
Abstract
Spotted fever group Rickettsia species are intracellular bacteria transmitted by tick or mite vectors and that cause human diseases referred to as spotted fever group rickettsioses, or spotted fevers. In the United States, the most recognized and commonly reported spotted fevers are Rocky Mountain spotted fever (RMSF) (Rickettsia rickettsii), Rickettsia parkeri rickettsiosis, Pacific Coast tick fever (Rickettsia species 364D), and rickettsialpox (Rickettsia akari). In this study, we summarize and evaluate surveillance data on spotted fever cases reported to the Centers for Disease Control and Prevention (CDC) through the National Notifiable Diseases Surveillance System from 2010 to 2018. During this period, there were 36,632 reported cases of spotted fevers with 95.83% (N = 35,104) reported as meeting the case definition as probable and 4.17% (N = 1528) reported as meeting the case definition as confirmed. The average national incidence of total cases, both probable and confirmed, was 12.77 cases per million persons per year. The highest statewide incidence was in Arkansas, with 256.84 per million per year, whereas the lowest incidence occurred in California, with 0.32 per million per year (note that spotted fevers were not notifiable in Hawaii and Alaska). Cases of spotted fevers were reported more frequently among males by gender, White by race, and non-Hispanic by ethnicity. The incidence of spotted fevers increased significantly from 2010 to 2018, but it is uncertain how many of the reported cases were RMSF and how many developed from more moderate spotted fevers. Improvement of the ability to differentiate between spotted fever group Rickettsia species is needed.
Introduction
Classified by the Centers for Disease Control and Prevention (CDC) and Council of State and Territorial Epidemiologists (CSTE) as a nationally notifiable infectious disease, spotted fever group rickettsioses (spotted fevers) incidence has been monitored by the CDC since the 1920s. Spotted fevers are caused by a group of closely related intracellular bacteria from the genus Rickettsia (Biggs et al, 2016). Tick-borne spotted fever group Rickettsia species can be asymptomatic or cause a wide range of symptoms including headache, fever, and rash (CDC, 2020). Rocky Mountain spotted fever (RMSF) is the rickettsiosis in the United States that is associated with the highest rates of severe and fatal outcomes (Biggs et al, 2016).
Spotted fevers pose a significant clinical dilemma for physicians, progressing rapidly from a nonspecific febrile illness to organ failure and death in some untreated cases (Openshaw et al, 2010). Untreated case fatality rates for RMSF may be up to 20–25% (Childs and Paddock, 2002). Even though fatalities can be avoided with prompt treatment with a tetracycline antibiotic, treatment is most effective when started in the first 5 days of illness, and other broad-spectrum antibiotics are not effective (Zientek et al, 2014). Doxycycline is recommended by the American Academy of Pediatrics as the treatment of choice in patients of all ages (Chapman et al, 2006).
In this study, we summarize the passive surveillance data of human spotted fever cases reported to the CDC from 2010 to 2018. Our goal is to increase awareness of recent trends of spotted fevers and to analyze these patterns, following the methods used by Openshaw et al (2010) and Drexler et al (2016). We also characterize the epidemiology of reported cases, including demographic profiles, incidence, and the spatial–temporal patterns of infections.
Materials and Methods
National surveillance systems
The public health departments at state, territorial, and local levels can report RMSF cases through the parallel surveillance tools of the National Notifiable Diseases Surveillance System (NNDSS) or the CDC Tickborne Rickettsial Disease Case Report Form (
Tickborne Rickettsial Disease Case Report Form provides supplementary case data (including clinical course, risk factors for infection, travel history 2 weeks before onset of symptoms, whether or not a tick was found and removed from the patient's body, hospitalization status, laboratory results, and patient outcome) but is not publicly available. Not all NNDSS reports have a corresponding case report form. For this study, the data were accessed through publicly available Morbidity and Mortality Weekly Report (
Case definition and categorization
Beginning January 1, 2010, cases of RMSF were classified under a new encompassing category spotted fever group rickettsioses (spotted fevers) (Sun, 2018). We followed the case definition and categorization (CDC, 2010; Smithee et al, 2009) to summarize the data from 2010 to 2018. Spotted fever in the United States includes primarily cases of RMSF (R. rickettsii), Rickettsia parkeri rickettsiosis, Pacific Coast tick fever (Rickettsia species 364D), but also includes the mite-borne rickettsialpox (Rickettsia akari) (Drexler et al, 2016). Cases of spotted fevers can be categorized as confirmed, probable, and suspect based on a combination of both clinical and laboratory characteristics (CDC, 2010; Smithee et al, 2009).
A confirmed case is clinically compatible (meets clinical evidence criteria) that is laboratory confirmed, a probable case is a clinically compatible (meets clinical evidence criteria) that has supportive laboratory results, and a suspected case is with laboratory evidence of past or present infection but no clinical information available (e.g., a laboratory report) (CDC, 2010; Smithee et al, 2009). Specifically, clinical characteristics are characterized by acute onset of fever, and may be accompanied by headache, malaise, myalgia, nausea/vomiting, or neurological signs (CDC, 2010; Smithee et al, 2009). Laboratory evidence either provides confirmatory or supportive evidence.
Confirmatory evidence includes one or more of the following: (1) demonstration of a fourfold rise in immunoglobulin G (IgG)-specific antibodies reactive to R. rickettsii or other spotted fever group Rickettsia species by indirect immunofluorescence assay (IFA) between paired specimens (one taken in the first week of illness and the second taken 2–4 weeks later), (2) detection of R. rickettsii or other spotted fever group Rickettsia species in a clinical sample through PCR assay, (3) demonstration of spotted fever group antigen in biopsied specimens by immunohistochemistry, or (4) isolation of R. rickettsii or other spotted fever group Rickettsia species in a cell culture (CDC, 2010; Smithee et al, 2009).
Supportive laboratory evidence includes any serological evidence related to IgG or immunoglobulin M (IgM) antibodies reactive with R. rickettsii or other spotted fever group Rickettsia species by IFA, enzyme-linked immunosorbent assay (ELISA), dot-ELISA, or latex agglutination (CDC, 2010; Smithee et al, 2009).
Analysis
This study analyzed probable and confirmed human case data with an onset of illness between January 1, 2010, and December 31, 2018. National, state, and age-specific pieces of incidence were calculated using population data estimated from April 1 to July 1 of each year by the Population Estimates Program, United States Census Bureau (U.S. Census Bureau, 2020). The incidence was calculated as the number of infections per million persons per year (Openshaw et al, 2010). This study does not include confidence intervals or results from statistical hypothesis testing since reported cases cannot be generalized to unreported cases or to other reporting time periods (Heitman et al, 2016). No IRB approval was necessary since the source of the data is public and analysis of the data will not make the data individually identifiable.
Results and Discussion
From 2010 to 2018, 36,632 cases of spotted fevers were reported through NNDSS. There was a steady annual increase in cases from a low of 1985 in 2010 to a high of 6248 in 2017 (Fig. 1). The annual national incidence followed a similar trend as the annual reported cases, increasing from 6 in 2010 to ∼19 in 2017, with a mean of 12.77 for the 9-year period. Heitman et al (2019) also noticed this increase in spotted fever rickettsiosis from 2016 to 2017.
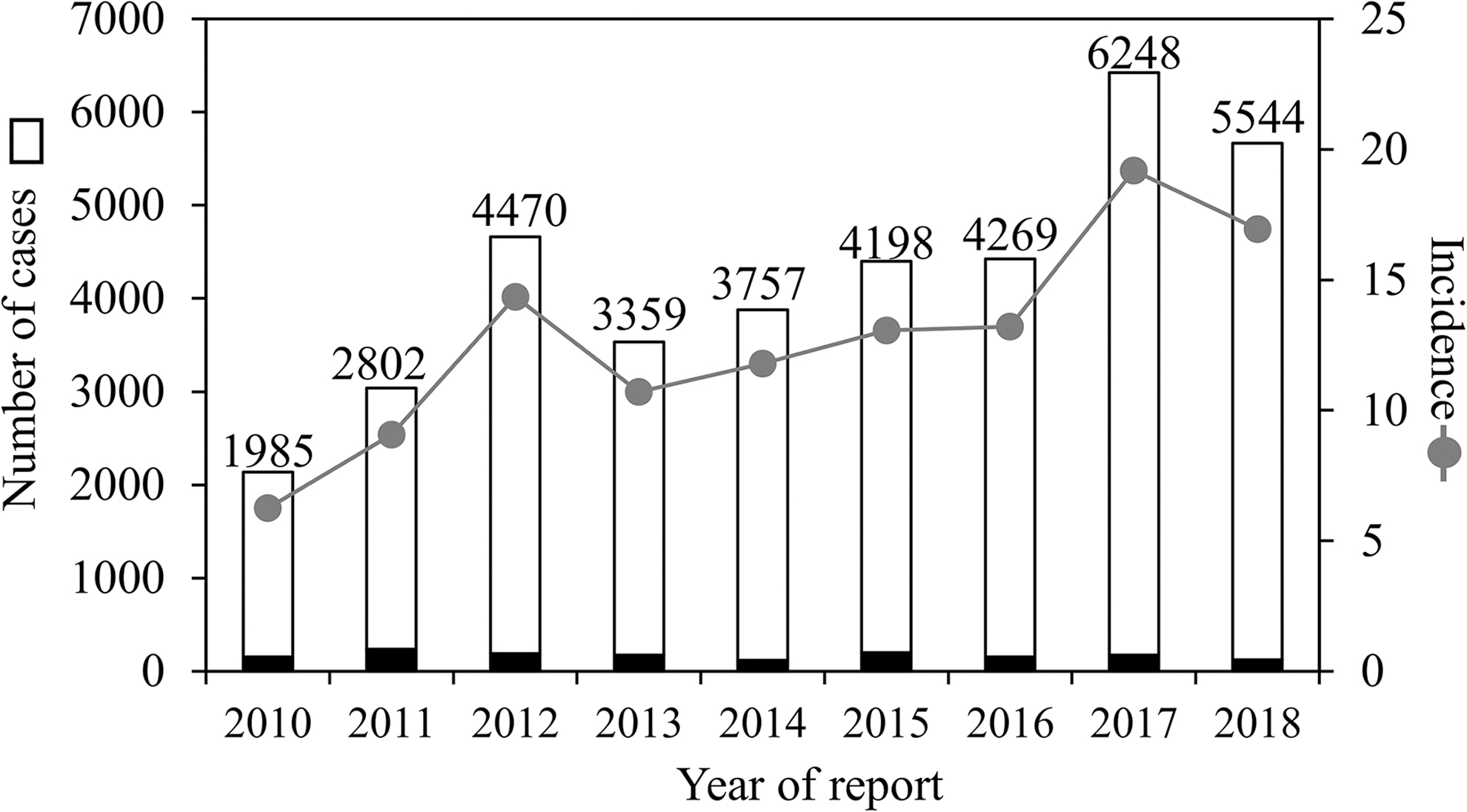
Number of reported cases and associated incidence of spotted fever group rickettsioses in the United States from 2010 through 2018. Bars represent confirmed cases (black portion) and probable cases (white portion). Gray dots represent incidence (No. of infections per million persons per year). Based on data from the Nationally Notifiable Diseases Surveillance System
Among the 2010–2018 reported cases, 95.83% (N = 35,104) and 4.17% (N = 1528) were classified as probable and confirmed, respectively, based on the spotted fever case definition. Cross-reactivity among members of the spotted fever group Rickettsia species and transitional group Rickettsia species (including R. akari and Rickettsia felis) limits the ability to draw antigen-specific conclusions and attribute to a specific rickettsial species (Drexler et al, 2016).
Demographic profiles of cases of spotted fevers indicated that males comprised 52.03% of the reported cases, females comprised 47.71%, and gender of the remaining 0.26% was unknown (Table 1). Regarding race, a majority of the reported cases were White (66.38%), followed by Black or African American (2.62%), American Indian or Alaska Native (2.23%), and Asian and Pacific Islander (0.48%), with 1.78% classified as “other” and the remaining 26.51% as “unspecified/unknown.” Non-Hispanic ethnicities comprised 66.61% of reported cases. More infections were reported in individuals 40–64 years of age (45.32%) and >65 years old (21.78%).
Demographic Profiles of Spotted Fever Group Rickettsiosis Cases in the United States Reported to the Centers for Disease Control and Prevention from 2010 to 2018
Incidence defined as the number of infections per million persons per year, based on cases reported to the Centers for Disease Control and Prevention and population data reported by the Population Estimates Program, United States Census Bureau.
The demographic profiles are generally consistent with those reported by Drexler et al (2016) based on CDC data for the 2008–2012 time period, although those authors indicated the highest incidence occurred in the 60–69-year age group. These profiles for spotted fevers also are similar to demographic profiles reported for other tick-borne diseases of humans including anaplasmosis, babesiosis, and ehrlichiosis (Baker et al, 2020; Bishop et al, 2021; Mogg et al, 2020). Such demographic patterns are potentially explained by behavioral and physiological differences among demographic groups (Kilpatrick and Randolph, 2012). These results may also reflect an inherent reporting bias due to the unequal access to health care among demographic groups (Jones et al, 2012).
Even though the reported cases were low for Native Americans (Table 1), Native Americans continue to be disproportionately impacted by spotted fevers considering their percentage of the United States population is <2% (Folkema et al, 2012; NCAI, 2020). Indeed, Adams et al (2017) also reported that the incidence of spotted fevers among American Indians or Alaska Natives was more than twice that of Whites, 9 times higher than of Blacks or African Americans, and 25 times higher than of Asians and Pacific Islanders in 2015.
Epidemics of RMSF have been ongoing since 2003 on tribal lands of Arizona associated with the brown dog tick, Rhipicephalus sanguineus sensu lato (Demma et al, 2005). The peridomestic nature of R. sanguineus s.l. with canines and humans supports the cycle of R. rickettsii transmission and maintenance (López-Pérez et al, 2020). Furthermore, the emerging overlap of tropical and temperate lineages of R. sanguineus s.l. may also influence the epidemiology of RMSF in the southwestern United States and northern Mexico where case fatality rates are unusually high (Foley et al, 2019; Villarreal et al, 2018). High incidence of RMSF in this region might contribute to the disproportionate burden of spotted fevers in Native American populations.
The geographic distribution of reported cases of spotted fevers remained relatively unchanged from 2010 to 2018, with highest incidence forming a “belt” from the midwest to the east coast (Fig. 2). The state of Arkansas had 6850 cases (18.70% of the total), followed by Tennessee (N = 4892, 13.35%), North Carolina (N = 4081, 11.14%), Missouri (N = 3222, 8.80%), Alabama (N = 2889, 7.89%), Virginia (N = 2814, 7.68%), and Oklahoma (N = 2300, 6.28%).
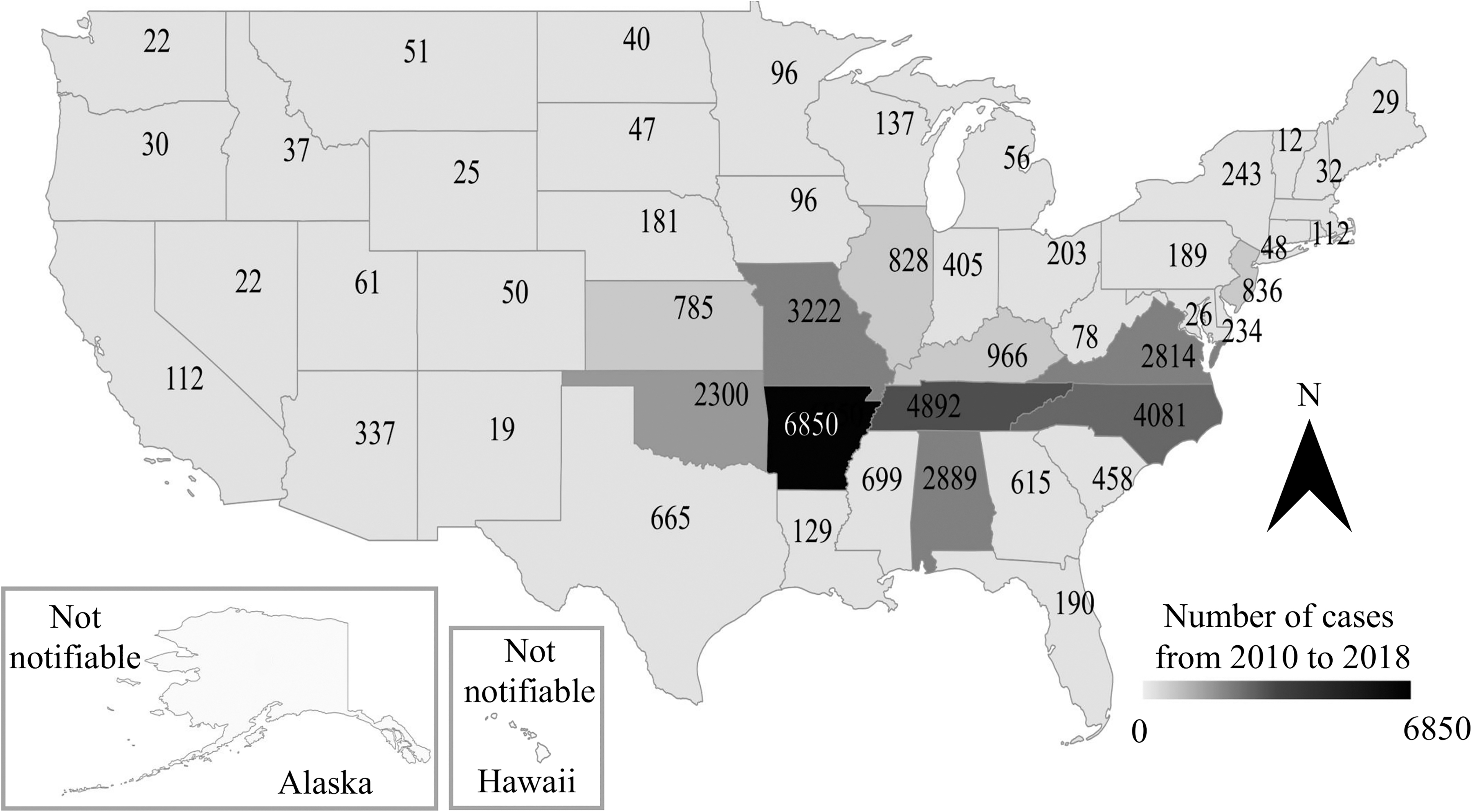
Spatial pattern of reported cases of spotted fever group rickettsioses in the United States from 2010 to 2018 (N = 36,632) based on data from the Nationally Notifiable Diseases Surveillance System.
These results are similar to an earlier summary by Openshaw et al (2010), who reported the highest number of cases, accounting for two-thirds of the total, occurred in Oklahoma, Missouri, Arkansas, Tennessee, and North Carolina. According to our study, Arkansas had the highest average incidence (256.84) from 2010 to 2018, whereas the lowest incidence (excluding Hawaii and Alaska where spotted fevers were not notifiable) occurred in California (0.32).
Seasonally, the reported cases of spotted fever were lowest in January, February, and March, and highest in June, July, and August (Fig. 3). The higher occurrence of reported cases during summer months may be associated with the concurrence of increased outdoor activity of humans from spring through summer when there is increased host-seeking activity by immature and adult ticks, including vectors in the genera Dermacentor and Amblyomma. Regionally, Rickettsia exposure through tick activity will vary with climate, host diversity and distribution, and relevant vector species.
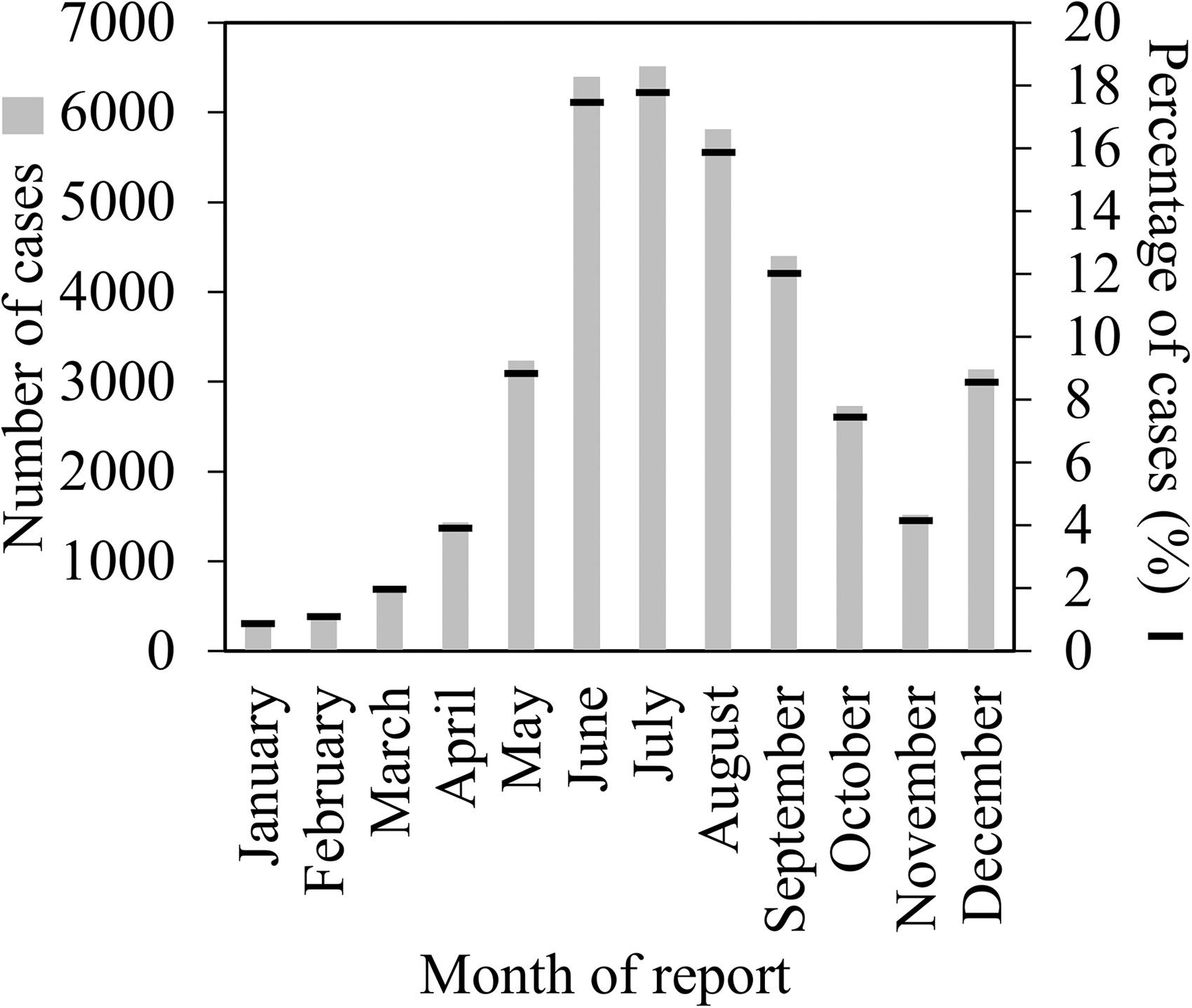
Month of report of spotted fever group rickettsiosis cases in the United States from 2010 to 2018 (N = 36,632) based on data from the Nationally Notifiable Diseases Surveillance System.
The increased feeding activity is augmented by the increased availability of (nonhuman) vertebrate hosts, which can result in the maintenance of high tick population densities (Wang et al, 2016; Wang et al, 2015; Wang et al, 2012). Thus, southern regions exhibit higher incidence both earlier and later during the year than in northern regions, and peak incidence can occur later during the fall.
Continuous improvement in the knowledge of tick ecology including activity, distribution, and abundance and their vector capacities relates to individual and population risk factors for contracting spotted fever rickettsioses and could consequently increase the efficacy of tick surveillance and control practices across the United States (Eisen and Paddock, 2020; Mader et al, 2021). Keeping up with changes in tick and tick-borne disease distribution and ecology is a continuous challenge.
In addition to expanding ranges for major vectors of spotted fever group rickettsioses such as Amblyomma americanum (Raghavan et al, 2019), Amblyomma maculatum Koch sensu lato (Paddock and Goddard, 2015), and Dermacentor variabilis (Sanders et al, 2013), new discoveries further underscore the need for continuous surveillance, for updates in education, and the need for an informed public health infrastructure. For example, A. americanum frequently carry R. amblyommatis, another member of the spotted fever group, with the prevalence of tick infection reaching 84% in some populations in nature (Levin et al, 2018). Recent tick surveys identified the progressive northward invasion of A. americanum, contributing to the increased number of patients with febrile illnesses of unknown etiology after a tick bite in the northeastern United States (Sonenshine, 2018).
Even though R. amblyommatis has not been isolated from patients, and the quantitative and qualitative natures of R. amblyommatis transmission during tick bloodmeal remain unknown, Yen et al (2021) found their results from a mice model corroborate clinical and serological evidence that R. amblyommatis may cause self-limiting mild febrile illnesses in humans and other mammals. Snellgrove et al (2021) also suggested that R. amblyommatis can cause either subclinical or mild infections based on their guinea pig model. Moreover, the invasive Asian longhorned tick, Haemaphsyalis longicornis, has been found in 17 states, including Arkansas, Missouri, North Carolina, Tennessee, and Virginia (United States Department of Agriculture, 2021).
Recent laboratory studies indicate H. longicornis may be a competent vector of R. rickettsii, but how its presence in the United States will affect the maintenance or spread of R. rickettsii and the future incidence of spotted fever group rickettsioses is unknown (Stanley et al, 2020). The discovery of human cases of R. parkeri in the southwestern United States (Herrick et al, 2016) and of R. parkeri infected A. maculatum s.l. populations in unique ecological environments in Arizona, New Mexico, and Texas (Hecht et al, 2020; Paddock et al, 2020) provides evidence of another spotted fever risk to human populations in the border regions.
In closing, we note that the coronavirus disease 2019 (COVID-19) pandemic (2020–to date) may have a noticeable impact on the reported incidence of spotted fevers and other tick-borne illnesses in the United States. Wormser et al (2021) reported three specific cases of individuals seeking care for treatable tick-borne infections in which their diagnosis was delayed due to issues arising from the COVID-19 pandemic. Concerns about spreading COVID-19 have reduced outpatient visits with health care providers and patients who seek care are required to test negative for COVID-19 before being tested for tick-borne infections, thus leading to delay in diagnosis and treatment (Rubin, 2020). Thus we can expect a COVID-19–related downward bias in reported incidence for at least the years 2020 and 2021.
Conclusion
The increasing incidence of spotted fever group rickettsioses in the United States is an issue of national importance. Analysis of long-term trends in reported cases informs our response to this public health issue. This study provides continuity to the shorter term trends in reported spotted fever incidence described previously (2016–2017, Heitman et al, 2019; 2008–2012, Heitman et al. 2016) by incorporating the 2013–2015 and 2018 data. Analysis of the 2010–2018 data indicates number of new cases reported annually approximately tripling during this period.
Disease mitigation strategy can be partially informed by increasing the percentage of confirmed cases compared with probable cases. Currently, the use of a single elevated IgG titer result for diagnosis of a probable case of spotted fevers may produce a skewed understanding of spotted fever epidemiology and national disease burden (CDC, 2020). RMSF is more severe than other spotted fevers, so failing to properly identify the species of Rickettsia hinders a proper understanding of spotted fever epidemiology and how the public is affected (Biggs et al, 2016). Efforts to increase the percentage of confirmed cases by species of spotted fever group rickettsia should be given a high priority.
Footnotes
Acknowledgments
We thank two anonymous reviewers for their time and effort.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.