infectious Diseases University Clinical Center of Kosovo, Pristina, between January 2015 and August 2018. The study was approved by the local Ethical Committee University Clinical Center of Kosovo (Protocol number:1578;17.04.2014), and all subjects provided signed informed consent.
At the first visit related to the index tick bite (index visit), subjects were evaluated clinically, ticks (the complete ticks or parts of the ticks) were removed from the skin, blood samples were taken for standard laboratory and serological tests, and antibiotic treatment was started when deemed indicated.
At visits scheduled at 2 and 6 months after the index visit, clinical evaluation and serological tests (at 2 months) were repeated and participants were followed up for the development of clinical manifestations of LB and/or seroconversion in seronegative patients. Seropositive participants in the initial visit were evaluated for the seroprevalence and followed up for clinical manifestations only.
Patient evaluation and follow-up
A special questionnaire was filled out during each visit. The first visit questionnaire contained the following: identification data of the participant (general, occupational, and contact information), the duration of tick(s) attachment, the history of prior tick bites, and current antibiotic treatment for other reasons. The second visit questionnaire contained: data on any new tick bites and the appearance of clinical manifestations since the first visit, and type and duration of antibiotic treatment. The third visit included data on any appearance of clinical manifestations.
At the index visit, complete ticks that were successfully removed from the skin without being damaged proceeded for entomological identification (School of Veterinary Medicine, University of Pristina). Participants were discharged and instructed to contact the researchers by phone or in person in the case of worsening of any of the symptoms or in the case of new-onset symptoms at any time during the subsequent 6-month period. During the second visit, scheduled 2 months after the index visit, detailed medical history, clinical evaluation, and blood sampling for serological testing were repeated. The third, that is, the follow-up visit, was scheduled at 6 months after the initial evaluation.
The list of clinical manifestations taken into account included the following: chills, fever, muscle and/or joint pain, headache, dizziness, neck pain, and fatigue; burning sensation and/or itching at the site of the bite; or clinical signs indicative of meningitis, meningo-radiculoneuritis, cranial neuritis-Bell's palsy, carditis, arthritis, borrelial lymphocytoma, EM, multiple erythema, and erythema recidivans. Criteria for the diagnosis of EM were in cases where the lesion appeared on the site of a tick bite (with interval of minimum 2 days after tick bite) and/or visible lesion on the site of tick bite is enlarging.
Serological analysis
Serological tests were performed to detect (potential) seroconversion using the enzyme-linked immunosorbent assay (ELISA) for immunoglobulin M (IgM)/immunoglobulin G (IgG) class antibodies against B. burgdorferi (NovaLisa Lyme Borrelia; NovaTec, Dietzenbach, Germany), for qualitative determination of IgM/IgG antibodies against B. burgdorferi in human serum or plasma using VlsE (recombinant), and lysate antigens of B. burgdorferi, B. afzelii, B. garinii, and B. flagellin (recombinant) and purified OspC as specific antigens. The sensitivity of the test is around 85% for specific IgM antibodies and >95% for specific IgG antibodies; specificity is 94% and 96.7%, respectively.
Statistical analysis
Data are summarized as percentages (proportions) or as means (standard deviations), or, where appropriate, median (quartiles). Where deemed of interest for estimation, proportions are reported with the exact Clopper-Pearson 95% confidence intervals. In an attempt to identify predictors (as assessed at the index visit) of the development of clinically manifested diseases, a multivariate modified Poisson regression model with robust sandwich estimation (to model relative risk) was fitted to the probability of the event. Data were analyzed using SAS 9.4 for Windows software (SAS, Inc., Cary, NC).
Results
Subjects
A total of 380 subjects with tick bites were included in the study, the majority of them in 2015 (n = 179) and fewer in 2017 and 2018 (n = 65 for the 2 years combined). Since the research site was located in Pristina, the largest municipality in Kosovo, the majority of participants were residents of the Pristina municipality. Nonetheless, participants were seen from different areas of Kosovo (all within a 100 km perimeter) (Fig. 1).
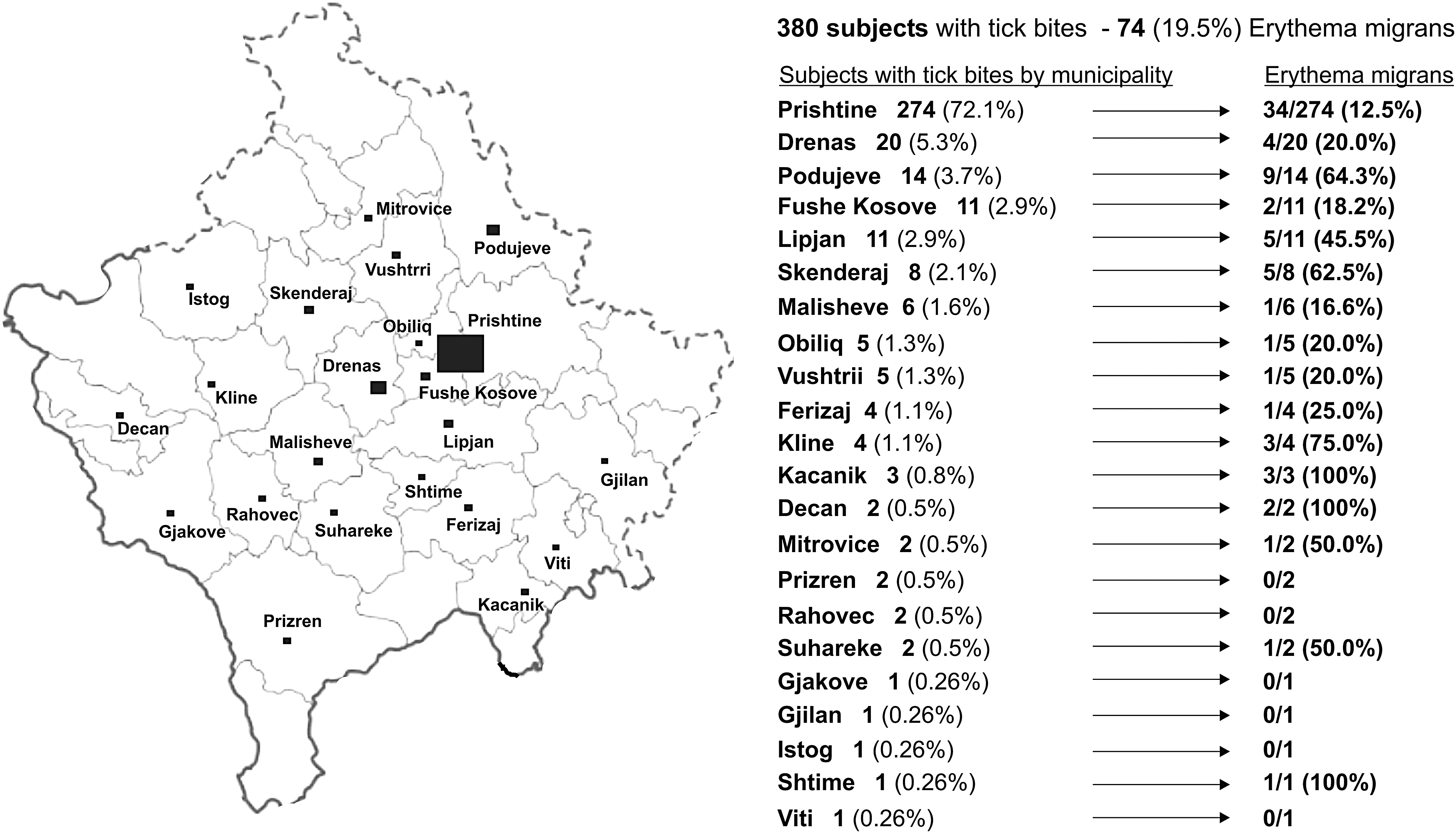
Geographical origin of the included patients. Larger squares indicated municipalities contributing more patients (actual counts and percentages provided). The research center was located in Pristina.
The majority of cases in all study years were observed during May and June (Table 1). The age range was wide (18–91 years), but patients were predominantly middle aged (median age 48 years) with a slight male predominance (Table 2). The majority of subjects (365, 96.0%) included in the study belonged to the general population in whom tick bites were related to recreational activities, with only 15 (3.9%) study participants bitten during professional activity. Close to half of them had previous experience with tick bites in the past, but without clinical signs in all but a few patients (Table 2).
Absolute Number of Enrolled Patients by Calendar Time (Part of a Year)
Subject Characteristics at the First Visit for the Index Tick Bite
Data are median (range) or count (percent).
IgG, immunoglobulin G; IgM, immunoglobulin M.
Observations at the first visit for the index tick bite
In half of the participants, the duration of tick attachment was uncertain, while most commonly, it was <24 h (Table 2). All 117 preserved ticks at removal (Table 2) were identified as Ixodes ricinus (adult females and nymphs). IgG seroprevalence among subjects during the first visit in the study was 28/380 (7.4%), with 17 male and 11 female. More than half of subjects (16/28; 57.1%) with IgG positive in the first visit declared previous tick bite. Only one participant with detectable IgG on the first and second visits reported possible early LB in the past.
During the first visit, 7 patients were already taking antibiotics, and antibiotics were prescribed to 69 (18.3%) patients (Table 2)—mostly amoxicillin based (to prevent superinfection) to those with manipulation during tick removal (patients who tried to remove the embedded tick by themselves and parts of tick remained in the skin)—while doxycycline was prescribed prophylactically in 12 patients after removing the engorged (swollen) tick.
Observations at the second visit
During the second visit (55–65 days after the first one), 377 subjects were seen: three were lost to follow-up (one died of prostatic cancer and the other two for unknown reasons) (Table 3). Overall, 13 subjects (3.5%) experienced at least one systemic symptom since the first visit—most commonly fatigue, joint pain, headache, fever, and chills (Table 3). Only seven patients experienced ≥2 systemic symptoms (Table 3). Burning and itching at the bite site were each reported by 15 (4.0%) subjects. EM was clinically observed in 74/380, that is, 19.5% (95% confidence interval [CI] 15.6–23.8) of all patients initially included in the study.
Subject Characteristics at the Second Visit for the Index Tick Bite (Three Dropouts; One Died of Prostate Carcinoma and Two Lost to Follow-Up), and at the Third Visit (Thirty-Eight Additional Lost to Follow-Up)
Data are count (percent).
It was evaluated that subjects who had developed ≥2 or more systemic symptoms or had local symptoms (itching and burning) (without EM), or had visible typical EM (Fig. 2) actually developed a clinically manifested disease: there were 76 such patients, that is, 20.0% (95% CI 16.1–24.4) of all subjects included in the study.
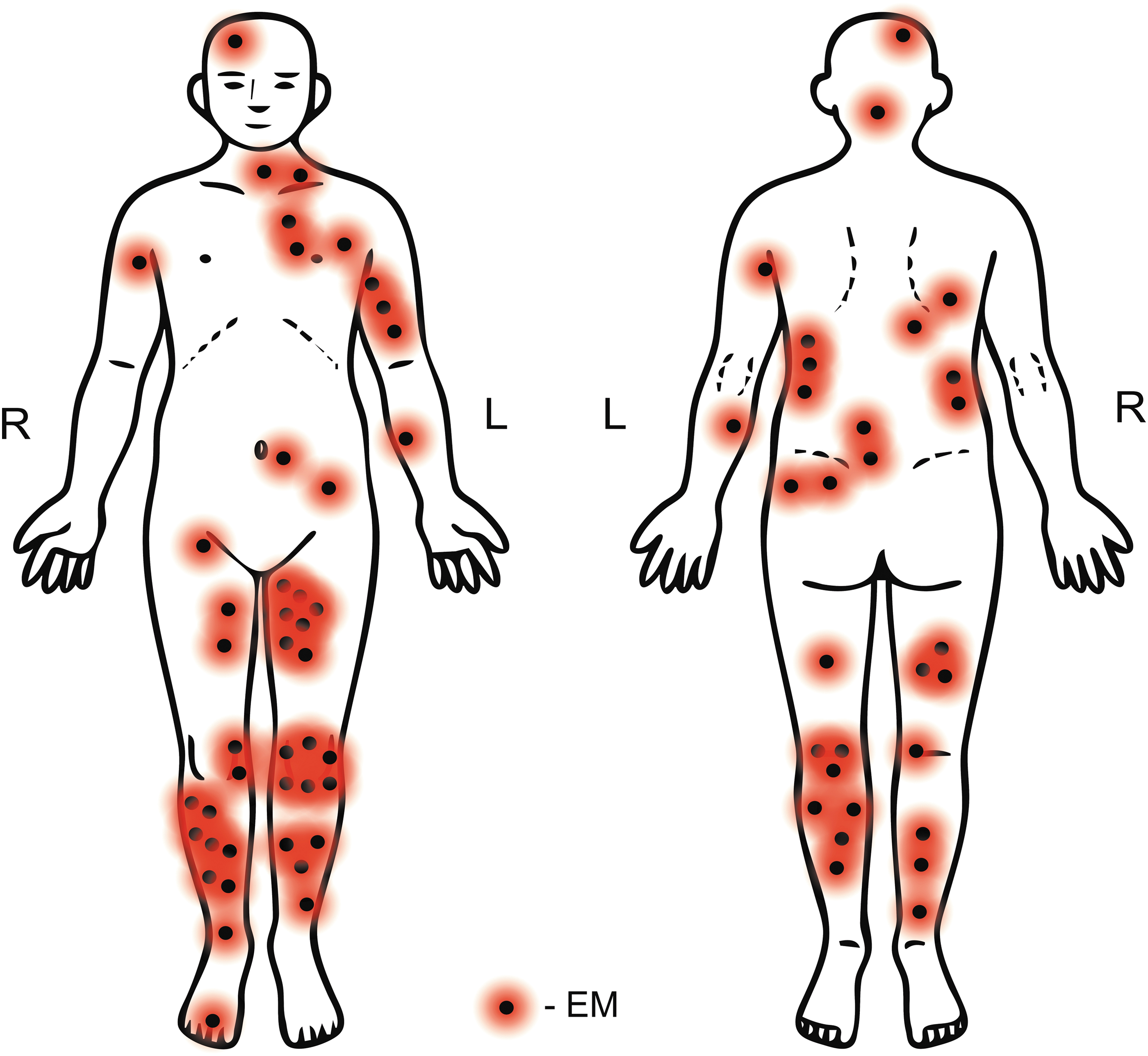
Schematic representation of the location of all observed cases of erythema migrans.
The number of patients with clinically diagnosed EM and positive ELISA test results (seroconversion) after 2 months was very low. Only 15 patients with clinically diagnosed EM (in seronegative patients) were serologically confirmed with seroconversion (2 months later), 3.9% of all subjects included in the study. While in 11 seropositive participants (for IgM or IgG) in the first visit clinical EM was also observed during the study, nine seronegative participants in the first visit developed seroconversion in the second visit (2 months after), without any clinical manifestation during the period of the 6-month follow-up.
Observations at the third visit (follow-up)
At 6 months after the initial visit, 339 subjects were seen (the rest were lost to follow-up): during this period, only three patients presented with clinical manifestation—one patient developed EM recidivans, one developed multiple erythema 3 months after the tick bite (with IgM positive in the second visit), and one patient experienced fatigue, arthralgia, palpitation, and dyspnea with a right bundle branch block 77 days after the tick bite (with seroconversion/IgM positive at the second visit) (Table 3).
Factors related to the development of a clinically manifested disease
Since only three subjects developed clinical manifestation between visits 2 and 3, and considering the extent of patient attrition between these two visits, findings at visit 2 were considered primary to evaluate factors related to the probability of developing any clinical form of the disease. Raw data indicated that this was more common in patients from locations other than Pristina (Fig. 1), likely due to confounding-by-indication. Patients examined from other locations were probably those who had experienced more severe local or systemic symptoms, while others (milder) were managed locally. Data also indicated an increasing trend over the observed years (Table 3).
Figure 3 tabulates the proportions of patients with a clinically manifested disease by location-by-removal of a preserved tick-by-duration of tick attachment-by antibiotic treatment: when the tick was preserved at removal, the risk was low, while it was considerable when this was not achieved—more so at other locations than in Pristina residents (Fig. 3). The risk appeared considerably lower when antibiotics were used (vs. no use) in patients in whom the tick was not preserved during removal, and evidently more so in patients from locations other than Pristina (Fig. 3). Antibiotic use seemingly did not affect the risk when the tick was preserved at removal (since the risk was anyhow low). The duration of tick attachment also did not appear to be associated with the development of a clinically manifested disease (Fig. 3).

Tabulation of patients with a clinically manifested disease with respect to geographical location by preservation of tick at removal, by the duration of tick attachment, and by prophylactic antibiotic use.
The multivariate analysis (Table 4), preservation of the tick at removal, early antibiotic treatment, and Pristina location were independently associated with a lower risk of developing a clinically manifested disease, while the risk in years 2017 and 2018 appeared higher than in 2015 (Table 4). Unfortunately, no interactions between these factors could be meaningfully tested due to cells with zero events/subjects (Fig. 3).
Summary of Multivariate Analysis of the Probability of Clinically Manifested Disease at Visit 2
A modified Poisson regression model with robust error variance was fitted to the probability of a manifested disease in which calendar year, tick preservation, use/prescription of antibiotics, and location were independents of primary interest, while age and sex were further adjustments.
Estimates and covariance from the fitted model were retained and used to adjust all estimates of the effects of primary interest and p-values for multiplicity (logical step-down with a simulation method).
RR, relative risk; CI, confidence interval.
Treatment of patients with EM and late disease manifestations
The majority (63/74, 85.1%) of the patients with EM were treated with oral doxycycline (2 × 100 mg/day), eight were treated with oral amoxicillin (3 × 500 mg/day) and three with intravenous ceftriaxone 2 g/day, with treatment duration ranging between 10 and 21 days. One patient with EM recidivans was initially treated with amoxicillin and then with oral doxycycline over 14 days with a prompt resolution of symptoms. Two 14-day courses of oral doxycycline were administered to the patient with multiple EM. The patient with late development of dyspnea, palpitations, fatigue, and arthralgia with a seroconversion was hospitalized and was treated with intravenous ceftriaxone for 14 days.
Discussion
LB is present in Kosovo and is related to the presence of I. ricinus in the environment (Sherifi et al. 2018). This observation finding is that all ticks removed from patients, which could be preserved for identification without damaging while removing them, were I. ricinus. This finding is also consistent with reports that nymphs and adult females are most commonly responsible for bites in humans (Wilhelmsson et al. 2013, Cayol et al. 2017).
Unimodal and bimodal patterns of seasonal tick questing activity have been reported in Europe, varying between years and regions (Wilhelmsson et al. 2013, Cayol et al. 2017). Spring and early summer are critical months for the questing activity of I. ricinus, while tick activity decreases during warm summer months and increases again in autumn (Piesman and Humair 2011, Cayol et al. 2017). These observations are more consistent with the unimodal pattern (most cases seen in May and June).
Specific occupations (forestry workers, hunters, farmers, etc.) and rural populations have an exceptionally high risk of tick bite exposure (Lindgren and Jaenson 2006, Di Renzi et al. 2010). The subjects of our study stand for the general population, including urban population and recreational activities, and close to half of participants had previous experience with tick bites in the past, and positive IgG seroprevalence in first visit was found in 7.4% of participants (Table 2).
EM is the most common manifestation of LB (van den Wijngaard et al. 2017, Enkelmann et al. 2018, Stanek and Strle 2018). In this study, all the EM were in relation to site of the tick bite, and the interval between the tick bite and the visibility of the EM was from 2 to 23 days after the tick bite. The diagnosis is clinical (Stanek et al. 2011) and diagnostic accuracy largely depends on medical expertise (Sajanti et al. 2017).
Although serological confirmation of infection is needed for other forms of the disease (Steere et al. 2016, Stanek and Strle 2018), serological confirmation (seroconversion) after 2 months of clinically observed EM during this study was only observed in 15 seronegative patients, 3.9% of all subjects included in the study. The range of overall risk of LB after tick bite estimates of 0.8–5.2%, reported from prospective studies in Switzerland, Sweden, Finland, and the Netherlands (Nahimana et al. 2004, Wilhelmsson et al. 2016, Hofhuis et al. 2017).
However, convalescent serology may be falsely negative in patients exposed to antibiotic treatment early in the course of the disease (Aucott et al. 2009, Stanek et al. 2011, Hofhuis et al. 2013). Early antibiotic treatment in clinically observed EM was common in our observational study. On the other hand, positive antibody immune response and a persistent positive IgG titer after treatment are found mostly in patients with longer duration or larger sized EM before therapy (Glatz et al. 2006). EM was observed also in 11 seropositive participants (for IgM or IgG) in the first visit, while nine seronegative participants in the first visit developed seroconversion in the second visit (2 months after), without any clinical manifestation during the period of 6 months of follow up.
Nevertheless, there are limitations on serology in our study where only ELISA was used as a laboratory support. Due to no prior data for LB in Kosovo, our investigation was mainly a clinical approach, with tick bite (embedded tick in the skin) criteria fulfillment in all cases.
Only two patients during this study developed the early disseminated form of LB, and one developed EM recidivans. One cannot exclude the possibility that appropriate antibiotic treatment of EM contributed to preventing other forms of the disease in the study—but this is highly hypothetical.
Doxycycline and amoxicillin were mainly used as first-line therapy (Lindgren and Jaenson 2006) in this study for the treatment of borrelial skin lesions. Indication for antibiotic prophylaxis after a tick bite is a controversial issue. The strongest indication in highly endemic areas when an engorged tick is attached for ≥36 h, but would also be reasonable when the duration of tick attachment, is uncertain (Warshafsky et al. 2010, Aucott and Luft 2016, Steere et al. 2016).
In Europe, antibiotic prophylaxis is not generally recommended since its efficacy is not considered proven (Steere et al. 2016). Also, Ixodes ticks need 17–48 h to transmit Borrelia to humans and animals (Weber 2001, Nahimana et al. 2004, Stanek et al. 2012). Thus, if the tick is removed quickly, other treatments are not generally required (Steere et al. 2016). On the other hand, a single 200 mg dose of doxycycline within 72 h of tick removal has been shown 87% effective in preventing the development of EM around the bite site (Nadelman et al. 2001, Wormser et al. 2006, Hofhuis et al. 2017).
In this study, the duration of tick attachment was unknown in 50% of the patients and was >72 h in additional 6.8%, while in around 25% of the patients, it happened within 24 h, but this was not the main criterion for antibiotic prophylaxis-doxycycline to be administered in patients with engorged or swollen ticks.
In the multivariate analysis—which should be taken with caution considering the study design likely resulting in residual confounding—early antibiotic use was associated with a reduced risk of clinically manifested diseases. This finding is suggestive of a possible effect of prophylaxis. In line with the expectations (Hofmann et al. 2017), proper removal of the entire tick was associated with a considerably reduced risk of disease. As mentioned earlier, the observed apparent differences between the location of Pristina and other parts of Kosovo are likely due to confounding-by-indication. Finally, although there appeared a trend of a higher risk of LB in the years 2017 and 2018 versus 2015, this is highly uncertain considering the small number of subjects seen during the last 2 years of the study.
This study is limited by its design: it did not record all tick bites (most certainly, the unknown number of clinically unremarkable bites and those seeking medical advice elsewhere were missed), but just those cases where patients felt the need to specifically contact the single research site. Hence, the true risk of LB could not be estimated; however, it likely provides a relatively accurate data about clinical manifestations of the LB following a tick bite in this specific subset of patients (seeking medical help at a specialized institution).
Conclusion
In conclusion, this study provides the first data about human LB in Kosovo. In many aspects, these findings are in agreement with similar reports from other European countries. In general, this assessment of the disease following tick bite can be helpful in indicating the need for disease awareness and reinforcing the importance of primary prevention measures to prevent Borrelia transmission due to tick bites. Also, the importance of early diagnosis and appropriate treatment to prevent late severe stages of the disease.
Ethics Approval
The study was approved by the local Ethical Committee University Clinical Center of Kosovo (Protocol number: 1578;17.04.2014).
Footnotes
Authors' Contributions
A.P-B. designed the study, managed the recruitment of the subjects, conducted the acquisition of data, analysis, and interpretation of data, made the conception, and wrote the article; S.A. managed the recruitment of the subjects and facilitated the acquisition of data; S.A. and A.B. conducted monitoring and acquisition of data; V.T. and A.P-B. statistically analyzed and interpreted the data and critically revised the article for important intellectual content; G.T. drafted and critically revised the article for important intellectual content. All authors gave final approval of the version to be submitted.
Acknowledgments
The authors wish to thank the study participants for their contribution to the research. The authors specifically thank Professor Kurtesh Sherifi for identifying ticks, and Xhevat Jakupi, PhD, and his medical/technical staff (Sevdie and Florim) at the National Institute of Public Health of Kosovo for their support. They also thank the Clinic of Infectious Diseases in Pristina, colleagues, and all medical staff for supporting this research.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.