
Abstract
Background:
Camel-to-human transmission of the Middle East Respiratory Syndrome coronavirus (MERS-CoV) was confirmed as a cause of primary infection in humans. There is a dearth of information regarding the behavior of the virus in camels and the mode of spread among them under natural conditions. The aim of this study was to monitor exposure of camels to the MERS-CoV under field conditions.
Methods:
From January 1 to November 30, 2015, a secluded herd of 20 pregnant female camels and their neonate calves was established. Nasal and rectal swabs were collected from calves daily for 90 days after birth, then weekly until the end of the study. Nasal and rectal samples were collected from the dams at outset and then weekly until the end of the study. The samples were tested with rtRT-PCR to detect the MERS-CoV RNA.
Results:
All purchased pregnant camels were MERS-CoV RNA negative at outset. Nineteen dams and 15 calves completed the study. Seven (46.7%) of the 15 calves developed a rise in rectal temperature (39–40°C), shivering, rhinitis, anorexia, and general weakness at a mean ± standard deviation of 18.9 ± 4.9 days of age and their MERS-CoV RNA test was positive on the first day of illness. Three of the seven infected calves died 14 ± 9.1 days postonset of illness at age 17, 14, and 46 days, respectively. The remaining four infected calves fully recovered and they were MERS-CoV RNA positive for 17.5 ± 8.8 days. Four (21.1%) of the 19 dams had positive tests; three dams had no clinical signs, whereas the fourth dam exhibited signs not compatible with MERS-CoV infection and died three days after the positive test, 33 days after parturition. All MERS-CoV infections occurred within 22 days.
Conclusions:
This study has expanded our understanding of the MERS-CoV epidemiology among camels, which is an important step forward to device effective preventive measures.
Introduction
The Middle East respiratory syndrome coronavirus (MERS-CoV) is a respiratory pathogen that was first identified in Saudi Arabia in June 2012 (Zaki et al. 2013). MERS-CoV causes acute respiratory disease that has a high case fatality rate (Arwady et al. 2016). All cases have been linked to countries in or near the Arabian Peninsula with more than 85% of cases reported from Saudi Arabia (WHO 2015). A large outbreak reported in 2015 in health care settings in South Korea was also linked to a traveler returning from a visit to four gulf countries in the Middle East, namely, Bahrain, United Arab Emirates, Saudi Arabia, and Qatar (Choi 2015, Ki 2015).
Outbreaks of MERS-CoV have been associated primarily with transmission in health care settings (Assiri et al. 2013, Al-Abdallat et al. 2014, Choi 2015, Ki 2015, Oboho et al. 2015). Transmission among household contacts of patients has been documented but sustained human-to-human transmission has not been described (Arwady et al. 2016).
The seroprevalence of MERS-CoV antibodies in the general population in Saudi Arabia is low (Müller et al. 2015). Strategies to prevent and control infection are recommended to limit secondary transmission in health care settings and among household contacts (WHO 2013, 2014, Madani 2014, Madani et al. 2014). MERS-CoV cases continue to be reported in Saudi Arabia in health care settings as well as in the community (Arwady et al. 2016).
The first record of coronavirus (CoV) infection was made in chickens in 1930 in the United States. The virus was identified as the infectious bronchitis virus of chicken. Later, CoVs were identified as a cause of gastroenteritis and respiratory infections in different species of livestock and other animal species (Khamassi Khbou et al. 2021). The first human coronavirus (HCoV), currently known as HCoV 229E, was isolated in 1960 from patients with common cold symptoms (Kenney et al. 2021). To date, seven HCoVs have been identified, namely, 229E, NL63, HKU1, OC43, severe acute respiratory syndrome (SARS)-CoV, MERS-CoV, and SARS-CoV-2 (Kenney et al. 2021).
Animals have been suspected as a source of primary MERS-CoV infection given the similarities to SARS CoV, a zoonosis known to cause human respiratory disease, often severe, with sustained human-to-human transmission and amplification in health care settings (Peiris et al. 2003, Drosten et al. 2014). In the initial search for the likely animal source of MERS-CoV, it was noticed that patients with primary MERS-CoV infection had exposure to dromedary camels (Camelus dromedarius).
Subsequent serologic studies from the Arabian Peninsula confirmed high seroprevalence of MERS-CoV neutralizing antibodies in dromedaries (Hemida et al. 2013, 2017, Reusken et al. 2013, Briese et al. 2014, Meyer et al. 2014). Other studies also detected partial genome sequences of MERS-CoV from dromedary specimens (Nowotny and Kolodziejek 2013, Haagmans et al. 2014, Raj et al. 2014). More recently infectious MERS-CoV from dromedaries was detected (Azhar et al. 2014, Chu et al. 2014, Hemida et al. 2014). Finally, camel-to-human transmission of MERS-CoV was unequivocally confirmed (Azhar et al. 2014). There is still a dearth of information regarding the behavior of the virus in camels and the mode of spread among them under natural conditions. The present study employed secluded neonate camels and their dams as sentinel animals to understand the pattern of infection and spread, clinical signs, and epidemiological aspects of the natural MERS-CoV infection in camels.
Materials and Methods
Establishment of a secluded camel herd
Twenty pregnant female camels, at their late stage of pregnancy, were purchased from the local markets on January 1, 2015, and kept in a dedicated barn 38 Km south of Jeddah, Saudi Arabia. They were supplied with water and food comprising alfalfa and Rhodes grass hay, ad libitum, and put under close veterinary medical care. Experienced veterinarians supervised their parturition to ensure safe delivery of the neonates, followed the health conditions of the dams and their calves, and supplemented them with all the necessary nutritives and other requirements. The dams and their newborn calves constituted the sentinel herd. The study extended from January 1 to November 30, 2015.
Samples collected
Nasal and rectal swabs were collected from each calf on the day of birth, then daily for 90 days, and then weekly until the end of the study. Nasal and rectal samples were also collected from the dams weekly until the end of the study. Milk samples were collected from the dams on the day of parturition, then daily for 7 days, and then monthly until the end of the study. Serum samples were collected from the female camels upon their arrival to the barn and from the calves upon their birth and then monthly from both until the end of the study for detection of serum MERS-CoV antibodies. No environmental samples were collected from the barn for MERS-CoV RNA testing before the camels were placed.
Real-time transverse transcriptase polymerase chain reaction
RNA was extracted from the nasal and rectal swabs and milk specimens using the QIAamp Viral RNA Mini Kit (Qiagen) according to the manufacturer's instructions. Eluted RNA was screened for the MERS-CoV upstream region of the E gene (upE region) and confirmed by targeting the open reading frame region ORF1a and ORF1b with the use of real-time RT-PCR, as previously described by Corman et al. (2012). Further confirmation was performed by partially sequencing the RNA-dependent RNA polymerase (RdRp) and nucleocapsid (N) regions of the viral genome, as recommended by the World Health Organization (WHO, 2013). Both assays were conducted on specimens collected from the camels.
All RT-PCR reactions were performed in a well-controlled biosafety environment to avoid the risk of RT-PCR contamination. RT-PCR was performed in a three-room laboratory with workflow maintained from the clean to the less clean area.
Serum neutralization antibody assay
The serum neutralization test (SNT) for detection of the MERS CoV antibodies in the camels' sera was performed as described by Lau et al. (2020). The test was performed in tissue culture microtiter plates incubating serially diluted camel sera with 102 median tissue culture infective dose (TCID50) per mL of MERS-CoV (Azhar et al. 2014) for 2 h before adding to the Vero cell monolayers and incubating for 1 h at 37°C. This was followed by adding Minimum Essential Medium maintenance medium (containing 2% fetal calf serum) and further incubating at 37°C. The infected Vero cells were examined daily for 5 days for any cytopathic effect (CPE), and the sera were regarded as positive for neutralizing antibody if no CPE was observed. All tests were performed in triplicate.
Ethics approval
The National Committee of BioEthics (NCBE, 2016) at King Abdulaziz City for Science and Technology and King Abdulaziz University's policies on the care and use of animals were followed. Ethics approval was obtained from the Research Ethics Committee at the Faculty of Medicine, King Abdulaziz University, Jeddah, and the Ministry of Health, Riyadh, Saudi Arabia (Reference number 26921 [animal study]).
Results
The 20 purchased pregnant female camels were MERS-CoV RNA negative at the outset of the study. Of the 20 pregnant female camels, one aborted, two delivered stillbirths, and the remaining 17 camels delivered 17 calves. Two of the 17 newborn calves were weak and having scours and then died at three and five days of age. The one aborted and two stillborn calves, the two calves that died at three and five days of age, and their respective dams tested negative for the MERS CoV RNA.
One dam died after giving birth to a healthy calf as a result of a snake bite and was MERS-CoV RNA negative on the day of death. The remaining 19 dams and 15 calves were kept as a secluded sentinel herd in the present study. Each member of the 34 camels was kept under close clinical observations to identify any signs of disease. Figure 1 shows a summary of the outcome and MERS-CoV RNA testing results of the 20 pregnant female camels and their newborn calves.
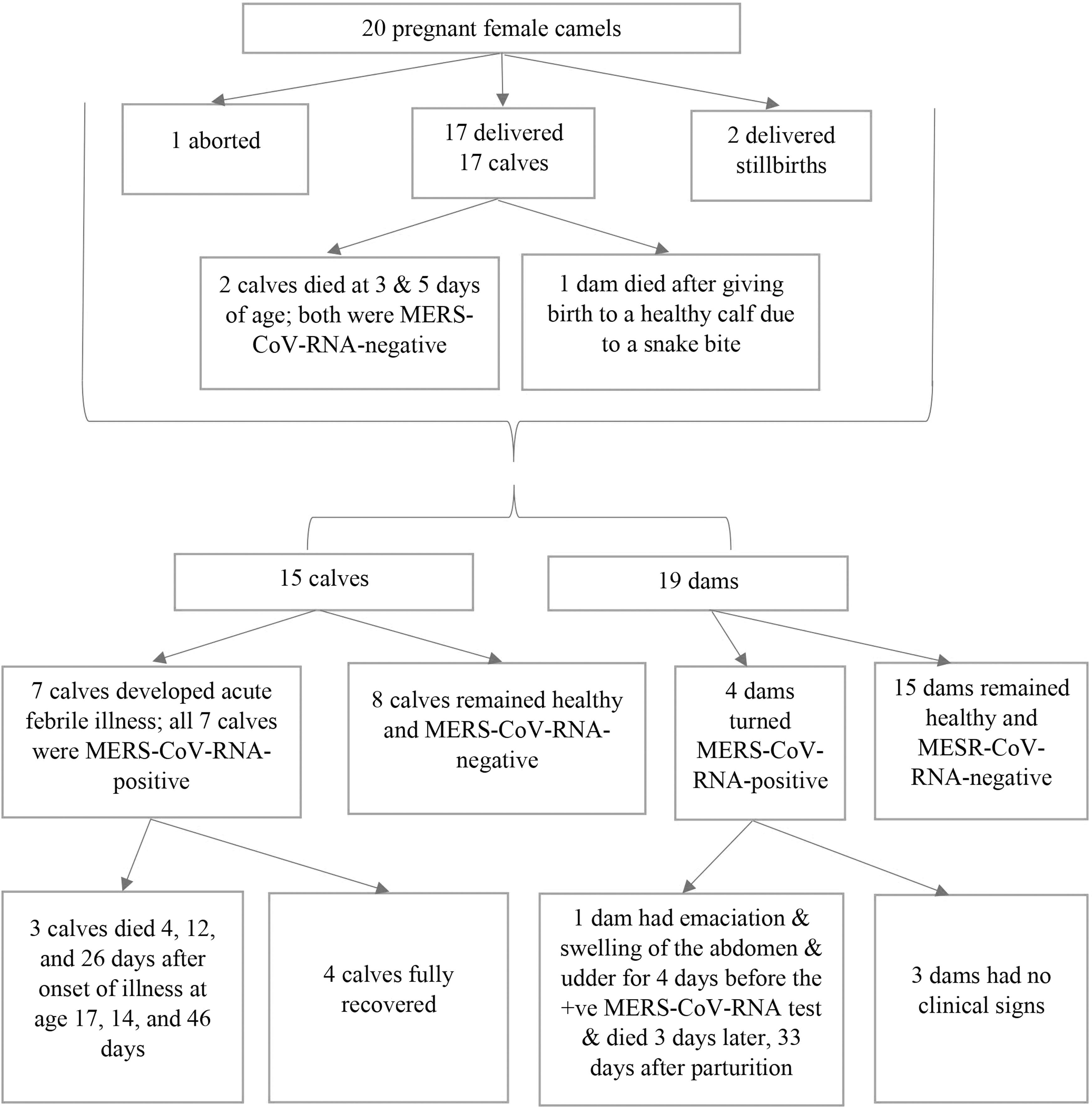
Summary of the outcome and MERS-CoV-RNA testing results of the 20 pregnant female camels and their newborn calves. MERS-CoV, Middle East respiratory syndrome coronavirus.
Table 1 shows a summary of the MERS-CoV RT-PCR results, morbidity, mortality, and case fatality rates of the secluded camels during the study period. Table 2 shows details of the results of the samples that were positive for MERS-CoV RNA among the infected camels, the chronological order of MERS-CoV infection among the herd, the age at primary infection, duration of sickness, and outcome of each sick camel.
Middle East Respiratory Syndrome Coronavirus rtRT-PCR Results, Morbidity, Mortality, and Case Fatality Rates of the Secluded Camels During the Study Period
Morbidity rate: number of MERS-CoV PCR-positive camels/total number of camels tested × 100.
Mortality rate: number of deceased camels that were MERS-CoV PCR positive/total number of camels tested × 100.
Case fatality rate: number of deceased camels that were MERS-CoV PCR positive/total number of camels that were MERS-CoV PCR positive × 100.
Characteristics of Middle East Respiratory Syndrome Coronavirus Infection in 11 Secluded Camels with Laboratory-Confirmed Middle East Respiratory Syndrome Coronavirus Infection
Mean ± SD age at primary infection (first positive MERS-CoV PCR) of the seven calves = 18.9 ± 4.9 days.
Mean ± SD duration of the clinical MERS-CoV disease of the seven sick calves = 16 ± 9.1 days.
Mean ± SD duration of the clinical disease of the four recovered calves = 17.5 ± 8.8 days.
Mean ± SD duration of the clinical MERS-CoV disease of the three deceased calves = 14 ± 9.1 days.
Mean ± SD age at death of the three MERS-CoV-infected deceased calves = 25.7 ± 14.4 days.
Mean ± SD duration of reinfection of the four calves that had reinfection = 14.3 ± 5.9 days.
As per routine schedule of sampling, the MERS-CoV RNA was detected in the collected samples from the secluded camels.
Before parturition.
After parturition.
NCD, no clinical disease; SD, standard deviation.
During the routine sampling, seven (46.7%) of the 15 calves developed a rise in rectal temperature (39–40°C), shivering, rhinitis, anorexia, and general weakness at 2, 13, 17 (each of 2 calves), 20, 27, and 36 days of age. All of these seven symptomatic calves were MERS-CoV RNA positive on the day of onset of clinical symptoms. All nasal swabs and only three rectal swabs from these seven calves were MERS-CoV RNA positive. Three of the seven infected calves were sick until their death 4, 12, and 26 days after the onset of disease (mean ± standard deviation of 14 ± 9.1 days) at age 17, 14, and 46 days, respectively.
MERS-CoV RNA was not detected from these three calves after their initial positive tests until their death. Necropsy to determine the macroscopic and microscopic pathology and virus loads in various organ systems was not performed. The remaining four infected calves fully recovered after 21, 15, 29, and 5 days of illness, respectively (mean ± standard deviation of 17.5 ± 8.8 days). The remaining eight noninfected calves remained healthy and MERS-CoV RNA negative.
Four (21.1%) of the 19 dams had positive MERS-CoV RT-PCR tests. Three of the four MERS-CoV RT-PCR-positive dams did not show any clinical signs of illness. The fourth dam had emaciation and swelling of the abdomen, the udder, and the flanks for 4 days before the MERS-CoV RNA-positive result and died three days later, 33 days after parturition. No respiratory signs were observed in this dam or in any of the other MERS-CoV RNA-positive dams (Table 2).
All (100%) nasal samples and only three (27.3%) rectal samples collected from the 11 infected camels (7 calves and 4 dams) were MERS-CoV RNA positive. The three positive rectal samples were all from the calves and none of the rectal samples from the infected dams was positive. All milk samples were negative for MERS-CoV RNA.
All the female camels were MERS-CoV RNA negative at the outset of the study on January 1, 2015, and remained so for up to 38 days thereafter. On the 39th day (February 9, 2015) of the study, one female camel turned MERS-CoV RNA positive and this was considered to be the index case (Fig. 2). One day later (February 10, 2015), a calf turned MERS-CoV RNA positive. A week later (February 17, 2015), three more calves turned MERS-CoV RNA positive. Nine days later (February 26, 2015, i.e., day 57 of the study), one female camel and six calves turned MERS-CoV RNA positive. On March 2, 2015 (day 61 of the study), two female camels turned MERS-CoV RNA positive. Thus, within 22 days (February 9, 2015 to the March 2, 2015) four female camels and seven calves were infected with MERS-CoV.
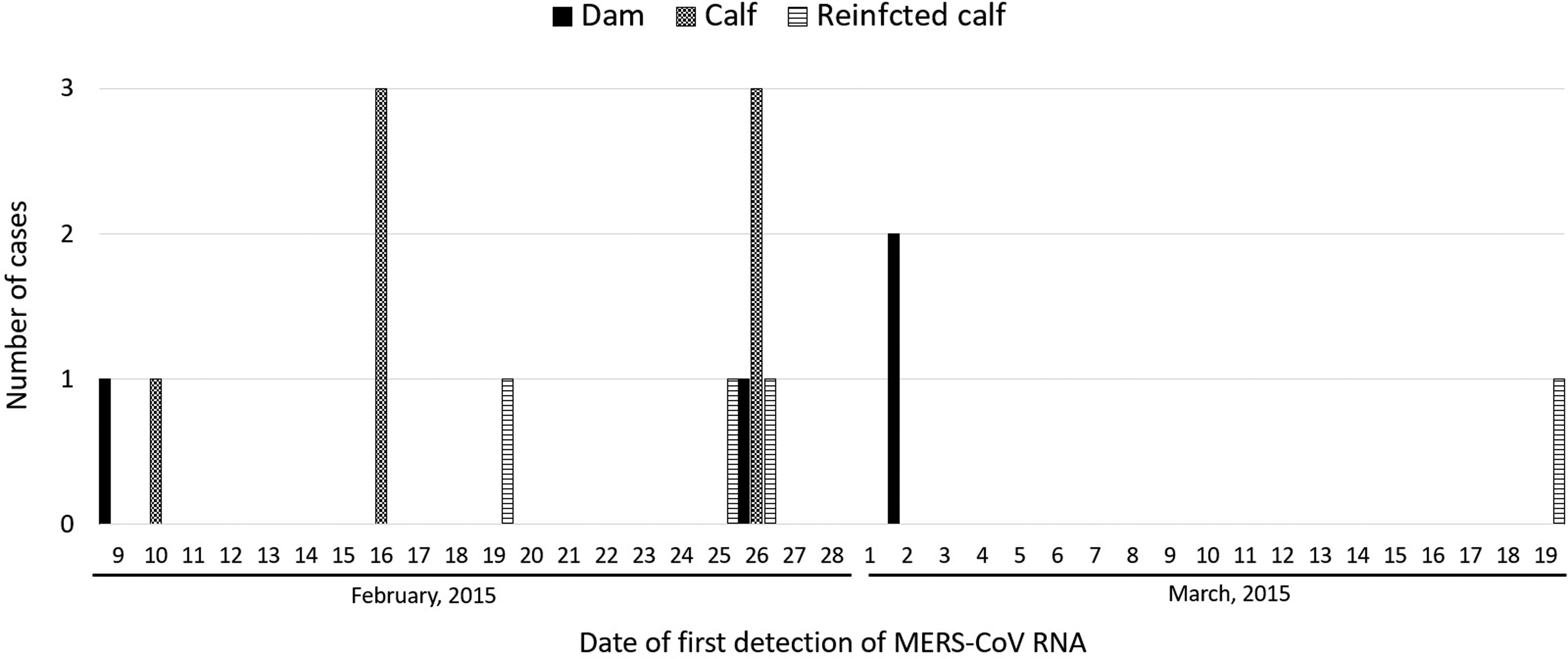
The number of first MERS-CoV infections and reinfections by date of onset among 4 dams and 7 calves that were part of a secluded camel herd of 19 dams and 15 calves from January 1, 2015 until November 30, 2015.
It was also observed that, four calves of the 11 infected camels (36.4%) turned MERS-CoV RNA negative, and then positive again (reinfected) in a mean time of 14.3 ± 5.9 days (Fig. 2 and Table 2). MERS-CoV RNA was not detected between the two positive results. The remaining female camels and calves in the herd remained MERS-CoV RNA negative throughout the study period. Table 3 shows the cycle threshold values of the four reinfected calves.
The Cycle Threshold Values of the Four Reinfected Calves
No MERS-CoV RNA was detected between the primary infection and reinfection.
CT, cycle threshold.
All the pregnant camels were seropositive for MERS-CoV antibodies at the time of purchase with a mean reciprocal SNT antibody titer of 745. The preinfection mean reciprocal SNT antibody titer of the four infected dams was 587. Excluding the infected dam that died, the mean reciprocal SNT antibody titer of the remaining three infected dams was 1387 a month after the infection. All the dams, including the three dams that recovered, were subsequently tested for SNT antibodies every month until the end of the study (9 months). The monthly mean reciprocal SNT antibody titers were as follows: 1320, 1240, 1310, 1480, 946, 1600, 1013, 960, and 960, with a mean titer of 1203. The preinfection mean reciprocal SNT antibody titer of all the calves was 99. The postinfection monthly mean reciprocal SNT antibody titers were as follows: 265, 406, 71, 166, 584, 40, 220, and 840, with a mean titer of 324. The milk was negative for serum-neutralizing MERS-CoV antibodies.
Table 4 shows a comparison between the natural MERS-CoV infection in our sentinel camels and the experimental infection reported by Adney et al. (2014).
Comparison Between Middle East Respiratory Syndrome Coronavirus Natural and Experimental Infection of Dromedary Camels
Data on experimental infection of dromedary camels with MERS-CoV were obtained from the work done by Adney et al. (2014).
One dam that died 33 days after parturition had clinical manifestations not compatible with MERS-CoV infection before turning positive for MERS-CoV 3 days before its death. Therefore, its death could not be attributed, solely, to the MERS-CoV infection (see Discussion section).
Discussion
To ensure that the secluded camel calves were completely naive to the MERS-CoV in this study, pregnant female camels at their late stage of pregnancy were procured and their parturitions were supervised to get naive newborn camel calves that were used along with the dams as a sentinel herd. Like other camel herds in Saudi Arabia, the secluded camel herd in this study was kept in the field without interference to ensure natural exposure, if any, to the MERS-CoV. Similar to other camel herds in the vicinity of our study barn, water and feeds comprising alfalfa and Rhodes grass hay were provided to our study camels ad libitum and the camels were left to wander inside the barn freely.
Both dams and calves were infected indicating that any susceptible camel, regardless of age, can be infected with the MERS-CoV. However, the calves experienced higher morbidity, mortality, and case fatality rates (46.7%, 20%, and 42.9%, respectively), as compared with the rates observed for the camel dams (21.1%, 5.3%, and 25%, respectively). The higher morbidity, mortality, and case fatality rates of the calves might be explained by the fact that camel neonates are known to be born devoid of circulating antibodies (Abd-Elnaeim et al. 1999). Female camels have a diffuse epitheliochorial type of placentation that does not allow passage of maternal antibodies to the fetus (Abd-Elnaeim et al. 1999). Accordingly, neonates are born vulnerable to infection and they depend solely on the colostral antibodies to acquire passive immunity against infections. The neonates have to suckle within the first 24–48 h of birth, otherwise a phenomenon known as “intestinal closure” will supervene and prevent absorption of colostrum, thus increasing the vulnerability of the neonates to infection (Sangild 2003). However, in many cases, the colostrum may not contain antibodies against specific pathogens, may contain low level of antibodies to protect the neonates, or the ingested colostral antibodies may not be protective altogether. In such a situation, the neonate will be vulnerable to infection as seemed to be the case with the calves in the present study.
All the pregnant camels were seropositive for MERS-CoV antibodies with a moderate mean reciprocal SNT antibody titer (745) at the outset of the study. The moderately high preinfection mean reciprocal SNT antibody titer (587) of the four infected dams might have conferred some degree of protection to the three dams that tested MERS-CoV RNA positive without showing clinical signs. The fourth dam that showed overt clinical disease likely had a secondary infection that compromised its immunity and led to death. Interestingly, the 15 MERS-CoV RNA-negative dams had a rise in the mean reciprocal SNT antibody titer (1203) a month after infection of the index dam despite having negative MERS-CoV RNA suggesting a subclinical infection associated with an anamnestic immune response in these MERS-CoV RNA-negative camels.
The preinfection mean reciprocal SNT antibody titer of all the calves was low (mean of 99), denoting their vulnerability to the MERS-CoV infection. The postinfection monthly titers of all calves (mean of 324) indicated that their antibody levels had risen, on average, three-folds after the infection.
All primary MERS-CoV infections and reinfections among the camel herd occurred within 22 days, except for one reinfection that occurred 39 days after the onset of this outbreak. No MERS-CoV RNA was subsequently detected in any of the dams or calves until the end of the study. Thus, it seems that the high reciprocal SNT antibody titers detected in the herd after the outbreak conferred immunity to the members of the herd and prevented reinfection until the end of the study.
As shown in Table 2, the spread of the MERS-CoV among the study herd occurred within 22 days, resulting in a morbidity rate of 32.4%. This high rate indicates that close contact between members of the herd during eating or drinking and the intimate contact between the calves and dams and the kissing behavior could have resulted in this rapid spread of the virus among the susceptible members of the study herd. It would be of interest to trace the source of infection of the index case in this study.
Genome sequencing of the MERS-CoV detected in the infected female camels and calves that was not performed in this study, could have helped in understanding better how the virus spread among the herd. The study herd was located within an area that was allocated by the municipality to be used for keeping camel herds. The feed suppliers visited many herds in the area, and could have acted as a means of spreading the infection. The aerosol mode of transmission could not be excluded although it was not found to be highly significant under experimental conditions (Adney et al. 2014). The possible social visits between the shepherd of the study herd and his friends who tended other camel herds in the vicinity might have also played a role in spreading the virus to the study herd.
The age of the calves that were infected with the MERS-CoV ranged from 2 to 36 days with a mean of 18.9 days. Thus, the infected calves were prone to infection from early age. One calf was infected at two days of age indicating that it was devoid of maternal antibodies and did not have time to consume enough colostrum before infection. However, it seemed that the range of the time span for the calves to become infected depended on their close contact with the infected members of the herd. The mean duration of the overt clinical disease in the seven infected and the three deceased calves was 16 and 14 days, respectively. This relatively long illness could have helped in maintaining the virus in the environment.
Adney et al. (2014) reported a mild rise of rectal temperature and rhinorrhea in adult camels experimentally infected with the MERS-CoV. In our study, the dams that were MERS-CoV RNA positive had no rise in temperature or overt clinical signs, except for the deceased dam, which exhibited signs (emaciation and swelling of the abdomen, the udder, and the flanks) not compatible with the signs of MERS-CoV infection reported by Adney et al. (2014). Therefore, the results of our study and that reported by Adney et al., confirmed that adult camels do not develop severe MERS-CoV infection through either natural or experimental infection.
Unlike adult camels, the sick camel calves showed a rise in temperature that reached 39–40°C, which was higher than the normal temperature in camels (35–38°C). Shivering, rhinitis, anorexia, and general weakness were also observed but there was no cough or pneumonia. It was interesting to see that four calves of the 11 infected camels (36.4%) turned RT-PCR negative and then positive again in a mean time of 14.3 ± 5.9 days (Table 2).
MERS-CoV RNA was not detected between the two positive results indicating that the second positive results represented reinfection rather than prolonged shedding of the virus. Three of the four reinfected calves had MERS-CoV RNA-positive nasal and rectal samples during their initial infection. MERS-CoV reinfection of the calves indicated that a single infection may not confer solid immunity and that camel calves can become reinfected and hence maintain the virus longer in the environment. However, following recovery of these sick camel calves, all members of the herd remained healthy and MERS-CoV RNA negative until the end of the study indicating possible solid herd immunity to the challenging field virus.
All nasal samples of the 11 MERS-CoV-infected camels were MERS-CoV RNA positive (100%), but only 27.3% of their corresponding rectal samples were MERS-CoV RNA positive, corroborating previous reports that tropism of the MERS-CoV is toward the respiratory system (Adney et al. 2014). Even though the respiratory tract is the predilected site for MERS-CoV infection in camels, detection of the MERS-CoV RNA in 27.3% of the rectal swabs of the infected camels suggests that MERS-CoV may also be enterotropic targeting the gut.
MERS-CoV RNA was not detected in the milk samples in this study suggesting that viremia, the usual requisite for shedding a virus into the milk, did not occur. This is further supported by other studies where viremia was not reported in adult camels that had been experimentally infected with the MERS-CoV (Adney et al. 2014).
MERS-CoV is a highly infectious virus with high mortality rates. Humans acquire primary MERS-CoV infection through direct or indirect contact with infected camels (Azhar et al. 2014, Alraddadi et al. 2016). Secondary infection occurs through transmission from human to human particularly in health care settings (Oboho et al. 2015).
In the Arabian Peninsula, camels have had a longstanding intimate relationship with humans. Before the availability of automobiles, camels were primarily used as means for transportation, traveling long distances through the deserts, and shipment of cargo. Camels are still extensively used in the Arabian Peninsula for meat and milk consumption, kept as fancy animals, and for the very popular racing and beauty championships. Recently, a camel named “Arnoon” was recorded in the Guinness book of records as the most expensive animal recorded ever (Anon 2021). It is a common practice among camel owners and shepherds to kiss and hug the animal. Such intimate contact and relationship between humans and camels in the Arabian Peninsula was the main cause for the MERS-CoV epidemic that occurred in Saudi Arabia in 2014 (Azhar et al. 2014, Alraddadi et al. 2016).
Many studies have reported on MERS-CoV dynamic interaction between humans and camels but critical knowledge gaps exist regarding the behavior of the virus among camels. With this background, this study attempted to explore the dynamic and epidemiology of the virus among camels. Such information will hopefully have an important positive impact on public health and the design of effective measures to control epidemics and prevent primary MERS-CoV infection and the consequent potential large-scale amplification that may occur in health care settings and the community as a whole.
In conclusion, the use of camel neonates and their dams as sentinel animals in this study provided important insight into the natural exposure of camels to the MERS-CoV under field conditions. The results indicated that MERS-CoV was smoldering in the field where the camel herd was established and that MERS-CoV infection targeted the susceptible camels, regardless of their age group. The results also indicated that the morbidity and mortality rates of the calves were two to three times higher than the rates of the dams. It was also observed that the infected camel calves experienced overt clinical disease, whereas the infected dams showed no clinical disease. The role of camel calves for spreading the MERS-CoV in the environment was apparently more important than adults. Nasal samples for MERS-CoV RT-PCR provided the highest diagnostic yield, while milk samples from the dams were consistently negative for MERS-CoV RNA. It is hoped that this information will help to expand our understanding of the MERS-CoV epidemiology among camels to device effective measures to prevent infection among camels and also from camels to humans.
Footnotes
Acknowledgments
The authors thank the Ministry of Health (MOH), Saudi Arabia, for funding this study and for its logistical support. They particularly thank Mr Ali Alzahrani, Ministry of Health, Jeddah, for facilitating all administrative and logistical activities of the project, including preparation of the barn for keeping the sentinel camel herd, procurement of the pregnant she-camels, arrangement to maintain supplies of camels' feeds, water, medicines, and all other requirements, and for procurement of the reagents for diagnostic tests.
Authors' Contributions
T.A.M. and E.M.E.A. conceived and designed the study, analyzed and interpreted the data, and wrote the article; E.M.E.A., H.S.H., and M.A.B. performed the veterinary assessment and collection of samples; A.M.H. and E.I.A. performed the RT-PCR tests; All authors read and approved the article; T.A.M. is the guarantor of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Ministry of Health, Saudi Arabia, funded this study. The Ministry of Health had no involvement in the study design, in the collection, analysis and interpretation of data, or in the writing of the article.