
Abstract
Background:
Pseudorabies virus (PRV) is a common pathogen found in pigs. The pathogenicity of PRV in humans is under researched and there are few confirmed cases of PRV infections in humans, which has led to a lack of clinical consensus.
Methods:
We presented a case of viral encephalitis caused by PRV in China. We performed a systematic review of the literature to investigate the clinical features and prognosis of PRV encephalitis and included 12 patients with PRV encephalitis.
Results:
All the patients had a history of direct or indirect contact with living pigs or pork before the onset of the disease, accompanied by prodromal symptoms, such as fever and headache. They presented with a series of lesions involving the central nervous system (CNS) and respiratory system, such as acute encephalitis syndrome, respiratory failure, retinitis, or endophthalmitis.
Conclusions:
The differential diagnosis of an acute attack of CNS infection should include PRV encephalitis, which should be diagnosed by a head magnetic resonance imaging (MRI), fundus examination, and cerebrospinal fluid next-generation sequencing. Intravenous immunoglobulin, glucocorticoid, antiviral, and symptomatic support treatment should be administered as early as possible to improve the prognosis.
Case Study
Introduction
The pseudorabies virus (PRV), also known as suid herpesvirus type 1, is a double-stranded DNA virus with an icosahedral symmetry and it belongs to the α-herpesvirus subfamily and varicella virus genus. PRVs have a wide range of hosts, including pigs, as natural and reservoir hosts (Pomeranz et al. 2005). Like other herpesviruses, the PRV is highly neurotropic and can infect the nervous system of host animals through transsynaptic passage and retrograde axonal transportation. There have been controversial cases of PRV infections in humans based on clinical symptoms, animal contact history, or antibody detection since 1914 (Anusz et al. 1992, Avak et al. 1987, Skinner et al. 2001).
After demonstrating the role of next-generation sequencing (NGS) in identifying unknown central nervous system (CNS) infection pathogens (Brown et al. 2018), both Ai et al. (2018) and Zhao et al. (2018) reported successive cases of human PRV infections that were confirmed at the genetic level. However, while the pathogenicity of PRV infections in humans is being researched and understood, confirmed cases of PRV infections in humans have been reported poorly, leading to a lack of clinical consensus. Herein, we described a case of a patient with viral encephalitis.
Case presentation
A 43-year-old man was admitted to our hospital on May 14, 2019, with fever and loss of consciousness and limb convulsions for 36 days, followed by fever and mood abnormalities for 3 days after improvement. The patient had a fever (highest temperature 39.5°C) with limb tremors that started 36 days before admission. In the early hours of the following day (35 days ago), he became unconscious with the thrashing of the limbs, eye deviation, loss of consciousness, and urinary incontinence. He had several seizures that lasted for 3 min. Pathogen detection using NGS at a local hospital showed a “suid herpesvirus type 1” infection in the cerebrospinal fluid (CSF) (Fig. 1). He was diagnosed with viral encephalitis with status epilepticus and was treated with antiviral agents, anti-infection agents, corticosteroids, and intravenous immunoglobulin (IVIG), to lower the intracranial pressure. He required endotracheal intubation and was treated in the intensive care unit.

Next-generation sequencing of the cerebrospinal fluid detected PRV with one unique sequence read and 0.03% coverage. PRV, pseudorabies virus.
The patient's consciousness was restored gradually, and there was a steady alleviation of the symptoms; however, there were still limb tremors. Thirteen days prior, the patient had recurrent fever, displayed mental disorders, emotional abnormalities, groping, and hallucinations (Fig. 2). A large number of pigs raised by the patients died 30 days before the onset of the disease, and spontaneous death was within ∼1–2 days. Before and after the onset of the disease in the pigs, a large number of ducks died of “big tongue disease.”
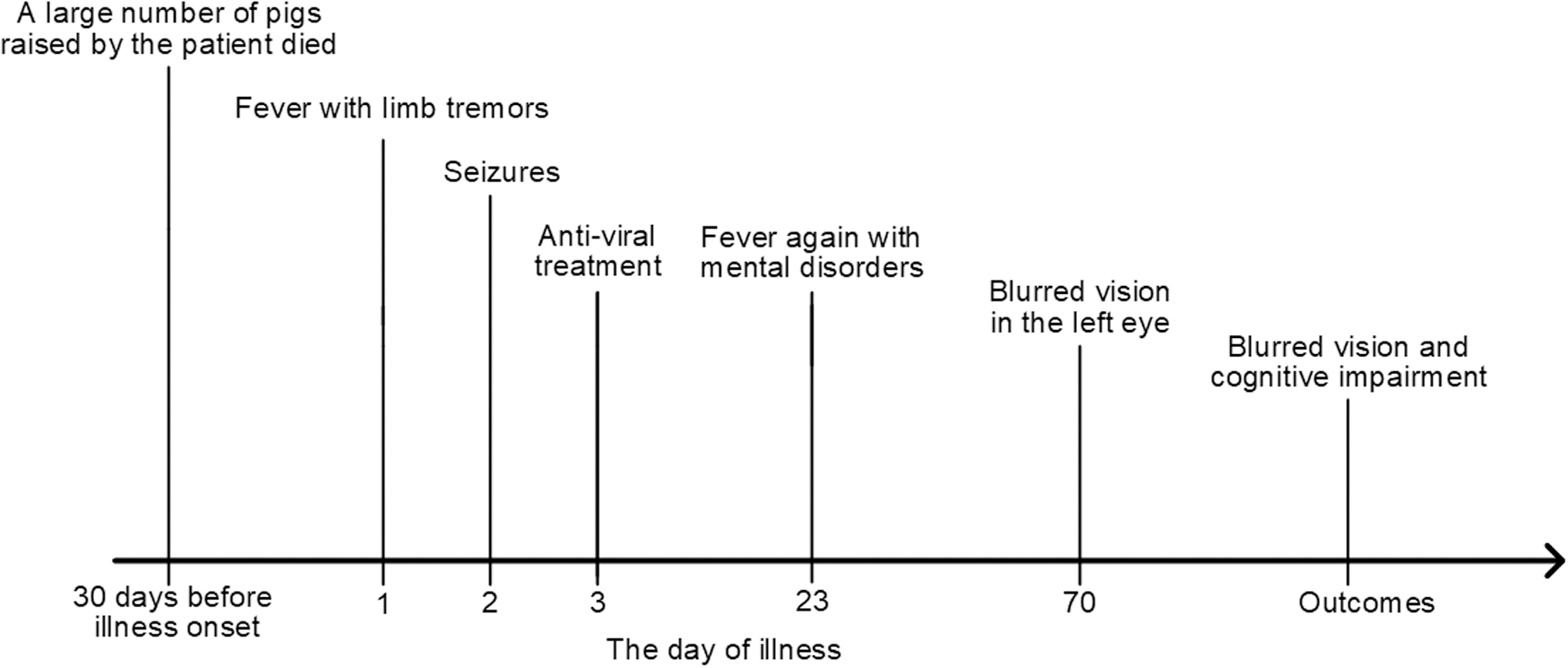
The brief of this patient's illness process (the fever onset day was considered the first day of illness).
The patient had a previous history of ankylosing spondylitis for 10 years. Physical examination upon admission: Physical analysis of the patient showed cognitive impairment and mild slurring in speech, limb tremor, and quadriparesis. The Kernig test results were positive. The brain magnetic resonance imaging (MRI) showed negative results on the 1st day (on the 10th day there were intense diffusion-weighted imaging signal changes in the bilateral temporal lobe and hippocampus, on the 34th day, there were neuroimaging T2 hyperintensities in the left basal ganglia, bilateral hippocampus, bilateral insula, and bilateral frontal lobe) (Fig. 3). Pulmonary computerized tomography (CT) showed extensive and diffuse opacities in the bilateral lungs on the 20th day. On the 28th day, the CSF analysis showed a white blood cell (WBC) count of 20 × 106/L, glucose of 3.15 mmol/L, and protein level of 1.06 g/L. Funduscopic examination indicates the papilledema. The tryptophan test, India ink staining, and bacterial smears were all negative.

Brain MRI of patients with PRV encephalitis.
The patient was discharged after 5 weeks of treatment with the antivirals, acyclovir and foscarnet, with olanzapine combined with lorazepam and valproate to control the psychiatric symptoms, and intravenous human immunoglobulin and glucocorticoids to regulate the immunity. He was discharged with psychiatric disorders, intermittent blurred vision, and an impaired cognitive function. He was readmitted to the hospital on the 70th day when he presented with blurred vision in the left eye. Ophthalmologic consultation revealed a retinal artery occlusion in the left eye and nerve atrophy in both eyes.
Systematic Review
Background
At present, PRV infection is concentrated mainly in countries with dense pig herds, such as Asia, South America, and Europe. Although pseudorabies has been eliminated in domestic pigs in some developed countries (Müller et al. 2011), worldwide, infections often occur in wild animals, especially wild boars (Müller et al. 2011, Chiari et al. 2015, Pedersen et al. 2018). Its uncontrollability in wild animals indicated a great potential risk of PRV transmission. Human PRV infections reported in recent years often have a history of contact with pigs, indicating that pigs play a critical intermediate role in pathogen transmission. Whether humans are susceptible to PRV has been controversial for many years. Although contemporary in vitro experiments have demonstrated the possibility of PRV infections in humans, there are limited data on the transmission of PRV infections from animals to humans (Li et al. 2017).
Since Ai et al. (2018) reported a case of endophthalmitis caused by PRV in a swine farmer, several instances of human PRV infections have been reported. Liu et al. (2021) isolated a strain of PRV HSD-1/2019 from the CSF of a patient for the first time, which provided the first direct and robust evidence of cross-species transmission of PRV to the population (Liu et al. 2021). Therefore, we performed a systematic literature review of published cases to understand the clinical features and prognosis of reported PRV encephalitis.
Methods
PubMed, EMBASE, and the Cochrane Library were searched from inception to May 2021. Search terms were “Pseudorabies virus,” “Human,” and “Encephalitis” using PubMed, Google Scholar, and China National Knowledge Infrastructure (CNKI). All the patients who were suspected of having PRV encephalitis were evaluated for inclusion. The authors examined all the studies in the reference list in the included literature to find other qualified studies. The inclusion criteria for the cases were:(1) history of epidemiological exposure: history of direct or indirect contact with live pigs or pork-related items before the onset of disease; (2) clinical features consistent with viral encephalitis (Solomon et al. 2012): current or recent febrile illness with behavioral, cognitive, personality, or consciousness changes, or new seizures or new focal neurological signs. Exclusion criteria for the case were: PRV encephalitis with an unclear diagnosis or only nucleic acid or serologic testing and a lack of clinical features and treatment options. The study was performed in accordance with the principles of the Declaration of Helsinki. The medical procedures of this study were approved by the Local Ethics Committee of Affiliated Hospital of Hebei University of Engineering, Handan, China.
Results
A total of 21 potential PRV encephalitis patients (including our hospital cases) were obtained from this study through a preliminary data search. From these cases, 12 patients with PRV encephalitis who met the inclusion criteria were identified (Fig. 4). Table 1 summarizes the patient demographics, core symptoms, treatment options, and clinical outcomes of the diagnosed cases. A modified Rankin Scale (mRS) score was used as an indicator of the prognostic index. The average age of the 12 patients was 48 years (43–59), and 11/12 patients were male. All the patients were engaged in occupations that were related closely to pigs. In total, 7/12 of the patients who were injured at work were in close contact with pigs or with pork within 1 week before the onset of disease, and 2/12 pig farmers had many sick pigs die in a short period on the pig farm within 20–30 days before the onset of the disease. There were several commonalities in the clinical presentations of the 12 patients.

Flow diagram showing the selection of the cases included in analysis.
Clinical Features of the Patients with Pseudorabies Virus Encephalitis
AMB, abnormal mental behavior; CT, computerized tomography; HA, headache; MRI, magnetic resonance imaging; mRS, modified Rankin Scale; OI, ocular inflammation; RF, respiratory failure.
First, the 12 patients had different degrees of prodromal symptoms. A total of 7/12 patients displayed the more obvious prodromal symptoms of fever and headache, combined mainly with upper respiratory tract infections. The remaining 5/12 patients had a rapid onset and they experienced a combination of prodromal symptoms with neurological symptoms simultaneously. Second, they all showed severe CNS involvement with rapid progression, and all 12 patients developed severe clinical signs within 1–2 weeks after the onset, with an inferior prognosis. In total, 6/12 patients had symptoms of cognitive behavioral abnormalities that manifested mainly as inattention, unresponsiveness, and reduced verbal and emotional indifference, and all 12 patients presented with symptoms of tonic–clonic seizures. All 12 patients had varying degrees of consciousness, of which 10/12 were in a coma, 6/12 had a Glasgow Coma Scale (GCS) score of 3 (5 cases) and 4 (1 case), 1/12 experienced sopor, and 1/12 somnolence.
In terms of other neurological signs: 8/12 had nuchal rigidity; 3/12 had a positive Kernig's or Brudzinski's sign, and in 1/12, Babinski's sign was positive. Third, 12 patients presented with varying degrees of dyspnea, often with pneumonia, and 10/12 patients required tracheal intubation, tracheotomy-assisted ventilation, or even ventilator-assisted ventilation. Fourth, PRV can cause ocular infections. Five of the 12 patients in this study had varying degrees of optic nerve damage. The optic nerve involvement worsened gradually over the course of the disease, with optic nerve atrophy, retinal edema, or detachment occurring even after treatment improved the central nervous and respiratory systems.
For laboratory tests and imaging, the results of the CSF analysis in 12 patients were similar to those of other viral encephalitis; with a mild or moderate elevation of WBC count, lymphocytosis, or monocytosis; mildly elevated protein levels; and normal blood glucose levels. Most of the patients had an average WBC count within a week of symptom presentation. All 12 patients were diagnosed using NGS. In total, 5/12 patients received positive results for the serology testing and the PRV antibodies, and 1/12 of them were also positive for CSF antibodies; however, further studies and explorations are needed to determine how long it takes for patients to develop positive antibodies after infections. For imaging in patients with PRV encephalitis, cranial MRI was more sensitive than CT in 11/12 patients who underwent a cranial MRI. The main cumulative sites involved the limbic system (the island leaf, hippocampus, cingulate gyrus, and amygdala), frontal and temporal lobes, basal ganglia, and thalamus. In addition, two patients underwent CT.
The 1/12 CT showed no abnormalities, and 1/12 CT on day 8 after onset showed a low signal on the basal ganglia, occipital lobe, and limbic lobe. This may also explain the clinical signs of altered mental status and frequent seizures. All 12 patients were treated with antiviral and antiepileptic therapy, 11/12 with adjuvant glucocorticoids, and 10/12 with IVIG. Patients who survived treatment had severe neurological sequelae, with 11/12 patients having an mRS score ≥3 and there was one death.
Discussion
In this study, the 12 patients with PRV encephalitis were predominantly young and middle-aged males, who performed mainly manual work in close contact with pigs. More than half of the patients had a history of significant hand trauma before the onset of the clinical symptoms, which suggested that they may have contracted the virus through mucosal or blood contact with infected pigs or contaminated objects. This route of infection was also confirmed by Ai et al. (2018), who reported endophthalmitis caused by a PRV infection in a patient whose eyes were contaminated with sewage containing pig manure (Ai et al. 2018). PRV usually causes respiratory or CNS infections in mammals; however, the specific mechanism of human PRV infection remains to be clarified.
The clinical signs and severity of human viral infections matched those seen in other non-native hosts, such as the rhesus monkeys. They were susceptible to PRV infections through intracerebral inoculation, producing neurological symptoms similar to those reported in patients since 2017, including convulsions, tonic–clonic seizures, and pupillary light reflex retardation (Hurst 1936). In addition, previous animal and in vitro studies have shown that a PRV infection activates nonspecific signaling pathways that induce apoptosis, which may contribute to the rapid onset of respiratory failure in patients with PRV encephalitis.
MRI is more sensitive than CT for imaging the brains of patients with PRV encephalitis (Yuan et al. 2009), and CT is often negative within 1 week of onset. Brain lesions are diffuse, with major cumulative sites involving the limbic system (the island leaf, hippocampus, cingulate gyrus, amygdala), frontal and temporal lobes, basal ganglia, and thalamus, which explained the clinical signs of altered mental status and frequent seizures, consistent with the extent of lesion distribution after PRV infections in monkeys (Macacus rhesus) (Hurst 1936).
The early diagnosis and treatment are crucial for a reduction in mortality from this disease and treatment consists mainly of antiviral therapy, supplemented with immunotherapy and symptomatic supportive treatment. Most of the 12 patients were treated with IVIG, glucocorticoids, antiepileptic drugs, and antiviral treatment. Acyclovir antiviral therapy is recommended clinically for varicella-zoster virus (VZV) infection, which causes an acute retinal necrosis syndrome and encephalitis due to the close affinity of this virus (Weng and Zhang 2019). Therefore, the anti-PRV drug acyclovir is currently the first choice for empirical treatment; however, effective antiviral therapy remains to be determined. PRV encephalitis progresses rapidly and has a poor prognosis, and patients who survive treatment have severe neurological sequelae. Therefore, patients with acute episodes of CNS infection have clinical signs that progress rapidly.
Especially in patients with recent exposure to pigs, the differential diagnosis should include PRV encephalitis with a brain MRI and CSF NGS. Once a diagnosis is made, treatment should be started, including a fundus examination, IVIG, glucocorticoids, antiviral, and symptomatic support. In addition, clinicians should educate people in close contact with pigs to minimize viral infections.
China, as the largest producer and consumer of pork, the pig industry is being threatened gradually by PRV infections. After the first human PRV infection, confirmed at the genetic level, was reported by Ai et al. (2018) at the Huashan Hospital, Fudan University in 2018, consecutive cases have been reported. However, due to the small number of cases that have been clinically confirmed, representativity may have been poor, and the conclusion biased; therefore, further research is needed. As the detection methods and diagnostic criteria continue to improve, we will incorporate more information to support the analysis of the pathogenesis and treatment strategies of PRV encephalitis.
Ethics Statement
We received written informed consent from the patient's wife.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Footnotes
Acknowledgments
The authors thank the patient for cooperating with their investigation. They acknowledge the professionalism and compassion demonstrated by all the health care workers involved in his care.
Authors' Contributions
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
No funding was received for this article.