
Abstract
Q fever and tick-borne borreliosis are two zoonotic diseases rarely diagnosed in Senegalese health facilities, particularly in rural areas. Our study aims to better understand the circulation of Coxiella burnetii and Borrelia spp. DNA on human skin and the domestic environment in rural areas. Cutaneous swabs were taken from febrile patients being treated for borreliosis and/or Q fever, the members of patients' households and control households in the Niakhar area. Dust samples were also collected from 90 households where 54 cases of borreliosis and Q fever were reported as well as from the households of members of control populations in Dielmo, Ndiop, and Niakhar. C. burnetii and Borrelia spp. DNA were detected by quantitative PCR in cutaneous swabs and dust samples targeting spacers IS1111_IS30A and Bor 16S gene. Of 1365 persons tested, 76 were shown to carry C. burnetii, 13 Borrelia spp., and 6 were identified as carrying both C. burnetii and Borrelia spp. The prevalence of Borrelia spp. DNA in households was 16.7% in Dielmo, 6.7% in Ndiop, and 23.3% in all other villages in the Niakhar area, and the presence of C. burnetii in the same localities was 10%, 13.3% and 66.7%, respectively. Furthermore, C. burnetii genotyping identified the presence of Multispacer Sequence Typing group 6. These results revealed for the first time the carriage on the skin of C. burnetii and Borrelia spp. DNA in humans and its wide distribution across households. Our findings suggest that many populations are exposed to these diseases, with frequent contaminating cases of infectious origin arising from the domestic environment.
Introduction
Q
Tick-borne relapsing fever is also a zoonotic bacterial disease present in Saharan, Sahelian, and Sudano-Sahelian areas of West Africa (Trape et al. 1996). The pathogen responsible for this disease is the spirochete Borrelia crocidurae (Lecompte and Trape 2003).
Humans are infected through bites of the soft tick Ornithodoros sonrai (Lecompte and Trape 2003), the only known vector that lives in rodent burrows (Lecompte and Trape 2003, Diatta et al. 2015), and which can occasionally bite outdoors, especially when burrows open into homes (Trape et al. 2013). A recent study has shown an exceptional carriage (31.5%) of C. burnetii in O. sonrai ticks in the Niakhar area (Ndiaye, unpublished data). In Senegal, the prevalence of Borrelia infection observed in humans in four health facilities in Niakhar was 19.1% (Mediannikov et al. 2014), and the highest incidence of this disease (11%) was observed in the population of Dielmo (Vial et al. 2006). However, a strategy of preventive control of borreliosis established in Dielmo and Ndiop has significantly reduced the incidence of this disease in both villages, falling, respectively, from 10.5 to 2.63 cases per 100 person-years and from 3.79 to 1.39 cases per 100 person-years (Diatta et al. 2016). Small mammals acting as reservoirs of Borrelia (Diatta et al. 2015), may also harbor C. burnetii, especially Rattus norvegicus and Rattus rattus (Reusken et al. 2011, Stragier, unpublished data).
Few data regarding the DNA presence of C. burnetii and Borrelia spp. in the environment in Senegal are available. Recently, a weak correlation has been established between positive environmental samples and the Q fever disease (Ratmanov et al. 2012), but no studies have yet been undertaken to show the cutaneous carriage of C. burnetii and Borrelia spp. DNA in humans.
The aim of our study was to better understand the circulation of C. burnetii and Borrelia spp. DNA on human skin and the domestic environment in rural areas to improve prevention and control strategies.
Materials and Methods
Ethical approval
The Comité National d'Ethique pour la Recherche en Santé of Senegal approved this study in the context of epidemiological fevers surveillance (with the following statement number #0087).
Niakhar area
The Niakhar District falls between latitudes 14°36′N/14°21′N and longitudes 16°18′W/16°30′W, in the Fatick region, 155 km southeast of Dakar and 15 km north of Fatick. It has a surface area of 388 km2 (Abat et al. 2016). The population is estimated at >55,000 inhabitants, and more than half are under the age of 20 (Chippaux 2005). The climate is typically Sahelian and temperatures are less extreme. The average annual rainfall was estimated at 757.4 mm in 2008. The Serer population is the predominant ethnic group, representing ∼96.5% of the population (Delaunay et al. 2003).
Dielmo and Ndiop sites
The villages of Dielmo (13°41′N/16°23′W) and Ndiop (13°43′N/16°24′W) with 510 and 481 inhabitants, respectively, are 5 km apart. Dielmo is located 280 km southeast of Dakar and 15 km north of the Gambian border. The vegetation and climate correspond to the Sudan savanna zone. Precipitation occurs over a period of 4 months, from June to October. The village of Ndiop is populated mainly by the Wolofs and the village of Dielmo is dominated by the Sereres. In both villages, agriculture is the main activity during the rainy season. During the dry season, gardening remains a family activity (Diatta et al. 2016).
Selection of febrile patients
The patients enrolled in this study were examined in four health facilities in the Niakhar area and in the villages of Dielmo and Ndiop. For each patient presenting a febrile syndrome, with a fever ≥37.5°C, a capillary blood sample was immediately taken and pathogens responsible for the fever were investigated in the Point-of-Care (POC) laboratory in Niakhar or Dielmo using real-time quantitative PCR (qPCR) with specific primers and quenchers targeting Borrelia spp. and C. burnetii. A clinical database from the POCs containing the results of the molecular tests made it possible to identify all cases of febrile pathologies that occurred in inhabitants of the Niakhar, Dielmo, and Ndiop areas. We were thus able to access all the information relating to patients suffering from borreliosis or Q fever mixed with Borrelia infection. In other words, every patient diagnosed as being infected with borreliosis or Q fever mixed with Borrelia infection was selected to participate in the study.
Cutaneous swabs collection in Niakhar area
After completing the informed consent procedure and signature of the informed consent by adult participants and parents or legal guardians of minors from Niakhar area, swabs were collected only in the villages of borreliosis patients and Q fever mixed with Borrelia infection, the members of patient's households, and control households. These control households represented households where no case of borreliosis and Q fever mixed with Borrelia infection was diagnosed, and who were, randomly selected based on their immediate proximity with the patient's households. With the participants' agreement, each swab was removed from its original tube and was soaked with drops of sterile saline. The left and right forearm of each participant was gently scraped with a soaked swab, which was then reintroduced into its original tube.
The borreliosis case code, the participant's references, and the sampling date were noted on each tube. The skin swabs were stored at 4°C in ambient temperature and at −20°C in the laboratory.
Collection of negative control
To ensure greater reliability of the test, negative controls were performed outside the Niakhar area. Cutaneous swabs were collected after obtaining informed consent signed by IRD staff, using the same methodology mentioned previously.
Dust sample collection in the villages of Dielmo and Ndiop and in the Niakhar area
Dust samples were taken from sleeping rooms, selected randomly from households where borreliosis patients and Q fever mixed with Borrelia infection lived in Dielmo, Ndiop, and other villages in the Niakhar area. Bedding, the sides of the beds, along the bed, the bedsprings, the windows, and the doors were targeted. Dust samples were collected using a soft toothbrush and a urine container. The participant code, the sampling place, and the date were noted on each collection container, which was then kept at ambient temperature.
DNA extraction of cutaneous swabs
A bacterial suspension with 800 μL of phosphate-buffered saline (PBS) was first performed on each buffer. Each Eppendorf tube was marked with the participant code. For extraction, 200 μL were used and the remaining 600 μL was stored for other purposes at −20°C. For each sample, 200 μL of 2% cetyltrimethylammonium bromide (CTAB) was added and incubated at 56°C overnight. After incubation, we added 200 μL of chloroform, inverted mixture, and centrifuged at 12,000 rpm for 5 min. The supernatant was then removed and placed in another empty tube with the same number as the participant, and 200 μL of isopropanol was added to this supernatant and centrifuged at 12,000 rpm for 15 min. The tubes were then emptied and drained thoroughly on paper towels. The pellet was dried in a speed-vac for a maximum of 5 min and washed in 200 μL of elution buffer. The DNA extracts were maintained at 4°C before use for PCR amplification.
DNA extraction from the dust samples
Part of each dust sample was transferred to 1.5 mL Eppendorf tubes into which 1 mL of PBS was added. Each tube was vortexed and centrifuged at 12,000 rpm for 15 min. We removed the supernatant, to which we added 200 μL of 2% CTAB and then incubated for 24 h. After incubation, we applied the same process as previously described for the cutaneous swabs.
Real-time qPCR
Real-time qPCR was used to detect the presence of C. burnetii DNA and Borrelia spp. in samples processed according to the DNA amplification protocol with CFX96. DNA from positive controls for C. burnetii and Borrelia spp. were obtained in the laboratory and a negative control consisting of 5 μL of ultrapure water was used to ensure the reliability of the test. The presence of Borrelia spp. was detected by amplification of a 148-pb fragment of the mitochondrial 16S rRNA gene, as previously described (Parola et al. 2011). The DNA of C. burnetii was investigated by performing a first-order qPCR targeting the IS1111 gene and a second confirming with the IS30A gene. The criterion of positivity of a positive qPCR was defined by a threshold value for a tested sample <35 cycle thresholds (Ct). A tested sample was considered positive for C. burnetii when the qPCR targeting the IS1111 and IS30A genes has <35 Ct for each gene (Mediannikov et al. 2010).
C. burnetii multispacer sequence typing genotyping
To perform a multispacer sequence typing (MST) of C. burnetii, samples with a Ct value <32 were subjected to standard PCR targeting three intergenic spacers Cox 2, 5, and 18. Primers sequences and targets are given in Table 1 (Glazunova et al. 2005). Amplification was conducted in the MiniAmp™ Thermal cycler (Applied Biosystems Technology, Thermo Fisher Scientific), following the thermal cycling conditions described previously. Thereafter, amplicons were visualized on agarose gel electrophoresis, followed by a purification on a NucleoFast 96 PCR plates (Macherey-Nagel EURL, Hoerdt, France) according to the manufacturer instructions. Three intergenic spacers were then sequenced using the Big Dye Terminator Cycle Sequencing Kit (Perkin Elmer Applied Biosystems, Foster City, CA) accompanied by an ABI automated sequencer (Applied Biosystems). Generated sequences were then assembled ChromasPro software (ChromasPro 1.7; Technelysium Pty Ltd, Tewan-tin, Australia). Finally, the present MST group of C. burnetii was identified using the freely available MST database.
Primers Names and Sequences Used for Polymerase Chain Reaction and Sequencing of Coxiella burnetii Spacers
Statistical analyses
The proportions of the cutaneous carriage of C. burnetii DNA, Borrelia spp., and of the association of C. burnetii/Borrelia spp. DNA in the households studied were evaluated. Furthermore, variations in the cutaneous carriage of the DNA of these two bacteria in borreliosis cases, the members of patients' households, and control households were evaluated, as well as the dispersion of their bacterial DNA in household dust. Significance tests were performed using the Open Epi software, version 3.01 (08/12/17) and R studio, version 3.4.1. To compare the variables, chi-squared tests were applied when necessary. The difference between two values was deemed to be significant when the significance limit “p” is <5% (p < 0.05).
Results
Cutaneous swab sampling and molecular analysis
Of 106 households visited, 2730 skin swabs were collected from 1365 persons. The cutaneous swab samples were randomly obtained from 54 (3.96%) patients who had developed borreliosis including 7 Q fever mixed with Borrelia infection; 774 (56.7%) persons were living in households with borreliosis patients and 537 (39.34%) others lived in control households. Of the 1365 persons sampled, 630 (46.15%) were men and 735 (53.85%) women. DNA extracted from the skin swabs tested by qPCR revealed that 5.57% (76/1365) (95% confidence interval [CI, 4.47–6.91]) of tested persons carried C. burnetii DNA, 0.95% (13/1365) (95% CI, 0.55–1.62) carried Borrelia spp., and 0.44% (6/1365) (95% CI, 0.20–0.95) carried C. burnetii and Borrelia spp. DNA (Table 2).
Proportions of Carriage of Coxiella burnetii, Borrelia spp. DNA, and of the Association of Coxiella burnetii/Borrelia spp. Bacterial DNA in the Households Studied in Niakhar Area, Senegal
Bor, Borreliosis; CI, confidence interval.
Cutaneous carriage of C. burnetii, Borrelia spp. DNA, and bacterial DNA association in the studied households
The proportions of the cutaneous carriage of C. burnetii DNA were 56.6% (43/76) (95% CI, 45.39–67.14) in households where borreliosis patients lived, 38.2% (29/76) (95% CI, 28.06–49.4) in the control households, and 5.3% (4/76) (95% CI, 2.06–12.77) in patients identified with borreliosis (Fig. 1). In contrast, proportions of skin carriage of Borrelia spp. DNA were 61.5% (8/13) (95% CI, 35.52–82.29) in the control households, 31% (4/13) (95% CI, 12.68–57.63) in those of the borreliosis patients' households, and 7.7% (1/13) (95% CI, 1.37–33.31) in the borreliosis patients (Fig. 1). The proportion of cutaneous carriage of C. burnetii was greater in the households of borreliosis patients than in those of control households where no cases were reported and in patients diagnosed with borreliosis. The proportion of the carriage of Borrelia spp. was higher in the control households than in those of members of borreliosis patients' households and even in cases of borreliosis. Statistical analysis revealed a nonsignificant variation in the carriage of C. burnetii DNA (chi-squared corrected Yates test = 0.92, p > 0.05) and Borrelia spp. DNA (chi-squared corrected Yates test = 0.1737, p > 0.05) between the households. Carrying the bacterial DNA of C. burnetii and/or Borrelia spp. is not related to the carrier's membership of a standard household. Simultaneous cutaneous carriage of C. burnetii and Borrelia spp. DNA was found in 1.3% (1/76) (95% CI, 0.23–7.08) of the households of the borreliosis cases and 6.6% (5/76) (95% CI, 2.84–14.5) in the control households studied (Table 2). No cases of C. burnetii/Borrelia spp. association was identified in confirmed cases of borreliosis. In total, six cases of mixed carriage (7.9%) (95% CI, 3.7–16.2) of bacterial DNA C. burnetii/Borrelia spp. were detected in households.
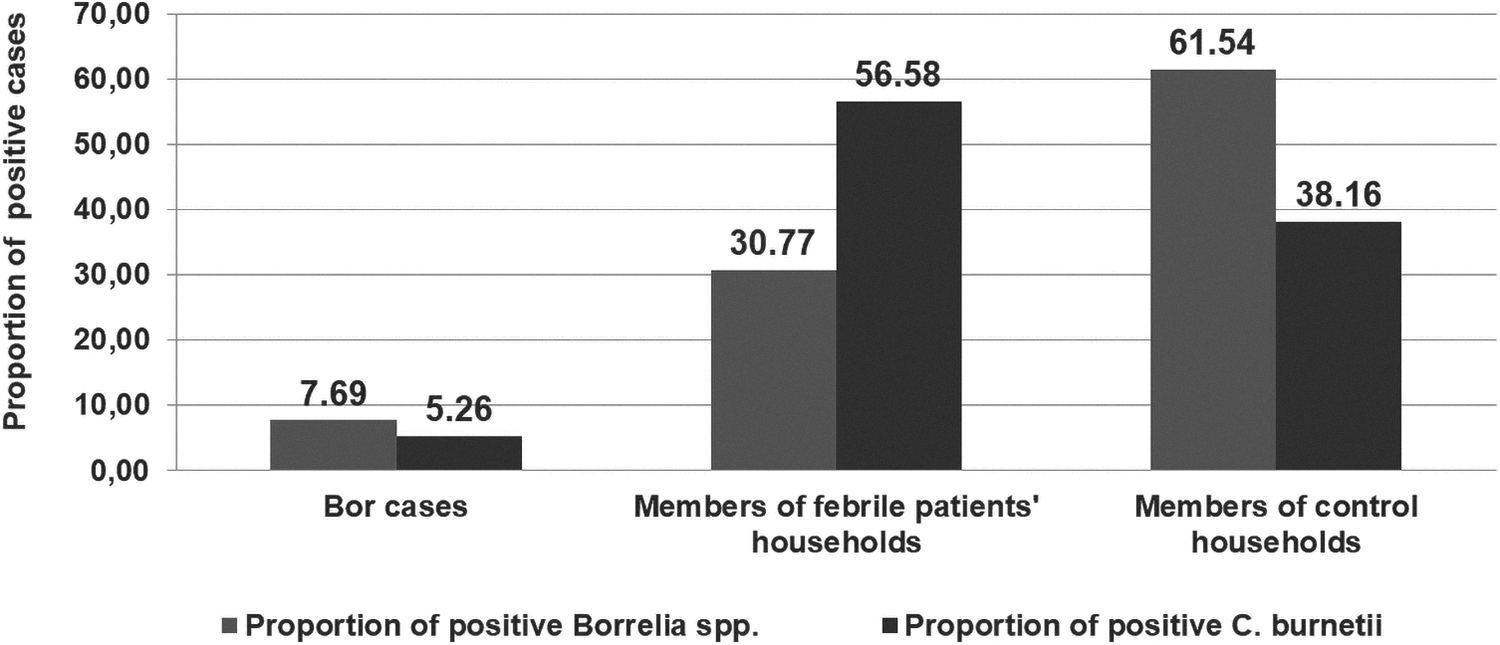
Variation of cutaneous carriage of Coxiella burnetii and Borrelia spp. DNA in borreliosis patients, members of febrile patients' households, and control households in the Niakhar area.
Negative control test
The result expected by the negative control test was obtained. All skin swabs collected (112 sampled) were negative for both pathogens being investigated.
Dust samples and molecular analysis
A total of 451 dust samples were collected from 90 households, namely 30 households in each study site. The data collected are summarized in Table 3. The qPCR analysis of the DNA extracts from the dust samples revealed the presence of C. burnetii DNA in 6% (27/451) of the samples tested, Borrelia spp. in 3.1% (14/451), and DNA association of the two bacteria in 0.6% (3/451) of cases.
Dust Collection Workforces in Dielmo–Ndiop Villages and in Other of Niakhar Area
Proportion of Borrelia spp. DNA in dust samples of studied households
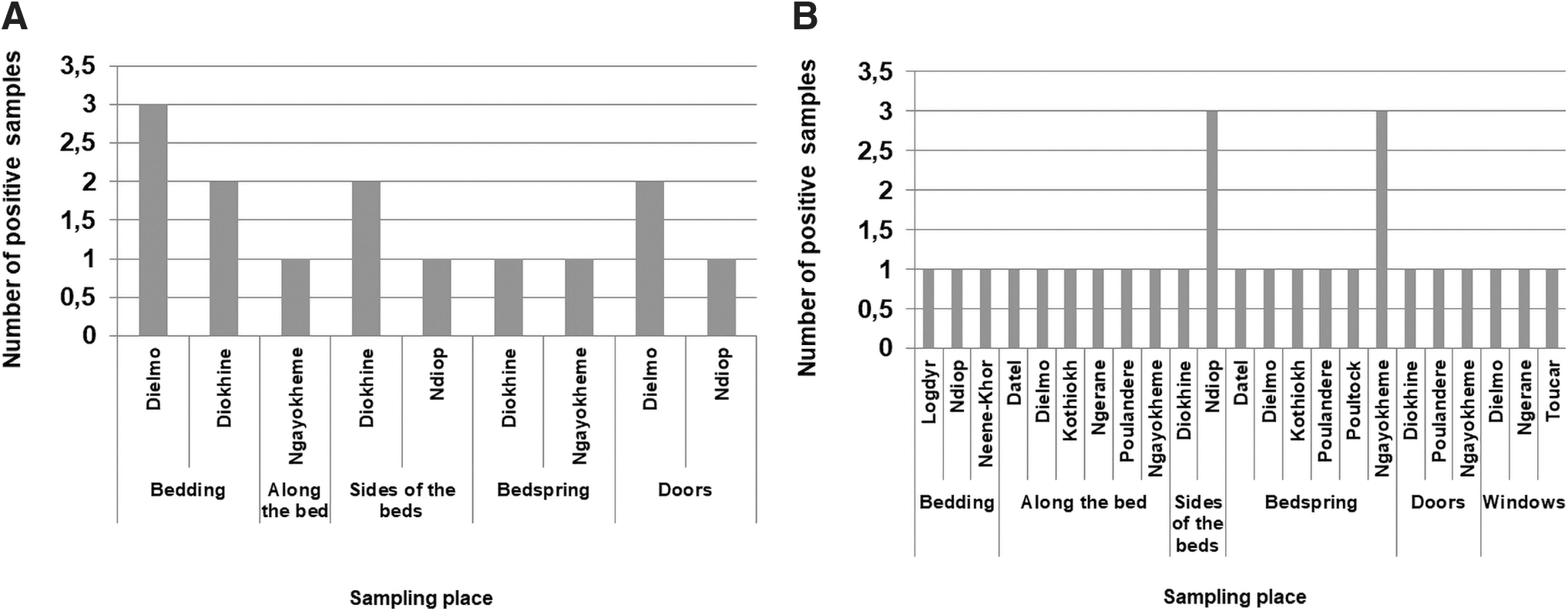
The presence of Borrelia spp. DNA was identified in 14 (3.1%) dust samples, of which 16.3% (5/31) were detected in bedding in Dielmo and Diohine, 15.15% (3/3) on the sides of the beds in Diohine and Ndiop, 25% (1/4) along the length of the bed in Ngayokheme, 5.1% (3/59) on the doors in Dielmo and Ndiop, and 25% (2/8) on the bedsprings in Diohine and Ngayokheme (Fig. 2A). The prevalence of this bacterial DNA in households was 16.7% in Dielmo, 6.7% in Ndiop, and 23.3% in all other villages in the Niakhar area.
Density of presence of Borrelia spp.
Proportion of C. burnetii DNA in dust samples of studied households
The DNA of C. burnetii was found in 27 dust samples, of which 9.7% (3/31) were on bedding in Logdyr, Ndiop, and Neene-kor; 12.1% (4/33) on the bedsides in Diohine and Ndiop; 12.5% (3/24) on the windows in Dielmo, Ngerane, and Toucar; 16.2% (6/37) along the length of the bed in Datel, Dielmo, Ngérane, Kothiokh, Ngayokheme, and Poulandere; 27.3% (3/11) on the doors in Diohine, Ngayokheme, and Poulandere; and 25% (8/32) on the bedsprings in Datel, Kothiokh, Dielmo, Ngayokheme, Poulandere, and Poultock (Fig. 2B). The prevalence of C. burnetii DNA in households from Dielmo, Ndiop, and the Niakhar area was 10%, 13.3%, and 66.7%, respectively.
MST genotyping of C. burnetii strains
In total 14 of 107 positive C. burnetii samples harbored a Ct value <32 and were subjected to MST genotyping. C. burnetii genotype was identified using Cox 2 and 5 spacer sequences, and validated using the Cox 18 sequence. Genotype 6 was identified in 13 of 14 samples collected from cutaneous swabs in Niakhar, Senegal. In addition, a potential new Cox genotype was identified with one Cox2 sequence.
Association of C. burnetii and Borrelia spp. DNA in dust samples
In total, three cases of C. burnetii/Borrelia spp. DNA association were found in the dust collected in the Niakhar area, more specifically, two cases in Diohine and Ngayokheme and one other in Ndiop. This association was identified in one case on the bedsides in Diohine and one other in Ndiop, as well as in one case in bedsprings in Ngayokheme. The presence of C. burnetii DNA was most detected on dust from the bedsprings (10%, 8/80) and length of the bed (7.1%, 6/84) (Fig. 3), was regularly found in the bedding (3.6%, 3/83), doors (3.3%, 3/91), windows (5.7%, 3/52), and bedsides (4.9%, 3/61). In contrast, Borrelia spp. DNA was mainly found on bedding dust (6%, 5/83) and dust from the bedsides (4.9%, 3/61) (Fig. 3), followed by dust from the doors (3.3%, 3/91) and, to a lesser extent, on the bedsprings (2.5%, 2/80) and along the length of the bed (1.2%, 1/84). No traces of Borrelia spp. DNA was identified in the dust of the bedroom windows. Statistical analysis showed no significant difference in the density of presence of C. burnetii and Borrelia spp. (chi-square test = 2.40, p = 0.12 > 0.05).
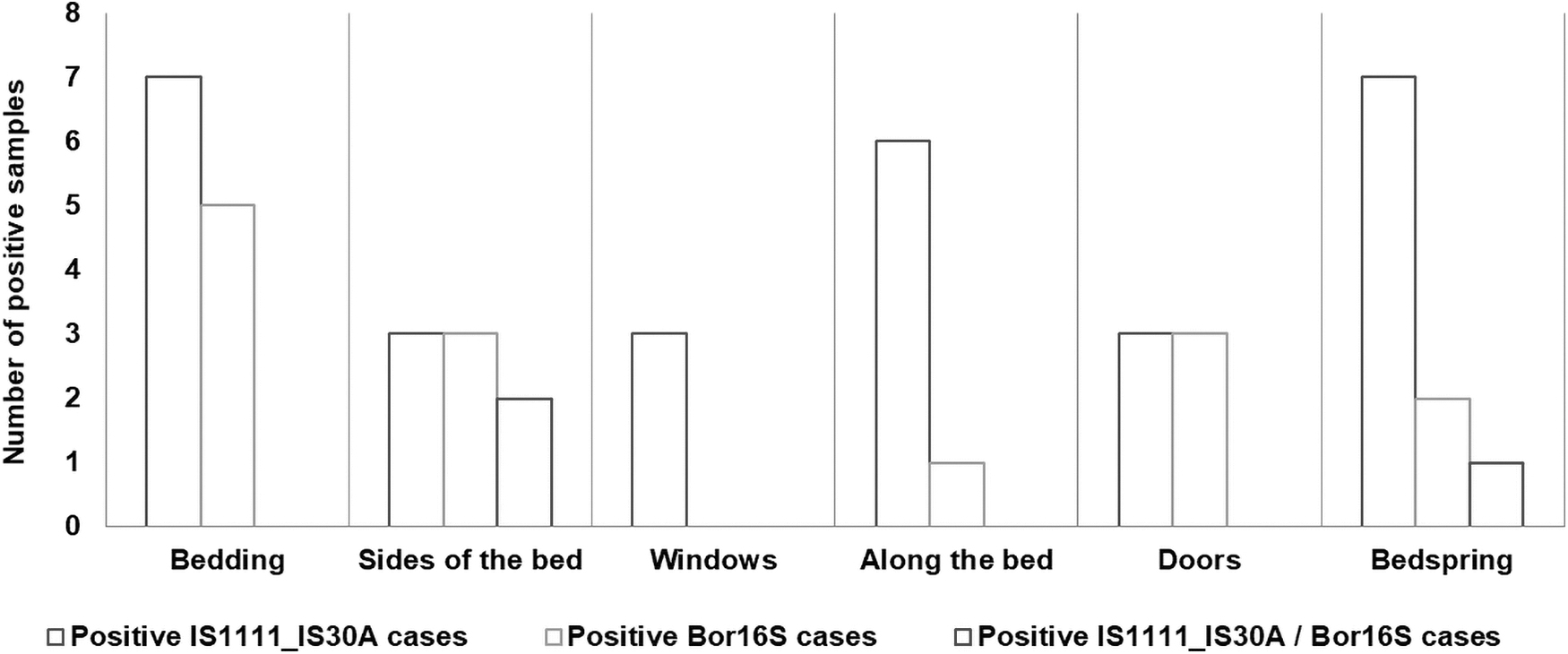
Variation in the density of C. burnetii, Borrelia spp. DNA, and the association of C. burnetii/Borrelia spp. bacterial DNA in the dust of studied households.
Discussion
Our study revealed for the first time the carriage of C. burnetii and Borrelia spp. DNA on human skin. The frequency of carriage of C. burnetii in all the households studied was 5.57%, with 56.6% and 38.2% of this DNA bacterium been identified, respectively, on the skin of the members of borreliosis patients' households and control households. In addition, the proportion of the carriage of Borrelia spp. was higher (61.5%) in the control households than in those of borreliosis patients (31%). Moreover, we have shown in this study that C. burnetii and Borrelia spp. were regularly present in dust collected in the sleeping rooms of studied households. C. burnetii DNA was detected with a higher prevalence of 66.7% in the Niakhar area, where no previous studies have been conducted to assess the prevalence of this DNA bacterium in human habitations. Molecular tests were performed by qPCR to highlight the occurrence of these two bacteria on the human skin and confirm their massive distribution within household rooms of rural dwellings. In addition, MST spacer typing was successful in 14 C. burnetii-positive samples genotype 6 detected in 13 samples from one locality (Niakhar). Of interest, this C. burnetii genotype was previously detected in ticks from Dielmo, Senegal (Mediannikov et al. 2010) and in a patient with endocarditis in France (Glazunova et al. 2005). Negative control tests for the qPCR and skin swabs collected validated the reliability of results, as well as the use of DNA from positive controls for C. burnetii and Borrelia spp. in all amplification analyses. Molecular techniques of qPCR used in this study were sensitive to detect DNA bacterial, and made, so, robust the results obtained.
Human cases of Q fever and borreliosis are rarely diagnosed in health structures in Senegal. Using molecular diagnostic tools by real-time PCR at the POC in Dielmo and Niakhar, screening for Borrelia and C. burnetii infections was carried out in rural areas to provide rapid treatment for patients. The proximity of infected domestic ruminants to human habitations could play a major role in the spread of C. burnetii, as previously reported (Kersh et al. 2010). Other previous studies have demonstrated the presence of C. burnetii and Borrelia spp. in feces from small rodents and insectivores frequenting human habitations (Kersh et al. 2010, Reusken et al. 2011). It would be interesting to know whether the skin carriage of bacterial DNA could currently, or in the medium term, be a source of human contamination with these two bacteria.
In the Niakhar area, populations seem appear to be more exposed to contact with dust contaminated by domestic livestock (reservoirs), which appears to be a dominant family farming activity in the area. In contrast, in Dielmo and Ndiop, the respective DNA prevalence of C. burnetii in dust within homes was 10% and 13.3%, higher than that reported by Ratmanov et al. (2012) in these two villages. Circulation of C. burnetii DNA is still higher in Ndiop than in Dielmo, probably because domestic breeding is more widely practiced in the village of Ndiop. DNA from this bacterial agent was found in all villages surveyed, suggesting that C. burnetii is commonly excreted into the environment by livestock and naturally infected small mammals. There is a real risk of exposure to such a medium (Ratmanov et al. 2012) as the presence of C. burnetii bacterium in dust could be a direct source of contamination. In dust collected from studied households, Borrelia spp. DNA was found for the first time with variable proportions depending on the location, including 16.7% in Dielmo, 6.7% in Ndiop, and 23.3% in the Niakhar area, which may be linked to intradomiciliary attendance of infected small rodents. Borrelia spp. DNA that was absent on the windows could be related to the ecology of small mammal reservoirs and the endophilic nature of the O. sonrai tick vector.
Cutaneous carriage of C. burnetii DNA was predominant in homes within households where borreliosis cases had been identified, whereas Borrelia spp. DNA was massively detected in control households. However, carriage bacterial DNA of C. burnetii and/or Borrelia spp. is not linked to membership of a specific household. In addition, the DNA presence of these two bacteria in dust proves that the environment in which the rural populations live is not free from these pathogens. It remains to be seen whether viable bacteria have been disseminated in the environment that may be responsible for human contamination. It would, therefore, be interesting to investigate how these two bacterial DNA found in cutaneous samples and in dust samples could be a plausible source of human contamination.
Footnotes
Acknowledgments
The authors thank the inhabitants of the villages of Ngayokheme, Poudaye, Niakhar, Poulander, Diohine, Neene-khor, Datel, Logdyr, Gadiack, Poultock, Kathiock, Nguerane, Ngalane, Toucar in Niakahar area and the other of Dielmo and Ndiop in the Saloum, Senegal.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This study was supported by the Institut Hospitalo-Universitaire Méditerranée Infection, the French National Research Agency under the “Investissements d'avenir” programme, reference ANR-10-IAHU-03, the Région Provence Alpes Côte d'Azur and European regional development funding of platforms research and innovation mutualized Mediterranean Infection (FEDER PRIMMI).