
Abstract
Cutaneous leishmaniasis (CL) is highly prevalent in rural and sylvatic regions of Latin America, with an estimated 55,000 annual cases. Diagnosis in resource-limited areas still relies on microscopy of dermal scrapings, while more sensitive methods like PCR are not attainable due to costs and lack of adequate health infrastructure. Isothermal amplification of Leishmania DNA can be performed without sophisticated equipment and training and may become a point of care (POC) test for health care centers with scarce resources. We evaluated the efficacy of recombinase-polymerase-amplification (RPA-LF) to diagnose CL in 226 patients attending a clinic in Puerto Maldonado within the Peruvian Amazon basin. Conventional PCR targeting kinetoplast DNA (kDNA-PCR) was used as the gold standard. Eight of 226 patients were considered true negatives (microscopy, kDNA-PCR, and RPA-LF negative), while RPA-LF resulted positive in 186 of 204 kDNA-PCR positive patients, yielding 91.2% (confidence interval [CI] = 86.5–94.4%) sensitivity and 93% (CI 88.6–95.8%) positive predictive value. There were 14% (32/226) discrepant samples alternating positive and negative results in similar proportions between both tests. Quantitative PCR used to resolve the discrepancies suggested that they occurred in samples with scarce parasite numbers as determined by high cycle threshold (Ct) values (≥32; cutoff 35.5). Microscopy had the lowest sensitivity of all methods (45.4%). Nested real-time PCR performed in 71 samples determined that Leishmania (Viannia) braziliensis was highly prevalent (69/71), and Leishmania (Viannia) lainsoni was present in only two isolates. Results indicated that RPA-LF has POC potential for CL endemic areas, yet further simplification and optimization coupled with field validation will be necessary to confirm its broad applicability.
Introduction
Cutaneous leishmaniasis (CL), a neglected tropical disease targeted by the WHO Tropical Diseases Research program, has a devastating global impact, affecting people in 92 endemic countries (Alvar et al. 2012). In the American continent the annual incidence was estimated to be between 187,000 and 300,000 cases (Alvar et al. 2012). It is caused by the protozoan Leishmania and transmitted by the bite of infected sand flies. CL causes a spectrum of diseases that include single or multiple ulcerated, nodular or papular lesions, as well as destructive nasal and oropharyngeal lesions of mucosal tissues (Burza et al. 2018).
Peru has the third highest number of CL cases in the Americas (6396 in 2017 and 5764 in 2018) (CDC-Peru 2019), after Brazil and Colombia. Seventeen of the 24 regions of Peru are endemic for CL, but most cases occur in the regions east of the Andes Mountains. The most common causative species are Leishmania from the Viannia subgenus, primarily Leishmania (Viannia) braziliensis and Leishmania (Viannia) peruviana (Odiwuor et al. 2012). Occasionally, other species within the Leishmania (Viannia) subgenus such as Leishmania guyanensis, Leishmania Shawi, and Leishmania lainsoni are isolated from cutaneous lesions of Peruvian patients (Lucas et al. 1998, Foulet et al. 2007, Llanos-Cuentas et al. 2008, Kato et al. 2010, Cordova et al. 2011). Like most countries of Latin America where CL is endemic, highly sensitive and accurate diagnostic tests are restricted to centralized laboratories, while microscopy of stained lesion scrapings is the only available test in primary health care centers in endemic regions (Boggild et al. 2010, de Vries et al. 2015).
One of the goals of leishmaniasis control programs is to improve patient management by increasing the capacity of health centers in rural areas to efficiently diagnose CL. The possibility of diagnosing and initiating CL treatment the same day would increase patient compliance leading to better therapeutic outcomes and reduced costs (Bern et al. 2008).
Outside Leishmania endemic areas, PCR-based amplification of DNA isolated from lesion material in reference centers is the most widely used method to diagnose CL, although no standardized protocol has been established (Galluzzi et al. 2018, Moreira et al. 2018). Isothermal amplification of Leishmania DNA, which can be performed without sophisticated equipment and training, is an attractive alternative for implementation in resource-limited health care centers (Saldarriaga et al. 2016, Castellanos-Gonzalez et al. 2018). Our previous work using various species of the Leishmania (Viannia) subgenus determined that recombinase-polymerase-amplification coupled with lateral flow reading (RPA-LF) had an analytical sensitivity equivalent to 0.1 parasites per reaction and no cross reactivity with Leishmania species outside of the Viannia subgenus (Saldarriaga et al. 2016). We demonstrated that among the isothermal amplification methods, RPA-LF has potential applicability in primary health care institutions (Saldarriaga et al. 2016).
This study evaluated the efficacy of RPA-LF to diagnose CL in patients who attended a leishmaniasis clinic in Puerto Maldonado (Madre de Dios Region), an endemic region in the Peruvian Amazon basin (Kato et al. 2010, Bol-Epidemiol-Peru 2012, Valdivia et al. 2012). We found that RPA-LF has sufficient diagnostic efficacy for use in primary health care institutions where microscopy is the only method to diagnose CL.
Materials and Methods
Ethical statement
This study was approved by Naval Medical Research Unit 6 (NAMRU-6) Scientific Review Board and Institutional Review Board (el IRB reference number NMRCD 2007.0018) in compliance with all applicable federal regulations governing the protection of human subjects.
Patients and study site
The NAMRU-6 study site in Puerto Maldonado (Madre de Dios) in the Peruvian Amazon region was the site of this study. Patients of both sexes (n = 226), who were 6–85 years of age and suspected of having active CL, were enrolled after providing informed consent. Study personnel collected demographic and epidemiological data from each patient and possible factors favoring infection and disease development.
Clinical samples
Following the standard of care, samples for diagnosis and identification of Leishmania species were obtained by scraping the internal border of ulcerated skin lesions with a lancet to prepare tissue smears for microscopy. Subsequently, six 3 mm diameter filter papers cut from Whatman FTA® cards were placed in direct contact with the ulcer using clean disposable forceps. The filter papers remained <1 min on the ulcer until they absorbed interstitial fluid, loose cells, and cellular debris. The filter papers were picked up with the forceps and let to dry inside an open plastic bag that was then sealed with desiccant for transport. Samples were coded for deidentification and transported at room temperature to the reference laboratories in NAMRU-6, Lima, and the University of Texas Medical Branch (UTMB).
DNA extraction
DNeasy Blood & Tissue Kit (QIAGEN) was used for extracting DNA from lancets and filter papers following manufacturer's instructions. For Whatman FTA discs, we followed the steps previously described (Saldarriaga et al. 2016). Briefly, two 3 mm filter papers were transferred to 1.8 mL microcentrifuge tube using disposable sterile plastic forceps. The filter papers were then washed thrice for 5 min each with 200 μL of FTA Purification reagent (GE Healthcare Life Sciences) followed by two additional washes with 200 μL of TE buffer pH 8 (Sigma-Aldrich) for 5 min at room temperature. Finally, the filter papers were suspended in 50 μL of TE buffer (AE buffer; Qiagen) and heated at 95°C for 30 min. Filter disks were discarded, and the DNA in solution was stored at −20°C until used.
Conventional PCR
This test (kinetoplast DNA [kDNA]-PCR) was run to identify Leishmania (Viannia) subgenus using MP1L and MP3H primers as previously described (Lopez et al. 1993). The kDNA-PCR mixture contained 1 × PCR buffer (Invitrogen, Carlsbad, CA), 1.5 mM MgCl2, 125 μM dNTPs, 0.5 μM of each primer, 0.05U/μL Platinum Taq DNA Polymerase (Invitrogen), and 4 μL of DNA sample. The thermal cycling conditions were: initial denaturation step at 94°C for 5 min followed by 35 cycles of denaturation at 94°C for 45 s, annealing at 58°C for 45 s, extension at 72°C for 1 min, and a final extension step at 72°C for 5 min. This kDNA-PCR generated an electrophoretic band of 70 bp specific for Leishmania (Viannia) subgenus.
Nested real-time PCR
For Leishmania species identification we used a nested real-time PCR based on Mannose Phosphate Isomerase (mpi) and 6-Phosphogluconate Dehydrogenase (6pgd) genes as previously described (Tsukayama et al. 2013). The first amplification round contained 1 × PCR buffer (Invitrogen), 1.5 mM MgCl2, 200 μM dNTPs (Invitrogen), 0.25 or 0.8 μM of each primer (MPI and 6PGD, respectively), and 0.03U/μL of Platinum Taq DNA Polymerase (Invitrogen). The thermal conditions were as follows: initial denaturation at 94°C for 5 min, followed by 40 cycles (MPI) or 35 cycles (6PGD) of denaturation at 94°C for 45 s; then, an annealing at 55°C (for MPI) or 62°C (for 6PGD) for 45 s and extension at 72°C for 90 s (for MPI) or 1 min (for 6PGD). The final extension was at 72°C for 5 min. The second amplification round contained 1 × LightCycler 480 Genotyping Master (Roche Diagnostic GmbH), 1.25 μM of forward primer, 0.25 μM of reverse primer, 0.18 μM of anchor and sensor probes, and 5 μL of PCR product from the first reaction. This amplification was carried out in a LightCycler 480 real-time PCR System (Roche Instrument Center) and consisted of an initial denaturation at 95°C for 5 min followed by 45 cycles of denaturation at 95°C for 10 s, annealing at 60°C for 20 s under a single acquisition step, and extension at 72°C for 20 s. A melting curve analysis was performed at the end of the amplification cycles by heating the amplicons at 95°C for 10 s, cooling at 45°C for 59 s, and then gradually increasing the temperature to 80°C with continuous acquisition steps at each Celsius degree.
Quantitative PCR
Quantitative PCR (qPCR) was used as a resolver test to determine the positivity or negativity of RPA-LF and kDNA-PCR discrepant results. DNA quantification using spectrophotometric reading (Nanodrop) from FTA-preserved samples usually yield unreliable data. Therefore, we suspended each sample in the same volume of TE buffer and used identical aliquots (2 μL) to run the test.
We used iTaq Universal SYBR Green (Bio-Rad) real-time PCR using the primers described by Pita-Pereira et al. (2012). The reaction mixture contained 2 × iTaq Universal SYBR Green Master Mix (Bio-Rad), 0.25 μmol of each primer, 2 μL of template DNA, and distilled ultrapure water for a final reaction volume of 10 μL. The reactions were set up, in triplicate, in a 384-well optical reaction plate in an ABI ViiA 7 Real-Time System (Applied Biosystems, Foster City, CA). The PCR conditions were as follows: an initial 2.5 min incubation step at 94°C, followed by 40 cycles of 30 s at 94°C, 30 s at 60°C. The generation of amplification plots and analyses was detected at the end of each cycle. After amplification, the melting curve was performed per standard operating procedures to allow for confirmation of amplicon identity. Stringent measures to control sample contamination included 6 nontemplate negative controls (NTC, reaction mix without DNA and distilled water alone), six nontemplate buffer (TE) negative controls, and three nonrelevant DNA controls, in each reaction plate. Positive controls (100 and 10,000 Leishmania sp.) were also included.
RPA reaction and lateral flow reading
The primers and probes for detection of Leishmania spp. DNA have been described by Saldarriaga et al. (2016). Briefly, the primers and probe (Fw-GATGAAAATGTACTCCCC GACA TGCCTCTG; Rev-bio-CTAATTGTGCACGGGGAGGCCAAAAATAGCGA; Probe-FAM-GTAGGGGNGTTCTGCGAAAACCGAAAAATG[THF]CATACAGAAA CCCCG[C3-spacer]) were added with magnesium acetate to the rehydrated cocktail containing recombinase polymerase (TwistAmp nfo RPA Kit; TwistDx). The amplification was carried out at 42°C for 30 min using a dry bath. The RPA product was then diluted 1:25 in the dipstick dilution buffer, and 70–100 μL were transferred to a 1.8 mL microcentrifuge tube. The lateral flow strip (UStar) was held vertically, and only the bottom tip of the lateral flow strip was immersed in this solution to enable the diluted amplification product to run upwards by capillarity. The results were read with the naked eye after 5 min. The appearance of a test band in the lower part of the strip (in addition of the upper control band) indicated a positive reaction.
Analysis of data
We aimed to enroll 184 Leishmania positive cases confirmed by the gold standard test (kDNA-PCR), as well as 42 patients with cutaneous lesions due to other causes (e.g., basal cell or squamous cell carcinoma, sporotrichosis, cutaneous anthrax, actinomycosis). The total number of gold-standard positive samples needed was estimated based on an expected sensitivity of 95% or higher, to be able to demonstrate that the sensitivity of the RPA-LF test is 90% or better with 95% confidence and 80% power. This sample size allows estimating the sensitivity very precisely with a narrow confidence interval (CI), approximately 90–98% if the expected 95% sensitivity is observed. The total number of gold-standard negative samples needed per site (n = 42), on the other hand, was estimated based on an expected specificity of 99% or higher, to be able to demonstrate that the specificity of the RPA-LF test is 90% or better with 95% confidence and 80% power. This sample size allows estimating the sensitivity very precisely with a narrow CI, approximately 92–100% if the expected 99% sensitivity is observed.
Statistical analyses were performed using GraphPad Prism version 8.3. The comparison of sensitivity and specificity of kDNA-PCR with RPA-LF used the McNemar chi-squared test because the pairs of tests were evaluated on specimens from the same patient. Each test performance was assessed by statistical indexes as follows: Sensitivity = [true positives/(true positives + false negatives)] × 100; specificity = [true negatives/(true negatives + false positives)] × 100. We used chi-squared test to compare proportion of patients with cutaneous lesions at different times of evolution and patients that were grouped according to activities commonly associated with risk of infection. Statistical significance was established at <0.05 using a 95% CI.
Results
A significantly larger number of patients came to the clinic with cutaneous lesions of <3 months of evolution (72.1%) compared to patients reporting lesions of ≥6 month's duration (12%) (χ2 p < 0.0001; 50.9–67.4%; Fig. 1). A single cutaneous lesion on limbs or face was the most frequent presentation (mode = 1; range 1–8). Demographic data collected from 172 patients showed that the median age was 28 years (range 6–82), and females represented 24% of the individuals enrolled. Reported occupations included farming, mining, or lumbering. Over 50% of patients reported occupations not known to pose increased risk of acquiring CL (Weigle et al. 1993, Loiseau et al. 2019). A large number of patients were students (31/172) in whom the risk of exposure was unknown. As expected, of those patients in which a specific occupation was obtained (n = 81), the highest proportion of infected individuals were farmers (37%). This group was significantly larger compared with miners (19.8%; χ2 p = 0.015; CI 3.3–30.3%) or homemakers (16.5%; χ2 p = 0.003; CI 6.9–33.2%). There were no significant differences in the proportion of farmers (37%) and patients dedicated to lumbering (27.2%). Women whose work was limited to the place of residence were also represented (16.5%), indicating that peri-domestic transmission likely was occurring (Fig. 1).

There was a significantly higher proportion of patients that came for consultation with lesions of short duration compared with patients with more chronic lesions (chi-squared test p < 0.0001, CI 34.1–52.9%). Grouping of patients by infection risk showed that farmers were significantly over-represented compared with miners (χ2 p < 0.01; CI 3.2–30.2%) or homemakers (χ2 p = 0.003; CI 6.9–33.2%). *p < 0.05; **p < 0.01. CI, confidence interval.
When we used kDNA-PCR as gold standard to evaluate the performance of RPA-LF, 8 of 226 persons were considered true negatives (microscopy, kDNA-PCR, and RPA-LF negative). Of the 226 subjects enrolled, RPA-LF resulted positive in 186 of 204 kDNA-PCR positive patients, yielding a 91.1% (CI = 86.5–94.4%) sensitivity and 93% (CI 88.6–95.8%) positive predictive value (Table 1).
Diagnostic Performance of Recombinase-Polymerase-Amplification Coupled with Lateral Flow Reading Having Kinetoplast DNA-PCR as Reference Test Determined in 226 Clinical Samples of Patients Attending the Clinic in Puerto Maldonado, Department of Madre de Dios, Peru
CI, confidence interval.
The diagnostic tests were discrepant in 14% of the samples (32/226) which affected RPA-LF specificity. Eighteen samples negative by RPA-LF were positive by kDNA-PCR, while 14 samples positive by RPA-LF were negative by kDNA-PCR (Fig. 2). Availability of 27 of the 32 discrepant samples allowed us to use qPCR as a resolver test. Seven samples (26%) were negative by qPCR, while the rest showed cycle threshold (Ct) values ≥32 (cutoff Ct 35.5) suggesting the presence of low parasite loads in patient samples, at or below the detection limit of RPA-LF or conventional kDNA-PCR.
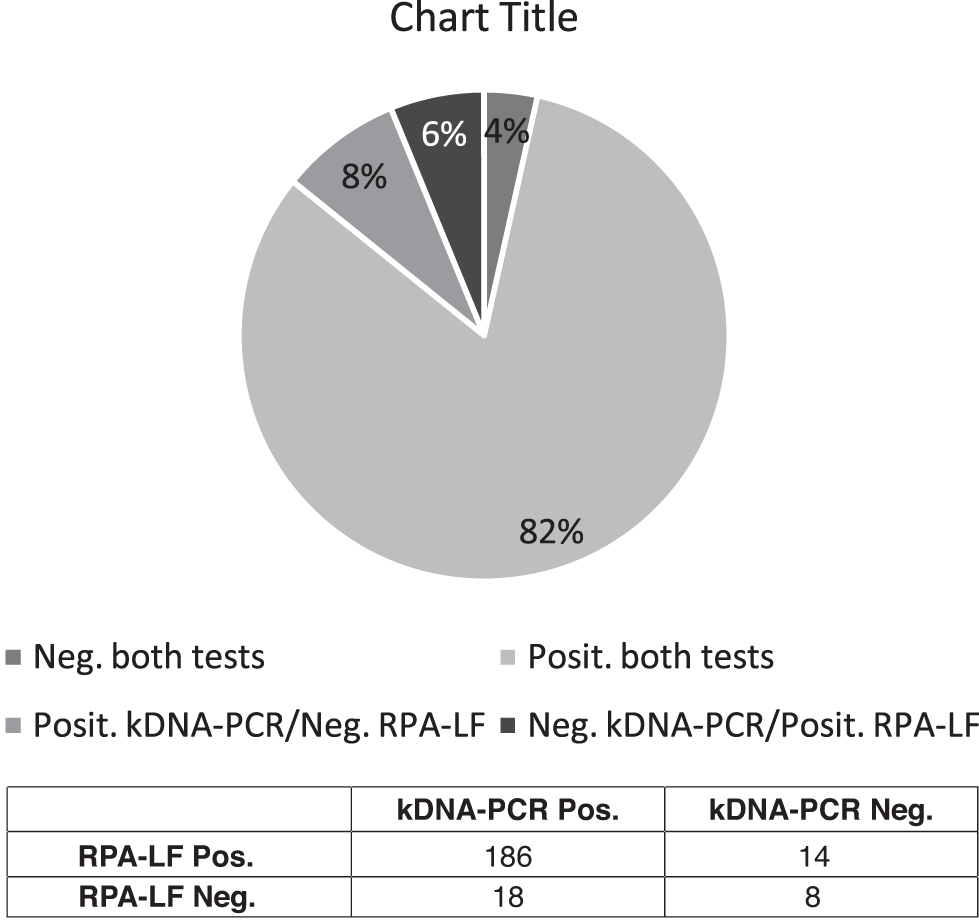
Number and proportion of patient samples (n = 226) that resulted positive by both diagnostic tests and discordant tests and negative by both tests.
We did not find a significant decrease of RPA-LF sensitivity when the test was applied to more chronic lesions, as described for standard parasitological methods (Luz et al. 2009, Satow et al. 2013). Twenty-nine of 32 patients (90.7%) with cutaneous lesions older than 4 months were positive by both molecular tests, while only 3 (9.3%) that showed weak bands in the kDNA-PCR gel were negative by RPA-LF. There was no correlation between the intensity of the test band in the lateral flow strips and the gel band of kDNA-PCR.
Only 45.4% (98/216) of patients were positive by microscopy yielding the lowest sensitivity of all the diagnostic tests. There was no association between the result of microscopy and the time of lesion evolution.
Species identification of Leishmania by Nested-RT-PCR was accomplished in only 71 subjects because of limited DNA availability. L. (V.) braziliensis was highly prevalent (69/71), while L. (V.) lainsoni was present in only two isolates (Veland et al. 2012, Suarez et al. 2015).
Discussion
In the current study, the evaluation of dermal samples from 226 patients who came for consultation with cutaneous ulcers indicated that RPA-LF had a diagnostic efficacy comparable to kDNA-PCR. However, there was significant discrepancy in the number of positive/negative patients between the two tests. As expected, the sensitive qPCR indicated that RPA-LF and kDNA-PCR could miss positive samples with very low numbers of parasites as indicated by Ct values close to the cutoff points (Ct 35–36). In these patients, CL could be confirmed by additional sampling aimed at extracting more DNA from the filter papers or delivering the samples to reference laboratories where qPCR is available.
Nested-RT-PCR showed that 97% of the isolates were L. brasiliensis, while <3% were L. lainsoni. A large proportion of RPA-LF positive isolates could be identified only at the genus level; therefore, we could not rule out that other species of the Viannia subgenus (e.g., L. shawi) were responsible for human infections in Madre de Dios (Kato et al. 2010).
A constraint of the study, common to most studies from endemic areas, is the lack of infection prevalence data from the study population in Madre de Dios, which prevented a more accurate estimate of the positive and negative predictive values of both tests (Vecchio 1966, Mischlinger and Schernhammer 2017). Human migration for economic reasons through the interoceanic highway in Madre de Dios adds complexity to the establishment of accurate CL prevalence (Guthmann et al. 1997, Jensen et al. 2018). For these calculations, we hypothesize that in the case of vector-borne diseases like leishmaniasis, it could be more relevant to use infection prevalence (e.g., leishmanin skin test) rather than disease prevalence since the risk of infection is independent of clinical manifestations (Rosales-Chilama et al. 2015).
Like previous studies from the Old and New World (Weigle et al. 1987, 2002, Andresen et al. 1996, Rodrigues et al. 2002, Al-Jawabreh et al. 2006), we found that microscopy performed at the local clinic had low sensitivity (45.4%). There was no significant difference in the diagnostic efficacy of RPA-LF or kDNA-PCR between patients presenting recent or chronic lesions (>3 months evolution), a potential problem affecting standard microscopy (Weigle et al. 2002). We had no information on the number of patients with previous history of CL, but we hypothesized that some of the samples that were negative by RPA-LF or kDNA-PCR (but positive by qPCR) were from individuals with recurrent lesions that may have harbored markedly low parasite densities as described by Pereira et al. (2017).
The utilization of Whatman FTA filter paper specially designed to preserve DNA has been used previously on lesions of patients to determine the ecological distribution of Leishmania species in Peru (Kato et al. 2010). Sample collection using filter paper allowed us in obtaining reproducible results after transporting the deidentified clinical samples at room temperature from the clinic in Puerto Maldonado to the laboratory in Galveston, Texas (UTMB). We believe that there are still possibilities of further refining RPA-LF for improved sensitivity and applicability in austere field environments. DNA extraction could be simplified to shorten the purification step with the goal of reducing the time with which results are delivered to patients. A short turnaround time is needed because individuals living in distant townships may not return a second time to obtain the result and initiate therapy due to transportation hurdles (distance, costs) and loss of labor days. Initiation of treatment immediately after receiving the result could improve compliance and reduce morbidity, as well as decrease the possibility of transmission to others (Vergel et al. 2006).
Variations of band intensity in the lateral flow strip were not consistently associated with high or low parasite burdens as suggested by the corresponding strength of kDNA-PCR bands in the gels or Ct values of qPCR. This lack of correlation could have been due, in part, to varied DNA input upon extraction from different filter papers from the same patient to perform kDNA-PCR or RPA-LF (or qPCR in a limited number of samples).
Therefore, as expected, visual reading of the lateral flow test strip is only qualitative and not a reliable estimate of pretreatment parasite loads in the lesions. Furthermore, it is unlikely that it can be used to monitor parasitological evolution during or after therapy even if the samples were obtained from the same cutaneous lesion. Visual detection of weak bands in lateral flow strips could be difficult to interpret. Consequently, inclusion of appropriate controls, principally the negative control showing no test band in the strip, is strongly recommended to validate the test result.
Another isothermal amplification test, loop-mediated amplification, has shown 80–100% sensitivity, yet complex primer design and variable reliability of methods used to read the qualitative results indicated that further optimization for field applicability is still required (Nzelu et al. 2019). Our evaluation of clinical samples indicated that RPA-LF fulfills many of the important features required for implementing a point of care (POC) diagnostic test for CL as defined by a recently published target product profile (TPP) (Cruz et al. 2019). In that work, the minimal and optimal TPP features of the diagnostic test were established by discussions and consensus with stakeholders and leishmaniasis experts from different organizations and CL endemic regions. We modified the table described by Cruz et al. (2019) to summarize specific RPA-LF characteristics that meet the optimal or minimal requirements of the POC test for CL. Within the optimal characteristics set forth in the table, RPA-LF fulfilled (1) the implementation in health care facilities with no infrastructure or mobile laboratory, (2) the noninvasive nature of sampling, and (3) the visual reading of results (Table 2).
Recombinase-Polymerase-Amplification Coupled with Lateral Flow Reading Features That Concur with Desirable Characteristics of the Point of Care Diagnostic Test for Cutaneous Leishmaniasis as Defined by Cruz et al.
POC, point of care.
Modified from Cruz et al. (2019) original table.
Additional work should validate RPA-LF at field sites with different logistic and personnel capacity to demonstrate broad applicability. Negative samples using this test should be sent to a reference laboratory for further diagnosis of CL or other dermal pathologies. Nevertheless, this work indicates that RPA-LF could be implemented in laboratories with minimal health infrastructure as either the only diagnostic test or following negative microscopy of suspected cases. Both strategies would facilitate improved diagnosis of CL in remote endemic areas. Future test optimization by reducing processing time (<30 min) and steps for DNA purification are achievable goals that will significantly enhance its applicability at community level by health care workers.
Footnotes
Acknowledgments
The authors are grateful to the patients participating in the study and the technical and logistic support of Centro de Salud Jorge Chavez, Centro de Salud Nuevo Milenio, and Laboratorio de Referencia Regional de Madre de Dios.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This study was partially funded by the US DoD Armed Forces Health Surveillance Division and its Global Emerging Infections Surveillance branch (AFHSD/GEIS) under PROMIS ID 17_N6_1.2.3, 2016–2017 and by a Congressionally Directed Medical Research Programs (CDMRP) award W81XWH-14-2-0196 and W81XWH-14-2-0195.