
Abstract
Background:
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a global pandemic, which has caused unprecedented damage to human health and life. The present study aimed to carry out and discover asymptomatic infected individuals in Shenzhen, China. The data will provide the control measures to stop COVID-19 prevalence.
Methods:
The study was a retrospective review of medical records from 462 confirmed patients with COVID-19 and 45 asymptomatic infected individuals in Shenzhen from January 19 to April 30, 2020; this is a retrospective, observational multicenter study.
Results:
A total of 462 confirmed cases were diagnosed in Shenzhen from January 19 to April 30, 2020. The cohort included 423 domestic cases (91.56%, 95% confidence interval [CI]: 88.67–93.76) and 39 (8.44%, 95% CI: 6.24–11.33) imported cases from other countries. Moreover, a total of 45 asymptomatic infections were found, encompassing 31 (68.89%, 95% CI: 54.34–80.47) local infections and 14 (31.11%, 95% CI: 19.53–45.66) individuals imported from other countries. The proportion of asymptomatic infected persons in Shenzhen is continuously increasing (Z = 13.19, p < 0.0001). The total number of local asymptomatic infections was more than that in other provinces (χ 2 = 118.83, p < 0.0001). The proportion of asymptomatic infected individuals among cases imported from other countries was higher than the domestic cases (χ 2 = 22.51, p < 0.0001, odds ratio = 4.90, 95% CI: 2.40–9.98).
Conclusions:
The proportion of asymptomatic infection is increasing. Hence, development and application of the diagnosis method with high sensitivity and specificity play a critical role in reducing COVID-19 global epidemics.
Introduction
A
COVID-19 asymptomatic infection is one of the most important sources for causing other patient infection with SARS-COV-2 (Wu and McGoogan 2020). It is referred to as those positive in nucleic acid testing with nasopharyngeal swabs but developing no novel coronavirus related symptoms, such as fever, upper respiratory symptoms, fatigue, and gastrointestinal symptoms (Popov et al. 2020, Naik et al. 2021). Hence, they are not referred to as patients due to the lack of symptoms. The primary reasons for asymptomatic infected individuals might be that the infector is yet to develop clinical manifestations in the early stage of the disease or that the individual is immune and does not show any clinical manifestation after SARS-CoV-2 infection (Naik et al. 2021). Due to the absence of clinical symptoms, asymptomatic infection is less prone to discharge their pathogens than confirmed cases and, hence, less prone to spread the virus theoretically (Zhu et al. 2020a).
The asymptomatic infection is the most insidious and leaky source of infection (Wu and McGoogan 2020). Thus, the capability to identify these infections should be improved as the virulent pathogen that would continue to enjoy the unobstructed route of easy transmission (Ren et al. 2021). Owing to less virulence discharge and no clinical symptoms, asymptomatic infection cannot be identified spontaneously, thereby rendering it necessary to improve the detection capability to recognize the asymptomatic infections and control the prevalence of COVID-19. Asymptomatic infections may be identified as follows: among close contacts of COVID-19 cases (Wu and McGoogan 2020), during active detection in the investigation of cluster outbreaks, during active detection of the exposed population when tracing the infection sources of COVID-19 cases, during active detection of COVID-19 cases, and individuals with travel or residential history in regions of constant transmission.
The rapid spread of COVID-19 has posed great challenges to the medical, health care, and social emergency management of regions and countries (Adhikari et al. 2020). The rapid spread threatens the life safety and exerts a significant impact on the economy and society such that no disease has surpassed in the past century, thereby causing great concern for all state governments and sectors of the society. Hence, the present study aimed to identify asymptomatic infected individuals in Shenzhen, China; it would provide scientific reference for the prevention and control of COVID-19.
Materials and Methods
Study design and participants
This study was a retrospective review of medical records from 462 patients with confirmed COVID-19 pneumonia and 45 asymptomatic infected individuals in Shenzhen from January 19 to April 30, 2020. All subjects were diagnosed according to the guidelines for COVID-19 diagnosis and treatment (trial version 7) published by the National Health Commission of the People's Republic of China.
Data collection
The epidemiological investigation reports of all COVID-19 confirmed patients and asymptomatic infections in Shenzhen from January 1 to April 30, 2020 were collected and investigated. The demographic information, date of onset, date of report, date of entry, country or region of residence or travel before entry, the region of the report, track of entry, and course of identification were collected.
All individuals from other countries immediately underwent nucleic acid detection and 14-day isolation observation, after arriving at Shenzhen by flight. In addition, all individuals from other provinces of China who came to Shenzhen underwent COVID-19 nucleic acid test if they were from middle/high epidemic area or had been in close contact with COVID-19 patients, followed by isolation and observation for 14 days.
Definitions of cases and asymptomatic infections
COVID-19 confirmed cases and asymptomatic infections were defined according to the Guidelines on the Prevention and Control of COVID-19 (seventh revision).
COVID-19 suspected cases were defined as those accompanied by epidemiological history and one clinical manifestation as follows: The epidemiological history included (1) travel or residence history in the epidemic area within 14 days before the onset of the disease, (2) individuals who had been exposed to COVID-19 cases in the epidemic area or local area before the onset of the disease and patients who had been exposed to pneumonia symptoms from the origin of the epidemic or from areas where local cases continue to spread. In addition, the clinical manifestations of COVID-19 involve (1) fever, (2) abnormal blood routine examination, that is, the blood cell count and lymphocyte count were normal or decreased, and (3) individuals with imaging features of pneumonia.
COVID-19 confirmed cases were defined as those with the presence of pathogen detected in the sputum, throat swab, and lower respiratory tract secretion from suspected patients; for instance, (1) the nucleic acid test is positive with real-time PCR; (2) the sequencing of the virus gene was highly homologous with the known SARS-CoV-2; and (3) IgM antibodies were positive.
Asymptomatic infection was referred to subjects who without clinical symptoms (such as fever, sore throat, and cough) and respiratory tract specimens are positive for nucleic acid detection or IgM antibody.
Domestic imported cases were referred to those with a travel and residential history in Hubei Province (including Wuhan City) or other provinces of China at 14 days before the onset of symptoms, as well as their contacts. Cases without a travel and residential history in cities other than Shenzhen at 14 days before onset were defined as domestic local cases. In addition, cases imported from other countries were referred to as COVID-19 cases residing in Shenzhen, with a travel and residential history 14 days before the onset and were not defined as the domestic source of infection, according to epidemiological investigations. The local cases were associated with those imported from abroad or had a history of contact with such travelers; however, no defined domestic source of infection was detected by the epidemiological investigations.
In addition, COVID-19 patients and asymptomatic individuals were divided into two stages in this study, according to the strategy periods. One group is the emergency response strategy period of the COVID-19 epidemic in Shenzhen from January 19 to February 12, 2020, another group is the normal prevention and control period of the epidemic of COVID-19 from February 13 to April 30, 2020, and the orderly resumption of work and production was carried out gradually during this period.
Assessment level of risk area
All areas are divided into high risk areas, medium risk areas, and low risk areas by city. The definition of low risk area is where there is no confirmed case or no new confirmed cases for 14 consecutive days. Medium risk area is where new confirmed cases are found within 14 days, and the cumulative confirmed cases are less than 50; in addition there is no cluster epidemic within 2 weeks. The high risk area is where there are more than 50 confirmed cases or there is cluster epidemic in recent 2 weeks. Those classifications are accorded to the Guidelines on the Prevention and Control of COVID-19 (seventh revision).
Statistical analysis
Data were analyzed using SAS® Software (Version 9.4 Copyright© SAS Institute, Inc., Cary, NC) and were used to conduct a statistical analysis. Information of the cases was input and verified in both softwares. Odds ratio (OR) and 95% confidence intervals (CIs) of categorical variables were calculated using two-tailed chi-squared or Fisher's exact test. Significant difference was considered as the level of p < 0.05 with two-tailed test.
Results
Source of the confirmed patients in Shenzhen, China
The first COVID-19 patient was found in Shenzhen on January 19, 2020, and the first COVID-19 case imported from another country was found on March 1, 2020, while the last case was diagnosed on April 30, 2020 (Fig. 1). From January 19 to April 30, 2020, a total of 462 confirmed COVID-19 cases were diagnosed in Shenzhen, China, including 423 domestic patients (91.56%, 95% CI: 88.67–93.76, 423/462) and 39 (8.44%, 95% CI: 6.24–11.33, 39/462) cases imported from other countries. Among the domestic cases (n = 423) identified in Shenzhen, the majority was imported from Hubei Province (73.76%, 95% CI: 69.37–77.73, 312/423), followed by local incidents (16.31%, 95% CI: 13.10–20.13, 69/423) and those imported from other provinces of China (9.93%, 95% CI: 7.43–13.15, 42/423) (Appendix Table A1 and Supplementary Appendix 2).
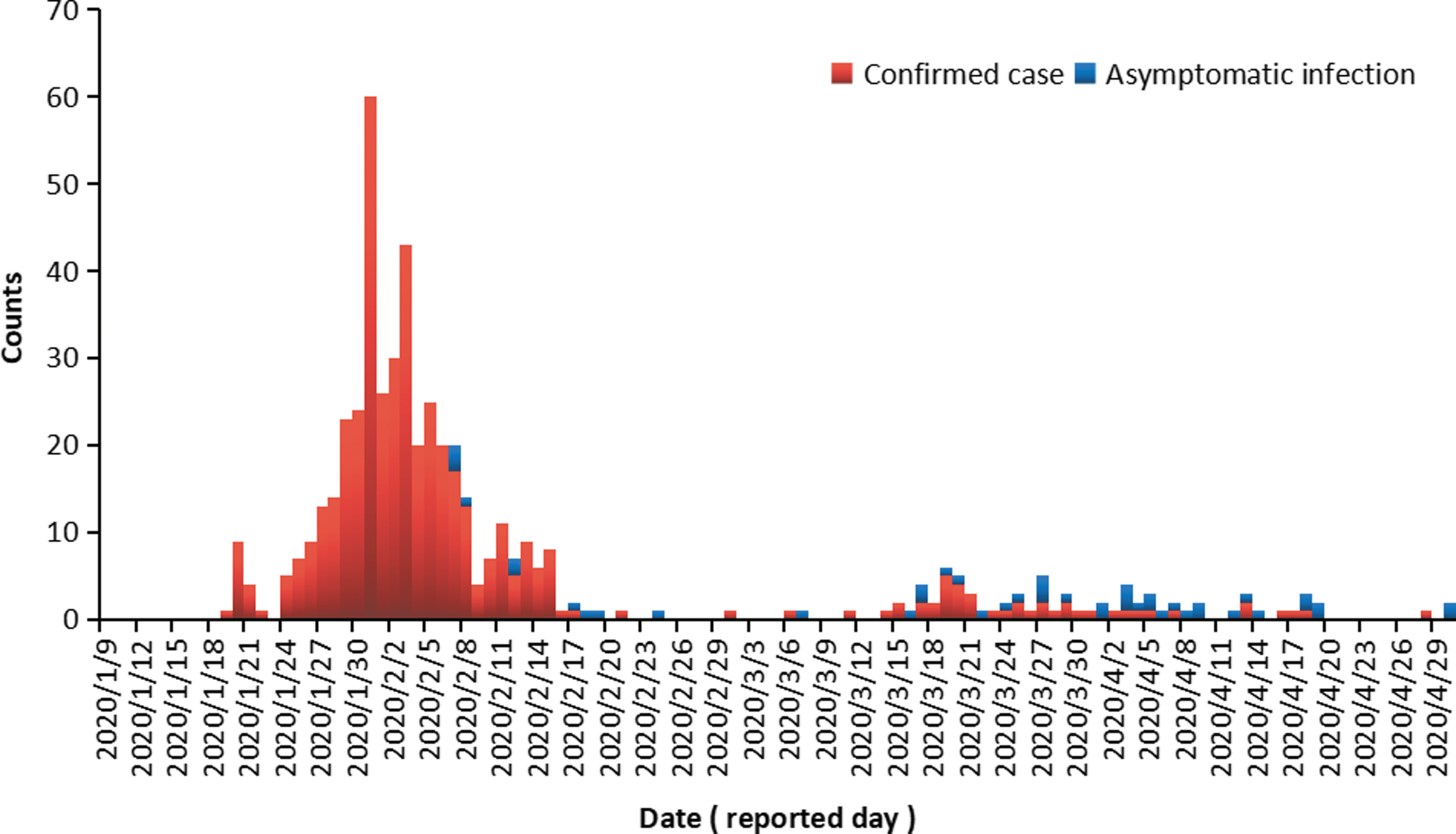
The time trend of COVID-19 confirmed patients and asymptomatic infected individuals in Shenzhen, China. COVID-19, coronavirus disease 2019. Color images are available online.
In this study, conducted from January 19 to April 30, 2020, 393 imported cases, encompassing 354 (90.08%, 95% CI: 86.73–92.66, 354/393) patients from the other cities of China and 39 (9.92%, 95% CI: 7.34–13.23, 39/393) cases from other countries, were detected in Shenzhen. These numbers indicated that COVID-19 patients in Shenzhen were primarily imported cases (85.06%, 95% CI: 81.40–88.12, 393/462), and only 69 were local patients (14.94%, 95% CI: 11.98–18.60, 69/462) caused by imported cases.
From January 19 to February 12, 2020 and from February 13 to April 30, 2020, the epidemiological features of COVID-19 in Shenzhen changed significantly. From January 19 to February 12, 2020, COVID-19 patients were mainly imported from Hubei Province (75.70%), followed by local cases and those imported from other provinces of China (excluding Hubei Province), while none was imported from other countries. However, from February 13 to April 20, 2020, patients imported from other countries accounted for the majority (54.93%) in Shenzhen, followed by those imported from Hubei Province (22.54%) and other provinces of China (excluding Hubei Province) (12.68%), while local cases accounted for only 9.68% of the total number of occurrences (Appendix Table A2). These data further indicated that the intensive community prevention, control measures, other comprehensive blocking strategies, and measures adopted by Shenzhen achieved significant results.
Source of asymptomatic infected individuals in Shenzhen, China
A total of 45 asymptomatic infections were found in Shenzhen from January 19 to April 30, 2020, including 31 local asymptomatic infections (68.89%, 95% CI: 54.34–80.47, 31/45) and 14 asymptomatic individuals imported from other countries (31.11%, 95% CI: 19.53–45.66, 14/45), while no asymptomatic carrier was imported from other cities of China (Appendix Table A2). From January 19 to February 12, 2020, only six (100.00%) local asymptomatic infections were found in Shenzhen, and no asymptomatic individuals were identified from other cities of China and other countries. In contrast, from February 13 to April 30, 2020, the proportion of asymptomatic infections imported from other countries rose to 35.90%. Taken together, the confirmed patients in Shenzhen were mainly imported (85.06%, 95% CI: 81.52–88.02, 393/462) during the epidemic, while the asymptomatic infections were mainly local individuals (68.89%, 95% CI: 54.34–80.47, 31/45), and both were statistically significant (χ 2 = 7.84, p = 0.0051, OR = 2.57, 95% CI: 1.30–5.08) (Appendix Table A3).
Epidemic curve characteristics of confirmed cases and asymptomatic infections in Shenzhen, China
Figure 1 shows that in terms of time distribution (by day), the proportion of asymptomatic infection increases continually (by day) in Shenzhen from January 19 to April 30, 2020 (Z = 13.1888, p < 0.0001). Similarly, the asymptomatic infections also showed a continuously rising trend (Z = 11.79, p < 0.0001) from January to April 2020, while that of the proportion of confirmed cases declined every month. The change in the proportion of asymptomatic infections indicated a statistical significance at the 4-month evaluation (χ 2 = 121.87, p < 0.0001) (Appendix Table 3). Thus, it could be deduced that asymptomatic infections in April accounted for a higher proportion than that in March (χ 2 = 11.99, p = 0.0005, OR = 5.23, 95% CI: 1.99–13.74), February (p < 0.0001, OR = 9.44, 95% CI: 3.84–23.20), and January (p < 0.0001). Moreover, the proportion in March accounted was more than that in February (p < 0.0001, OR = 9.44, 95% CI: 3.84–23.20).
Therefore, the ratio of asymptomatic infections to confirmed patients in Shenzhen was 1:10.27 (45/462). Similarly, the ratio of asymptomatic infections from local and other cities of China to confirmed patients from local and other cities of China was 1:13.65 (31/423) and that of the asymptomatic infected individuals imported from other countries to confirmed cases from other nations was 1:2.79 (14/39). The proportion of asymptomatic infections to confirmed patients in individuals imported from other countries was higher compared with individuals from local and other cities of China (χ 2 = 22.51, p < 0.0001, OR = 4.90, 95% CI: 2.40–9.98).
Distribution features of imported patients and asymptomatic infected individuals from other countries
The first confirmed case imported from other countries was identified in Shenzhen on March 1, 2020. Finally, 39 confirmed patients and 14 asymptomatic infected individuals were imported from other countries until April 30, 2020 (Appendix Table A4). The primary source nations of confirmed cases and asymptomatic infected individuals were the United Kingdom, the United States, and France (Fig. 2). The proportion of asymptomatic patients imported from different countries was not significant (χ 2 = 7.72, p = 0.66).

The source nations of confirmed patients and asymptomatic infected individuals in Shenzhen, China. Color images are available online.
In terms of time trend, the number of asymptomatic infections in Shenzhen imported from other countries did not decrease or increase daily (Z = 1.20, p = 0.23), but the proportion of asymptomatic infected individuals increased significantly in April. In addition, the number of patients imported from other countries in April (45.45%, 95% CI: 21.27–71.99, 5/11) and March (21.4%, 95% CI: 11.71–35.94, 9/42) did not differ significantly (χ 2 = 2.40, p = 0.12, OR = 0.33, 95% CI: 0.08–1.32).
Discussion
The present study performed a descriptive and exploratory analysis of COVID-19 confirmed patients and asymptomatic infections in Shenzhen, China; it demonstrated that the spread of infection was mainly through two stages, the early stage in which the cases were mainly those imported from the Hubei Province of China, and the late stage in which the cases were mainly those imported from other countries, while local cases were at a low level of incidence and prevalence (Wan et al. 2020). As of January 14, 2020, when the first suspected case was reported, the confirmed cases imported from Hubei Province accounted for 75.70% of all the confirmed cases in the early stage (296/391), while the same accounted for only 22.54% in the late stage. It indicated that the control measures of the Wuhan city (from January 22, 2020 onward) reduced the risk of an increase in the number of cases in other cities of China, thereby decreasing the pressure of prevention and control the COVID-19 in other cities (Prem et al. 2020).
The number of confirmed cases in Shenzhen imported from other provinces of China (excepting Hubei Province) in the late stage (12.68%) was more than that in the early stage (8.44%), indicating that targeted prevention and control measures should be improved and enhanced among the population that migrated to Shenzhen from other provinces of China (excepting Hubei Province). For instance, the real-time polymerase chain reaction would be conducted to detect SARS-CoV-2 for individuals from other cities of China to identify them in the early stage. The ceased local outbreak of COVID-19 in Shenzhen indicated that local municipal government implemented intensive prevention and control measures across the community (Zhou et al. 2020). The measures involved multisectoral coordination to control the epidemic, proactive close contacts and sub-close contacts tracing and testing, timely and standardized isolation and treatment, strict and standardized control of nosocomial infection, strict and effective community management, and timely information dissemination to contain the epidemic and reassure the citizens. In addition, symptom monitoring and contact tracking record of web-app approach supplemented the current management strategies to cease COVID-19 prevalence (Yap and Xie 2020); contact tracing (especially based on digital technology) can suppress the spread of COVID-19 if a high enough proportion of the population uses the app and that it can still reduce the number of infections if uptake is moderate (Zou et al. 2020). Moreover, it is suggested that similar prevention and control strategies and measures can be adopted in countries and regions that are ready to deal with the pandemic.
In the first stage of COVID-19 prevalence in Shenzhen (from January 19 to February 12, 2020; Appendix Table A2), 391 SARS-CoV-2 cases were found, and another study inferred that infected and uninfected close contacts mainly contributed to the COVID-19 pandemic (Bi et al. 2020); this is because many cases (local patients and imported cases from other province of China) emerged in this stage, the epidemic peak of the COVID-19 has arrived, the strategies and measures to eliminate COVID-19 are mainly aimed at cases and their close contacts (Bi et al. 2020), it may stop the epidemic of COVID-19 as soon as possible; in addition, asymptomatic infection has not been cognized in this stage, and individuals from other countries cannot enter China (including Shenzhen) in this stage. In the second stage of COVID-19 prevalence in Shenzhen (from February 13 to April 30, 2020; Appendix Table A2), China (including Shenzhen) has successfully controlled the local prevalence of the COVID-19 epidemic and has since focused on preventing and control of imported cases (Ren et al. 2021). Beginning April 1, 2020, individuals who enter China through the sea, land, and air from the countries and regions where COVID-19 is prevalent have been mandatorily tested for SARS-CoV-2 infection at border checkpoints and 14 days of medical observation at isolation hotel. In addition, the asymptomatic infection was found in China for the first time, and the proportion of asymptomatic infection is very high and rising among all SARS-COV-2 positive international travelers, which may indicate the increase of asymptomatic infection in the world. Hence, imported cases and asymptomatic infection are keys to spread the COVID-19. Finally, targeted prevention and control measures should be continuously changed according to the COVID-19 epidemic characteristics in the different periods.
The asymptomatic infections are difficult to be identified, and the individuals lack awareness of protection as they do not know about their infection (Bai et al. 2020); hence, their close contacts might result in the same or higher actual infectivity than confirmed cases. In the current study, the proportion of asymptomatic infection increased continuously over a period; it might be because of the continuous improvement in the detection capability and testing intensity.
The development of safe, effective, affordable, and deployable vaccine against COVID-19 remains paramount in addressing the pandemic crisis (Zhu et al. 2020b). However, presently, the global pandemic of COVID-19 does not have a defined duration, and there is always a risk of imported sources of infection. China will always face the risk of imported cases as long as the pandemic is not under effective control. In addition, as insidious sources of transmission, asymptomatic infections may be a major risk in the future development of COVID-19. Thus, normalized prevention and control measures are required for the low risk areas. Professional institutions are required to perform effective disease surveillance and build a sensitive, efficient, long-lasting, and well-run monitoring system that will identify the epidemic at the early stage. Moreover, timely and scientific emergency disposal measures and continued publicity and education would be conducted for the prevention and control of COVID-19. These measures include maintaining social distancing and wearing masks in crowded places to avoid the second outbreak of COVID-19.
Limitations
This study has several shortcomings that need to be addressed. It was a cross-sectional study, and hence, a causal conclusion could not be obtained. At the same time, the number of COVID-19 patients imported from abroad and with asymptomatic infection was not large; the results may be unstable and not reliable. Therefore, a large-sample study should be conducted in the future, and the asymptomatic COVID-19 infection merits additional investigation.
Conclusions
The finding of this study showed that asymptomatic infected individuals accounted for a high proportion among individuals imported from abroad, indicating that improved detection capability to identify the asymptomatic infection is critical for the controlled outbreak and prevalence of COVID-19. Furthermore, the control strategies at airports, seaports, and land ports should be adjusted constantly according to the new change in COVID-19 development in other countries. This approach is critical in identifying the infection source in a timely manner and ensures that imported infected individuals do not cause local outbreaks and epidemics.
Ethics Statement
The study was approved by the ethical review committee of the Chinese Clinical Trial Registry (SZCDCERC2020004A). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. All subjects signed informed consent form for the publication of their clinical details.
Footnotes
Acknowledgments
The acknowledgment is forwarded for the study participants for their valuable information and data collectors and supervisors for their commitment.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This study was supported by the Key Scientific and Technological Project of Shenzhen Science and Technology Innovation Committee (JSGG20200207161926465, KCXFZ202002011006190); the 13th Five-Year National Science and Technology Major Project for Infectious Diseases (no. 2017ZX10305501-002); the Open Project of Key Laboratory of Parasite and Vector Biology, China Ministry of Health (WSBKFKT-201804); the China Postdoctoral Science Foundation (no. 2020T130022ZX); the Shenzhen San-Ming Project for Prevention and Research on Vector-borne Diseases (no. SZSM201611064); the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2020-PT330-006); the Shenzhen Key Medical Discipline Construction Fund (SZXK064); the Program for the Shanghai Natural Science Foundation of China (no. 18ZR1443500); the Open project of Key Laboratory of Tropical Disease Control (Sun Yat-sen University), Ministry of Education (no. 2019kfkt02); the Key Laboratory of Echinococcosis Prevention and Control (no. 2020WZK2002). Thesis public-funded institutes have no role in the design of the study, collection, analysis, and interpretation of the data, and in writing the article.
Supplementary Material
Supplementary Appendix 2
Appendix
Appendix Table A4. Imported Countries of Confirmed Cases and Asymptomatic Infected Persons in Shenzhen, China
| Countries | Total (n = 53), n (%) | Confirmed case (n = 39), n (%) | Asymptomatic infection (n = 14), n (%) |
|---|---|---|---|
| The United Kingdom | 18 (33.96) | 14 (35.90) | 4 (28.57) |
| The United States | 13 (24.53) | 9 (23.08) | 4 (28.57) |
| France | 8 (15.09) | 4 (10.26) | 4 (28.57) |
| Philippine Islands | 4 (7.55) | 3 (7.69) | 1 (7.14) |
| Spain | 2 (3.77) | 2 (5.13) | 0 (0.00) |
| Brazil | 2 (3.77) | 2 (5.13) | 0 (0.00) |
| Switzerland | 2 (3.77) | 1 (2.56) | 1 (7.14) |
| Russia | 1 (1.89) | 1 (2.56) | 0 (0.00) |
| Netherlands | 1 (1.89) | 1 (2.56) | 0 (0.00) |
| Thailand | 1 (1.89) | 1 (2.56) | 0 (0.00) |
| Cambodia | 1 (1.89) | 1 (2.56) | 0 (0.00) |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.