
Abstract
A clinical and entomological investigation was performed to identify flavivirus infections in humans and mosquitoes in impoverished areas of Guerrero, a coastal state in southwestern Mexico. A total of 639 patients with acute febrile illness and 830 resting female mosquitoes in low-income communities of Guerrero in 2019 were tested for evidence of flavivirus infection. Sera were collected from all patients and screened at a dilution of 1:20 by plaque reduction neutralization test (PRNT) using dengue virus (DENV)2. A total of 431 (67.4%) patients were seropositive. Sera from a subset of seropositive patients (n = 263) were tested for flavivirus NS1 by enzyme-linked immunosorbent assay. Forty-eight (18.3%) sera contained viral antigen. All NS1-positive sera were titrated and further tested by PRNT using DENV-1 to -4, St. Louis encephalitis virus, West Nile virus, and Zika virus (ZIKV). Seven patients were seropositive for DENV-1, five patients were seropositive for DENV-2, one patient was seropositive for DENV-3, and two patients each were seropositive for DENV-4 and ZIKV. The remainder had secondary flavivirus infections or antibodies to an undetermined flavivirus. Comparative PRNTs were also performed on 60 randomly selected NS1-negative sera, identifying patients seropositive for DENV-2, DENV-3, and ZIKV. The entomological investigation yielded 736 Aedes aegypti and 94 Culex quinquefasciatus that were sorted into 183 pools and 20 pools, respectively. Mosquitoes were assayed for flavivirus RNA by RT-PCR and Sanger sequencing. DENV-2 RNA was detected in three pools of A. aegypti. In summary, we provide evidence for the concurrent circulation of all four DENVs and ZIKV in Guerrero, Mexico. The public health authorities reported no cases of DENV-3, DENV-4, and ZIKV in Guerrero in 2019 and thus, we provide evidence of under-reporting in the region.
Introduction
Mosquito-borne viruses have an enormous impact on human health. Of particular concern is dengue virus (DENV; genus Flavivirus, family Flaviviridae), which is hyperendemic in numerous countries in the tropics and subtropics (Gubler 2011, Simmons et al. 2012, Guzman et al. 2016). DENV causes an estimated 390 million infections worldwide each year, including 96 million infections that result in clinical episodes (Bhatt et al. 2013). In Mexico, DENV is responsible for an estimated 139,000 symptomatic infections each year, which is 4.5-fold higher than the officially reported number, indicating that there is gross under-reporting (Undurraga et al. 2015). The economic burden of DENV in Mexico is estimated to be US $170 million per year, including surveillance and vector control costs.
DENV is transmitted primarily by Aedes aegypti and occurs as four genetically and antigenically related viruses (also known as serotypes), designated as DENV-1 to -4 (Gubler 2011, Simmons et al. 2012, Guzman et al. 2016). All four serotypes are the etiological agents of dengue, a self-limiting febrile illness often accompanied by severe headache, malaise, severe joint and muscle pain, nausea, vomiting, and rash. Dengue can progress to life-threatening disease, that is, severe plasma leakage, severe bleeding, and organ failure. Infection with any serotype induces protective immunity to that serotype, but does not confer long-term protection against infection by other serotypes. A secondary heterologous DENV infection greatly increases the risk of severe disease through antibody-dependent enhancement (Halstead 2014). The World Health Organization previously classified dengue using three disease categories: dengue fever, dengue hemorrhagic fever, and dengue shock syndrome (WHO 1997). The guidelines were revised in 2009, with cases now classified as either dengue with or without warning signs or severe dengue (WHO 2009). The Secretariat of Health (Secretaría de Salud) in Mexico adopted the most recent guidelines in 2016.
Other mosquito-transmitted flaviviruses that occur in Mexico include Zika virus (ZIKV), West Nile virus (WNV), and St. Louis encephalitis virus (SLEV) (Estrada-Franco et al. 2003, Hernandez-Avila et al. 2018, Simon et al. 2020). These viruses produce clinical presentations that overlap with dengue, creating a diagnostic challenge for clinicians in regions where they co-circulate. The Secretariat of Health in Mexico co-ordinates nationwide testing for DENV and ZIKV, but nationwide testing for WNV and SLEV is not performed (Anonymous 2020a, 2020b). Diagnostic testing for DENV and ZIKV is usually performed in state diagnostic laboratories using enzyme-linked immunosorbent assays (ELISAs) that detect viral antigen. Quantitative RT-PCR (qRT-PCR) is also used, although less often, for DENV and ZIKV diagnosis and is performed at the National Institute for Diagnosis and Epidemiological Reference in Mexico City. The qRT-PCR for DENV is serotype specific.
Many residents of Mexico live in poverty and, therefore, have restricted access to health care and diagnostic testing. This is especially true in Guerrero, a coastal state in southwestern Mexico that has the second highest (69.7%) poverty rate in the nation. It is, therefore, likely that infectious diseases are grossly under-reported across the state. The goals of this study were to perform a clinical and entomological investigation to identify flaviviruses circulating in impoverished areas of Guerrero and to provide insight into whether cases are under-reported.
Methods
Sample population and performance sites for the clinical investigation
The sample population consisted of febrile patients who presented from May to November 2019 at select performance sites in Guerrero, a coastal state in southwestern Mexico (Fig. 1). Many patients presented at the following six hospitals and associated clinics: Centro de Salud con Servicios Ampliados de Tierra Colorada in Tierra Colorada, Hospital de la Comunidad de Tixtla in Tixtla, Hospital General Adolfo Prieto in Taxco de Alarcón, Hospital General Raymundo Abarca Alarcón in Chilpancingo, Laboratorio Nobel in Zumpango, and Labymedic Laboratorios in Acapulco. Other patients presented at the Laboratorio de Investigación en Citopatología e Histoquímica in the Universidad Autónoma de Guerrero, Chilpancingo after an announcement was made to the community using social media and by posting flyers in public areas to recruit study participants.
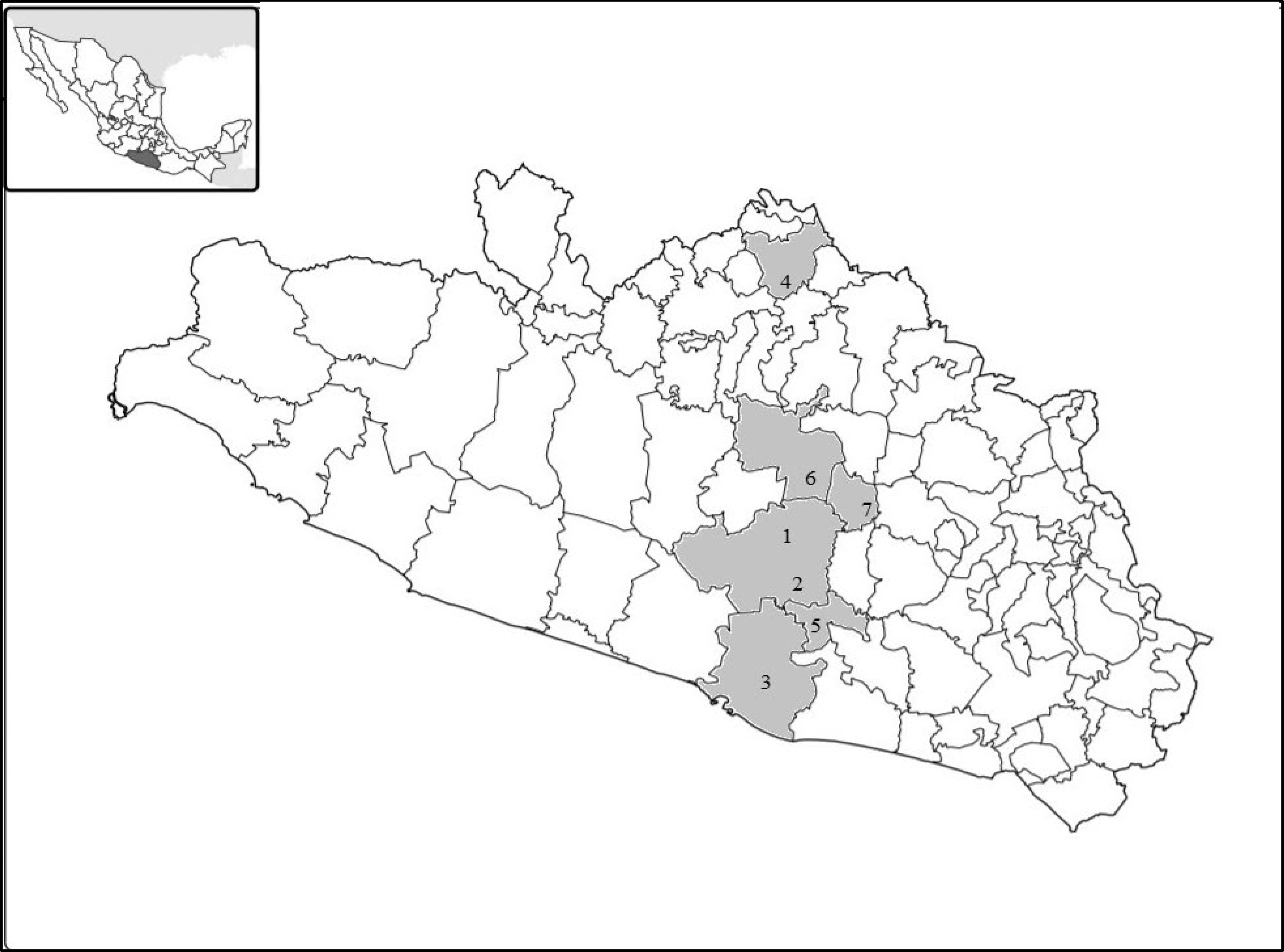
Geographic location of the performance sites. State map of Guerrero with municipality borders shown. Municipalities with performance sites are shaded light gray. Performance sites are as follows: 1. Hospital General Raymundo Abarca Alarcón in Chilpancingo, 2. Universidad Autónoma de Guerrero, Chilpancingo, 3. Labymedic Laboratorios in Acapulco, 4. Hospital General Adolfo Prieto in Taxco de Alarcón, 5. Centro de Salud con Servicios Ampliados de Tierra Colorada in Tierra Colorada, 6. Laboratorio Nobel in Zumpango, and 7. Hospital de la Comunidad de Tixtla in Tixtla. The inset in a map of Mexico with Guerrero shaded dark gray.
The study was designed to target individuals from communities poorly represented in the national arbovirus diagnosis and surveillance programs. To be eligible for inclusion, patients had to present with an acute unspecified fever and at least two of the following: nausea/vomiting, rash, aches and pains, leukopenia, and a positive tourniquet test, which meets the clinical criterion for dengue, and live in a low-income household in Guerrero and have not left the state in the past 12 months. Routine blood testing and physical examinations were performed on all patients, but all declined to undergo additional testing through the national health care system because it was cost prohibitive. Medical and laboratory personnel from the participating hospitals and associated outpatient clinics provided sera and select demographic information from undiagnosed patients who met the inclusion criteria, but were not willing to provide detailed medical information because of the time and effort needed to compile these data. Therefore, we were not provided with sufficient information to classify patients into dengue disease categories or to report disease outcomes. Sera were transported by express delivery on ice packs to Iowa State University. Institutional Review Board (IRB) approval was granted before the study began.
Plaque reduction neutralization test
Plaque reduction neutralization tests (PRNTs) were performed using DENV-1 (strain Hawaii), DENV-2 (strain NGC), DENV-3 (strain H-87), DENV-4 (strain 241), SLEV (strain TBH-28), WNV (strain NY99-35261-11), and ZIKV (strain PRVABC59) as previously described (Beaty et al. 1995). Viruses were obtained from the World Health Organization Center for Arbovirus Reference and Research, which is maintained at the Division of Vector-Borne Infectious Diseases, Centers for Disease Control and Prevention in Fort Collins, Colorado, USA. PRNTs were performed in six-well plates using African green monkey kidney (Vero) cells. Sera were tested at a starting dilution of 1:20 in the presence of 8% labile serum factor (Chappell et al. 1971). Titers were expressed as the reciprocal of serum dilutions yielding ≥90% reduction in the number of plaques (PRNT90). For etiological diagnosis, the PRNT90 antibody titer to the respective virus was required to be at least fourfold greater than that to the other flaviviruses tested. If the PRNT90 titers for two or more viruses were ≥1280, the patient was considered to have a secondary flavivirus infection.
Enzyme-linked immunosorbent assay
Sera were assayed using the Human Dengue Virus NS1 Antigen ELISA Kit (MyBioSource, Inc., San Diego, CA, USA) according to the manufacturer's instructions. Sera were tested at a dilution of 1:15. Optical densities were measured at 450 nm, with calibration standards used to generate standard curves. Sera from patients previously shown to contain or not contain flavivirus NS1 were used as positive and negative controls, respectively (Laredo-Tiscareno et al. 2018). The ELISA is not DENV specific because the NS1 protein contains group-reactive epitopes, for example, there is a highly conserved epitope sequence on the NS1 proteins of DENV and ZIKV (Rocha et al. 2017, Tan et al. 2019). Considerable cross-reactivity was reported when commercial ELISAs based on the NS1 proteins of DENV and ZIKV were used to test sera from PCR-confirmed dengue and Zika patients from Mexico (Zaidi et al. 2020).
Mosquito collections and homogenizations
Adult mosquitoes were collected in several low-income communities within 10 km of Acapulco. All collections were made in October and November 2019 using manual aspirators. Resting mosquitoes were aspirated from shaded areas in public spaces and outside business and private residences. Mosquitoes were transferred alive to the Universidad Autónoma de Guerrero, stored overnight in a −80°C freezer and identified on chill tables. Females were sorted into pools of up to 10 according to species, date and study site, placed into cryostorage vials containing RNAlater (ThermoFisher Scientific, Waltham, MA, USA) and transported on ice packs to Iowa State University. Mosquitoes were rinsed twice in phosphate-buffer saline then transferred to polypropylene round-bottom 5 mL tubes containing Trizol Reagent (ThermoFisher Scientific) and four 4.5-mm-diameter copper-clad steel beads (BB-caliber airgun shot). Tubes were vortexed for 30 s and centrifuged (3000 rpm, 10 min, 4°C) then supernatants were collected and total RNA was extracted as described in the manufacturer's instructions.
RT-PCR and Sanger sequencing
Total RNA was tested by RT-PCR using flavivirus- and DENV-specific primers. The flavivirus group-reactive primers, FU2 and cFD3, target a 845-nt region of the NS5 gene (Kuno et al. 1998). The DENV-specific primers, D1 and D2, recognized all serotypes and target a 511-nt region of the 5′ untranslated region and capsid gene (Lanciotti et al. 1992). Complementary DNAs were generated using Superscript III reverse transcriptase (ThermoFisher Scientific) and PCRs were performed using Taq polymerase (ThermoFisher Scientific). RT-PCR products were purified using the Purelink Gel Extraction Kit (Invitrogen) and sequenced using a 3730x1 DNA sequencer (Applied Biosystems, Foster City, CA, USA).
Results
Acute sera were collected from 639 patients with suspected dengue who lived in low-income communities in the state of Guerrero. Three hundred fifty (54.8%) patients were female and 289 (45.2%) were male. The ages of the patients ranged from 1 to 93 years, with a mean age of 32.9 years. Most patients presented at hospitals and associated outpatient clinics, but others presented at the Universidad Autónoma de Guerrero. The gender ratios and mean ages of patients who presented at the university did not differ significantly from patients who presented at the other performance sites (data not shown). More than half (56.0%) of the patients developed symptoms in September (Table 1).
Illness Onset for All Patients and for NS1-Positive Patients According to Month, Guerrero, 2019
All sera were screened at a dilution of 1:20 by PRNT using DENV-2 to determine if flaviviruses are a common cause of infection in the study area. Antibodies that neutralized DENV-2 were identified in 431 (67.4%) patients. Of these, 242 (56.1%) were female and 189 (43.9%) were male. Seropositivity was not influenced by gender (t-test, p > 0.05). The mean ages of patients with and without flavivirus-specific antibodies (33.4 and 32.0 years, respectively) were similar. Flavivirus-specific antibodies were detected in 54.5% of patients ≤14 years and in 62.3–76.1% of all other patients, but there was no significant association between age and seropositivity (chi-squared test, p > 0.05) (Table 2). Patients who presented at the Universidad Autónoma de Guerrero were significantly more likely to be seropositive compared with patients who presented at the Hospital General Adolfo Prieto, Hospital General Raymundo Abarca Alarcón, and Laboratorio Nobel (pairwise comparisons adjusted using Turkey's method, p = 0.0002). Flavivirus-specific antibodies were detected in 85.7% of patients recruited through the Universidad Autónoma de Guerrero compared with 64.7% of patients who presented elsewhere, ranging from 54.4% to 75.0% for these performance sites (Table 3).
Age Characteristics of Patients with Flavivirus-Specific Antibodies, Guerrero, 2019
Percentage of Patients with Flavivirus-Specific Antibodies According to Performance Site, Guerrero, 2019
CSSATC, Centro de Salud con Servicios Ampliados de Tierra Colorada in Tierra Colorada; HCT, Hospital de la Comunidad de Tixtla in Tixtla; HGAP, Hospital General Adolfo Prieto in Taxco de Alarcón; HGRAA, Hospital General Raymundo Abarca Alarcón in Chilpancingo; LLA, Labymedic Laboratorios in Acapulco; LNZ, Laboratorio Nobel in Zumpango; UAGroCh, Universidad Autónoma de Guerrero in Chilpancingo.
Sera from 263 seropositive patients were randomly selected and further tested for flavivirus NS1 by ELISA to identify those with acute flavivirus infections. Forty-eight (18.3%) sera contained virus antigen (Table 1). Almost half of the patients with NS1-positive sera developed symptoms in September. All NS1-positive sera were titrated and further tested by PRNT using all four DENV serotypes, SLEV, WNV and ZIKV. Seven patients were seropositive for DENV-1, five patients were seropositive for DENV-2, one patient was seropositive for DENV-3, and two patients each were seropositive for DENV-4 and ZIKV (Table 4). Nineteen patients had secondary flavivirus infections and 15 patients had antibodies to an undetermined flavivirus. Comparative PRNTs were also performed on 60 randomly selected NS1-negative sera. Nine patients were seropositive for DENV-2, three patients were seropositive for DENV-3, and six patients were seropositive for ZIKV. Of the remainder, 18 patients had secondary flavivirus infections and 24 patients had antibodies to an undetermined flavivirus.
Demographic and Plaque Reduction Neutralization Test Data for Patients with Acute Dengue and Zika Virus Infections
Performance site abbreviations are defined in Table 3.
Less than 20.
DENV-1, dengue virus-1; DENV-2, dengue virus-2; DENV-3, dengue virus-3; DENV-4, dengue virus-4; F, female; M, male; PRNT, plaque reduction neutralization test; SLEV, St Louis encephalitis virus; WNV, West Nile virus; ZIKV, Zika virus.
A total of 830 adult female mosquitoes were collected in October and November 2019 in low-income communities surrounding the city of Acapulco. Of these, 736 mosquitoes were identified as A. aegypti and 94 mosquitoes were identified as Culex quinquefasciatus. Mosquitoes were sorted into 203 pools (183 pools of A. aegypti and 20 pools of C. quinquefasciatus) and assayed by RT-PCR using flavivirus- and DENV-specific primers. Three pools of A. aegypti yielded amplification products, testing positive with both primer pairs. The RT-PCR products generated with the DENV-specific primers were sequenced, revealing that the mosquitoes had been infected with DENV-2 (GenBank acc. no. MW134528–MW134530). The sequences were identical to each other and to the corresponding genomic regions of multiple DENV-2 genome sequences in the GenBank database. Virus isolation was not attempted because the mosquitoes were transported in RNAlater. The DENV-2 minimum infection rate, expressed as the number of RT-PCR positive mosquito pools per 1000 mosquitoes tested, for A. aegypti was 4.1.
Discussion
We report the concurrent circulation of all four DENV serotypes and ZIKV in Guerrero, Mexico, in 2019. Our clinical investigation revealed that all these viruses were associated with acute infections in humans in the study area. The sample population consisted exclusively of individuals from impoverished communities with inadequate access to health care. We targeted a population poorly represented by the national DENV and ZIKV surveillance and diagnosis programs to determine whether flaviviruses are commonly associated with illness in low-income areas and to identify flaviviruses that could be circulating undetected. Mosquitoes from select low-income communities were also tested for evidence of flavivirus infection, with DENV-2 RNA detected in A. aegypti.
The Secretariat of Health reported 906 confirmed cases of dengue in Guerrero in 2019, with an incidence of 24.9 cases per 100,000 inhabitants (Anonymous 2019a). Another 490 confirmed cases occurred in Guerrero in 2020, as of the end of EW 40, with an incidence of 13.4 cases per 100,000 inhabitants (Anonymous 2020b). In both years, DENV-2 was the dominant serotype. DENV-1, but not DENV-3 or DENV-4, also detected. The Secretariat of Health last reported DENV-3 and DENV-4 in Guerrero in 2017 and 2016, respectively, with the co-circulation of all four serotypes last detected in 2016 (Anonymous 2016, 2017). We, therefore, provide evidence that DENV-3 and DENV-4 were circulating undetected in Guerrero in 2019. Concurrent circulation of all DENV serotypes was documented in two other states, Chiapas and Veracruz, in 2019 and in at least three states, Nuevo Leon, Tabasco, and Veracruz, in 2020 (Anonymous 2019a, 2020b). Simultaneous circulation of all DENV serotypes has been reported in many other countries, including those in Asia, the Caribbean, Central America, and South America (Suwandono et al. 2006, Bharaj et al. 2008, Mishra et al. 2017, Ramos-Castaneda et al. 2017, Shrivastava et al. 2018, Hamel et al. 2019).
The serotypes most frequently detected in the study area were DENV-1 and DENV-2. Other clinical and serological investigations performed in Mexico in the past two decades have also identified DENV-1 and DENV-2 as the serotypes most commonly associated with human disease and infections (Lorono-Pino et al. 2004, Brunkard et al. 2007, Rodriguez Mde et al. 2010, Dantes et al. 2014, Anonymous 2016, 2017, 2019a, 2020b, Serrano-Pinto and Moreno-Legorretara 2017, Laredo-Tiscareno et al. 2018, Palermo et al. 2019). A review of the nationwide surveillance data revealed that DENV-1 and DENV-2 were the dominant serotypes in Mexico from 2000 to 2011 (Dantes et al. 2014). In another study, a dual DENV-1 and DENV-2 infection was detected in a patient in Colima, Mexico, in 2009 (Espinoza-Gomez et al. 2017). Although DENV-1 and DENV-2 have remained the dominant genotypes in Mexico in the past two decades, frequent lineage replacement has occurred within serotypes (Carrillo-Valenzo et al. 2010).
Flavivirus-specific antibodies were detected in 67.4% of patients in the sample population, ranging from 54.5% to 76.1% among age categories, although these differences were not significant. Other studies performed in Mexico have also reported a high seroprevalence for flaviviruses in humans (Navarrete-Espinosa et al. 2006, Brunkard et al. 2007, Ramos et al. 2008, Rodriguez Mde et al. 2010, Pavia-Ruz et al. 2018). Antibodies to flaviviruses were detected by IgG ELISA in 78.3% of study participants (≥15 years) in a household serosurvey in Tamaulipas in 2004, ranging from 72% to 90% among age groups (Brunkard et al. 2007). In another study, antibodies to flaviviruses were detected by IgG ELISA in 57.3% of febrile patients (≥1 year) in Nuevo Leon in 2005 to 2007 (Rodriguez Mde et al. 2010). Many of the flavivirus antigen-positive patients in our sample population developed symptoms in September. These findings were not unexpected because peak rainfall occurs in Guerrero in June and September. It is well documented that rainfall is positively associated with flavivirus illness, with cases usually peaking 2–3 months after heavy rainfall (Ramachandran et al. 2016, Silva et al. 2016, Santos et al. 2019).
The first autochthonous cases of ZIKV in Mexico occurred in Nuevo Leon and Chiapas in November 2015 (WHO 2015, Guerbois et al. 2016). Guerrero had the second highest incidence of estimated ZIKV cases in Mexico in 2016 (Grajales-Muniz et al. 2019). The Secretariat of Health has now reported 887 confirmed cases of ZIKV in Guerrero, although none occurred in 2019 or 2020 as of EW 40 (Anonymous 2019b). Laboratory studies have demonstrated that A. aegypti from Guerrero are highly competent vectors of ZIKV, with infection, dissemination, and transmission rates exceeding 93% (Sanchez-Casiano et al. 2020). None of the mosquitoes collected in our study contained ZIKV RNA, although two patients had acute ZIKV infections. The clinical criteria for a ZIKV infection is the presence of a rash, with or without fever, and at least one of the following: arthralgia, myalgia or nonpurulent conjunctivitis/hyperemia. We were not provided with sufficient medical information to ascertain whether the patients met the clinical criteria of ZIKV. However, both had laboratory-confirmed acute ZIKV infections and thus, we provide evidence that the virus was active in Guerrero in 2019.
Our study has several limitations that should be acknowledged. First, virus isolation could not be attempted. Sera and mosquitoes were transported internationally on ice packs and in RNAlater, respectively, because dry ice is not easily acquired in Guerrero. Second, the health care providers who participated in the study were not willing to provide detailed clinical information because of the time and effort required to retrieve these data from their medical records. Therefore, dengue patients could not be classified into disease categories, ZIKV cases could not be conclusively identified, and patient outcomes cannot be discussed. In addition, the availability of paired sera would have strengthened the study.
Conclusion
We provide evidence for the concurrent circulation of all four DENV serotypes and ZIKV in Guerrero in 2019. All five viruses were associated with acute infections in humans, with DENV-2 RNA detected in mosquitoes. The Secretariat of Health did not report any cases of DENV-3, DENV-4, or ZIKV in Guerrero in 2019. Therefore, our findings suggest that several flaviviruses of major public health significance were circulating undetected in Guerrero during this time.
Footnotes
Acknowledgments
The authors thank Mayre Sanchez, Jonathan Cisneros, Milton Cisneros, and Jose Alfredo Basilio for assisting with the sera collections.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This study was supported by a postdoctoral scholarship from the from the Consejo Nacional de Ciencia y Tecnología of Mexico (Scholarship No. 406531) an intramural funds provided by the College of Veterinary Medicine at Iowa State University.