
Abstract
Background:
Crimean–Congo hemorrhagic fever virus (CCHFV) causes a highly contagious tick-borne disease with high case-fatality rates in humans. It is circulating not only in many Asian and African countries, but also spreading to and within Europe. To cope better with future outbreaks of Crimean–Congo hemorrhagic fever (CCHF), the WHO has prioritized the need for the development and validation of CCHF diagnostics, including serological assays. In this study, we evaluated the performance of the new EUROIMMUN anti-CCHFV IgM and IgG enzyme-linked immunosorbent assays (ELISAs).
Materials and Methods:
Both ELISAs were compared to the Vector-Best VectoCrimean-CHF-IgM and -IgG ELISAs using the EUROIMMUN CCHFV Mosaic 2 IgM and IgG indirect immunofluorescence assays (IFA) as reference. Forty-nine acute-phase serum samples from patients with CCHFV infection confirmed by reverse transcription-polymerase chain reaction (RT-PCR) and/or anti-CCHFV IgM IFA positivity were used to determine assay sensitivity. The assessment of specificity was based on sera from 30 control patients, 30 healthy blood donors, and 29 patients with hantavirus or sandfly fever virus infections. All samples originated from Turkey.
Results:
Sensitivity of the EUROIMMUN ELISAs (IgM 98.0%, IgG 47.1%) exceeded that of the Vector-Best ELISAs (IgM 95.9%, IgG 35.3%). Specificity of the EUROIMMUN ELISA IgM (86.4%) was slightly higher compared with the Vector-Best ELISA IgM (84.7%), while specificity for IgG was 100% for both assays. Qualitative agreement between the EUROIMMUN and Vector-Best ELISAs was substantial for detecting anti-CCHFV IgM (84.1%, ĸ = 0.673) and IgG (94.9%, ĸ = 0.791), whereas the quantitative results indicated a very strong positive correlation (IgM: r = 0.868, IgG: r = 0.913).
Conclusion:
The new EUROIMMUN anti-CCHFV ELISAs are standardized and easy-to-use tools that reliably support the identification of acute CCHF cases, and thus suitable for laboratories involved in on-site outbreak support.
Introduction
Crimean–
The virus circulates in a tick–vertebrate–tick cycle. Humans contract an infection either directly through tick bites or by contact with blood or tissues of viremic animals (e.g., farmers, slaughterers, veterinarians) or humans (e.g., health care workers). Sexual, intrauterine, or perinatal transmission is also possible (Ergonul et al. 2010, Ergonul 2012, Bente et al. 2013, Pshenichnaya et al. 2016, Fillatre et al. 2019, Yagci-Caglayik et al. 2020, Shahhosseini et al. 2021). The occurrence of CCHF closely overlaps with the habitat of ticks of the genus Hyalomma and has reached the most extensive geographic distribution among medically important tick-borne diseases. Outbreaks and sporadic cases have occurred in Africa, the Middle East, in Asia, and Southeastern Europe (Maltezou et al. 2010, Fillatre et al. 2019, Monsalve-Arteaga et al. 2020a, Nasirian 2020, Shahhosseini et al. 2021).
In Turkey, CCHF was first described in 2002 and the country now has the highest number of laboratory-confirmed CCHF cases worldwide (Karti et al. 2004, Yilmaz et al. 2009, Leblebicioglu et al. 2016, Ak et al. 2020), with circulating CCHFV strains falling into clade Europe-1 and Europe-2 (Shahhosseini et al. 2021). Moreover, autochthonous human infections have been observed in Spain since 2016 (European Centre for Disease Prevention and Control 2021, Portillo et al. 2021). CCHF (re-)emergence in Southeastern and Southern Europe results from climatic, ecologic, and anthropogenic factors that influence the host-tick-virus dynamics. According to risk models, the ongoing climate change in the Mediterranean region will lead to an increase and northward expansion of the Hyalomma marginatum habitat areas in the future (Estrada-Pena and Venzal 2007). In addition, changes in land use that permit the massive proliferation of vertebrate hosts and ticks can contribute to CCHFV transmission (Gargili et al. 2017).
The estimated number of human CCHFV infections worldwide amounts to 10,000–15,000 per year, the vast majority (about 90%) remaining subclinical and unnoticed (Bodur et al. 2012, Hawman and Feldmann 2018). In some patients, however, the infection develops into a serious or fatal disease. Initial suspicion of CCHF is based on clinical findings in the context of an appropriate exposure history. The incubation period (up to 9 days) is followed by a sudden onset of unspecific symptoms, such as high fever, myalgia, headache, diarrhea, nausea, and vomiting (prehemorrhagic period, 1–7 days). Hematological and biochemical evaluation typically reveals leukopenia, thrombocytopenia, and elevated liver enzymes. Subsequently, patients may develop hemorrhagic manifestations at various body sites and organ failure (hemorrhagic period, 2–3 days), associated with fatality rates ranging from 5% to ≥30% (Ergonul 2012, Bente et al. 2013, Fillatre et al. 2019, Nasirian 2020).
CCHF-associated hemorrhagic manifestations rank among the most severe of all hemorrhagic fevers. As internationally approved vaccines and antivirals are not available due to the lack of randomized clinical trials, supportive treatment is still the mainstay of CCHF management (Fillatre et al. 2019).
To guide early therapeutic decisions and to take timely measures for infection prevention and outbreak control, clinically suspected CCHF has to be confirmed as fast as possible. However, there is currently neither a universally accepted gold standard for CCHFV diagnostics nor international reference reagents for calibrating and harmonizing assays (World Health Organization 2019). Reverse transcription-polymerase chain reaction (RT-PCR) is primarily used for diagnosing active CCHFV since it enables highly sensitive detection and quantification of virus RNA at the earliest stage. However, its application is impaired by the wide genetic diversity of CCHFV strains and limited to the viremic phase. Results turn negative after several days of disease except for patients with fatal outcome who have persistently high viral loads until death (Drosten et al. 2003, Cevik et al. 2007, Wolfel et al. 2007, Ergonul 2012, Kaya et al. 2014, Bartolini et al. 2019).
To maximize diagnostic sensitivity, a combination of molecular and serological testing has been proposed (Ergonul 2012, Bente et al. 2013, Bartolini et al. 2019, Mazzola and Kelly-Cirino 2019).
The major target of the immune response against CCHFV is the N protein (Dowall et al. 2016). N-specific IgM becomes detectable after a median of 2–3 days after onset of symptoms and glycoprotein-specific IgM after 4–6 days, followed by IgG with a delay of 1–2 days after the IgM response (Ergunay et al. 2014). IgM reaches peak levels in the second and third week of disease and usually clears after about 4 months, while IgG persists for several years. The presence of IgM in a single sample or a greater than or equal to fourfold rise in IgG titers in two consecutive samples is evidence of a recent or current infection (Ergonul 2006, Fillatre et al. 2019).
Severe and fatal infections, however, are often serologically undetectable since the antibody response is typically weak or absent in these cases, leading to insufficient immunity and uncontrolled viremia (Kaya et al. 2014, Bartolini et al. 2019). Indirect immunofluorescence assays (IFAs) and enzyme-linked immunosorbent assays (ELISAs) are commonly used for antibody detection (Ergunay et al. 2014, Fernandez-Garcia et al. 2014, Schuster et al. 2016, Monsalve-Arteaga et al. 2020b, Emmerich et al. 2021). Although some commercial tests are available, most are marketed for research use only and many reference laboratories use in-house assays based on antigen derived from regional CCHFV strains (Bartolini et al. 2019, Mazzola and Kelly-Cirino 2019). In 2018/19, the WHO raised attention to the urgent need for the development and validation of CCHF diagnostic assays for use in reference laboratories as well as near-patient and point-of-care settings in CCHF-affected countries (World Health Organization 2019).
In this study, the diagnostic performance of two novel commercial ELISAs for the detection of CCHFV-specific IgM and IgG was evaluated against established CE-marked in vitro diagnostic IFA and ELISA tests.
Materials and Methods
Human serum samples
This study used leftover serum samples from routine CCHF diagnostic procedures carried out at the Microbiology Reference Laboratories Department affiliated to the Public Health General Directorate of Turkey (Ankara, Turkey). To confirm infection with CCHFV, samples had previously been analyzed by RT-PCR (either singleplex [RealStar CCHFV RT-PCR Kit; Altona Diagnostics, Hamburg, Germany] or multiplex [Bio-Speedy CCHF PCR Kit; Bioeksen, Istanbul, Turkey]) and by anti-CCHFV IFA. Patients with positive RT-PCR and/or with specific IgM antibodies detected by IFA were defined as having CCHFV infections (panels A and B), as described previously (Vanhomwegen et al. 2012). The following five serum panels were investigated, with details provided in Table 1.
Characteristics of Patients and Controls
In Panel B, two sets of samples were collected: the first set (n = 19, 0–8 DPSO) was used for RT-PCR analysis, while the second set (n = 19, 6–18 DPSO) was used for serological testing. In panels A and C, molecular and serological testing was carried out in a single set of samples.
CCHF, Crimean–Congo hemorrhagic fever; CCHFV, Crimean–Congo hemorrhagic fever virus; DPSO, days postsymptom onset; HNTV, hantavirus; IFA, indirect immunofluorescence assay; ND, no data; RT-PCR, reverse transcription-polymerase chain reaction; SD, standard deviation; SFV, sand fly fever virus.
Panel A (CCHF patient sample group I) consisted of 30 single serum samples collected 0–15 days postsymptom onset (DPSO; mean 6.2 DPSO) from a cohort of Turkish patients at risk for being infected with CCHFV (e.g., residing in or traveling to a CCHFV endemic region, history of tick bite, contact with animal blood/skin/body fluid, occupational risk of infection). The geographical distribution of patients' residencies in Turkey is shown in Supplementary Fig. S1. The patients' clinical symptoms and biochemical findings were consistent with CCHF. Infection with CCHFV was confirmed by positive RT-PCR in 20/30 (66.7%) cases and anti-CCHFV IgM positivity by IFA in 30/30 (100%), including 17 (56.7%) with positive anti-CCHFV IgG findings by IFA.
Panel B (CCHF patient sample group II) comprised paired serum samples from 19 Turkish CCHF patients. The geographical distribution of patients' residencies in Turkey is shown in Supplementary Fig. S1. Initial samples were collected 0–8 DPSO (mean 3.2 DPSO) and yielded positive RT-PCR results in 19/19 (100%) of cases. Follow-up samples were obtained 6–18 DPSO (mean 11.4 DPSO), revealing a positive anti-CCHFV IgM status by IFA in 19/19 (100%) patients, who all had clinical and biochemical findings typical for CCHF. Among these patients, 17 (89.5%) were anti-CCHFV IgG positive by IFA. Only the follow-up samples were available for serological analysis in the present study.
Panel C (control sample group) consisted of 30 single serum samples collected 0–35 DPSO (mean 4.3 DPSO) from Turkish patients belonging to the same at-risk cohort as those in Panel A, in part, presenting signs and symptoms consistent with CCHF. However, CCHFV infection was disproved by negative results using CCHFV-specific RT-PCR and IFA (IgM/IgG).
Panel D (healthy sample group) comprised 30 serum samples taken from Turkish blood donors who had neither CCHF-related clinical symptoms nor chronic illness. These samples had been tested negative for anti-CCHFV IgG by IFA (anti-CCHFV IgM IFA had not been performed on panel D). Additional molecular and serological data showed negativity for West Nile virus, hepatitis B virus, and human immunodeficiency virus.
Panel E (cross-reactivity sample group) consisted of 29 serum samples from suspected cases with a serologically confirmed prediagnosis for hantavirus or sand fly fever virus infection (Supplementary Table S1). These samples had been tested negative for anti-CCHFV IgM and IgG by IFA.
Indirect immunofluorescence assay
The Crimean–Congo Fever Virus Mosaic 2 IgM and IgG IFA (EUROIMMUN, Lübeck, Germany) had been used for serological precharacterization of the study samples. In this assay, each reaction field contains three biochips coated with transfected EU90 cells separately expressing recombinant GPC or N antigen, and control-transfected cells. Incubation was performed according to the manufacturer's instructions, followed by assessment of the slides through fluorescence microscopy. Reactivity at a dilution of 1:10 (IgM) or 1:100 (IgG) was interpreted as positive result. In positive samples, immunofluorescence was graded according to intensity levels (1+ to 4+).
Enzyme-linked immunosorbent assays
The anti-Crimean–Congo fever virus IgM ELISA and anti-Crimean–Congo fever virus IgG ELISA from EUROIMMUN are based on microplates coated with recombinant N antigen from CCHFV. The assays were performed and evaluated according to the manufacturer's instructions. Briefly, sera diluted 1:101 in sample buffer (EUROIMMUN) were added to the wells and allowed to react for 60 min at 37°C. Before IgM detection, sera were preincubated with sample buffer containing IgG/rheumatoid factor absorbent (EUROIMMUN) to remove IgG. Bound antibodies were detected by applying goat anti-human IgM peroxidase conjugate or rabbit anti-human IgG peroxidase conjugate for 30 min at room temperature. A chromogen/substrate solution (tetramethylbenzidine/H2O2) was added to induce a color reaction for 15 min. The enzymatic reaction was stopped with 0.5 M sulfuric acid. Optical density (OD) was measured photometrically at 450 nm (reference 620 nm). Anti-CCHFV IgM levels were determined as ratio values (extinctionsample/extinctioncalibrator), with ratios <0.8 considered negative, ≥0.8 to <1.1 borderline, and ≥1.1 positive. Anti-CCHFV IgG levels were quantified using a 3-point calibration curve prepared from calibrators that cover a range from 2 to 200 relative units (RU)/mL. Results <16 RU/mL were considered negative, ≥16 to <22 RU/mL borderline, and ≥22 RU/mL positive.
The VectoCrimean-CHF-IgM ELISA from Vector-Best (Novosibirsk, Russia) has a μ-capture format, while the VectoCrimean-CHF-IgG ELISA is an indirect ELISA using immobilized CCHFV antigen. Information on the precise nature of the antigen is not available (Emmerich et al. 2021). Both Vector-Best ELISAs were performed and evaluated according to the manufacturer's instructions. Results (ODs) were interpreted as follows: negative if ODsample < 0.8 × ODcontrol, borderline if 0.8 × ODcontrol ≤ ODsample ≤ ODcontrol, and positive if ODsample > ODcontrol.
Measurements yielding inconclusive (borderline) results were not repeated due to insufficient sample volume. For the same reason, samples with results above the analytical range or outside the detection limit of the plate reader were not rerun at a higher dilution and are presented in graphs as data points with OD values of 3.0 (this applies only to Vector-Best ELISA measurements).
Statistics
Confidence intervals (CIs) were calculated according to the modified Wald method. Interassay concordance was assessed using percentage of agreement between qualitative results. To correct the agreement for the probability of random coincidence, the Cohen's kappa coefficient (ĸ) was calculated. Kappa values from 0 to 0.20, 0.21 to 0.40, 0.41 to 0.60, 0.61 to 0.80, and 0.81 to 1.00 indicate slight, fair, moderate, substantial, and almost perfect agreement, respectively (Landis and Koch 1977). For the calculation of sensitivity, specificity, and concordance, borderline results (accounting for 11/276 [4.0%] of all anti-CCHFV IgM and IgG determinations) were considered positive. Pearson's correlation coefficients were determined to assess the degree of correlation between assays. p Values <0.05 were considered significant. Statistical analyses were conducted using GraphPad QuickCalcs (GraphPad Software, Inc., San Diego, CA) and SigmaPlot 13.0 (SSI, San Jose, CA).
Ethics statement
The study complies with the Declaration of Helsinki in its current version (World Medical Association 2013). Written informed consent from patients and ethics council consent were not required as only anonymized patient data and diagnostic leftover samples were used for this retrospective study.
Results
Diagnostic performance of the EUROIMMUN anti-Crimean–Congo fever virus ELISAs
By reason of lack of a gold standard in CCHFV serology, the EUROIMMUN ELISAs were validated against the EUROIMMMUN Crimean
The EUROIMMUN IgM ELISA correctly recognized 48/49 of the CCHF patient samples, corresponding to a sensitivity of 98.0% (panel A+B). The assay yielded negative anti-CCHFV IgM results in 51/59 control and potentially cross-reactive samples, indicating a specificity of 86.4% (panel C+E) (Table 2). Among specificity samples, anti-CCHFV IgM was exclusively detected in anti-hantavirus or anti-sand fly fever virus IgM-reactive cases in panel E (Fig. 1A and Supplementary Table S1).

Determination of anti-CCHFV antibodies by EUROIMMUN and Vector-Best ELISAs. (
Diagnostic Performance of Anti-Crimean
Borderline results were considered positive.
EUROIMMUN Crimean–Congo Fever Virus Mosaic 2 IFA IgM/IgG as reference.
Panel D was analyzed for CCHFV-specific IgM by ELISA, but not by IFA. Due to the lack of IgM IFA data, sensitivity and specificity of the IgM ELISAs could not be determined in this panel.
In-house IFA IgM/IgG as reference.
CI, confidence interval; ELISA, enzyme-linked immunosorbent assay.
Using the EUROIMMUN IgG ELISA, anti-CCHFV IgG positivity was correctly detected in 16/34 patient samples, corresponding to a sensitivity of 47.1% (panel A+B). Among the control samples, negative results for anti-CCHFV IgG were obtained in 89/89 cases, reflecting a specificity of 100% (panel C+D+E) (Table 2 and Fig. 1B).
Comparison of the EUROIMMUN anti-Crimean–Congo fever virus ELISAs with the Vector-Best VectoCrimean-CHF ELISAs
The performance of the Vector-Best ELISAs was also assessed using the EUROIMMUN IFA as reference. The Vector-Best IgM ELISA was 2.1% less sensitive than the EUROIMMUN IgM ELISA (95.9% vs. 98.0%, panel A+B) and 1.7% less specific (84.7% vs. 86.4%, panel C+E) (Table 2). Among specificity samples, the Vector-Best IgM ELISA measured borderline or positive anti-CCHFV IgM levels not only in panel E, but also in panels C and D (Fig. 1C and Supplementary Table S1).
Assessment of IgG reactivity demonstrated a 11.8% lower sensitivity of the Vector-Best IgG ELISA compared with the EUROIMMUN IgG ELISA (35.3% vs. 47.1%, panel A+B) at equally high specificity (100%, panel C+D+E) (Table 2 and Fig. 1D).
Agreement rates between qualitative ELISA results were determined separately for each serum panel and for the total of 138 samples. Out of 59 samples testing anti-CCHFV IgM positive by Vector-Best IgM ELISA, 47 were positive by EUROIMMUN IgM ELISA, corresponding to a positive agreement rate of 79.7%. Among 79 samples categorized as IgM negative by Vector-Best IgM ELISA, 69 had also a negative result by EUROIMMUN IgM ELISA, resulting in a negative agreement rate of 87.3%. Based on the correlation of positive and negative results in altogether 116/138 cases, the total agreement between both ELISAs amounted to 84.1%. The kappa coefficient indicated substantial qualitative agreement between both assays (ĸ = 0.673) (Table 3). Pearson analysis revealed a very strong positive, statistically significant association between the quantitative IgM data of both assays (r = 0.8680, p < 0.0001) (Fig. 2A).
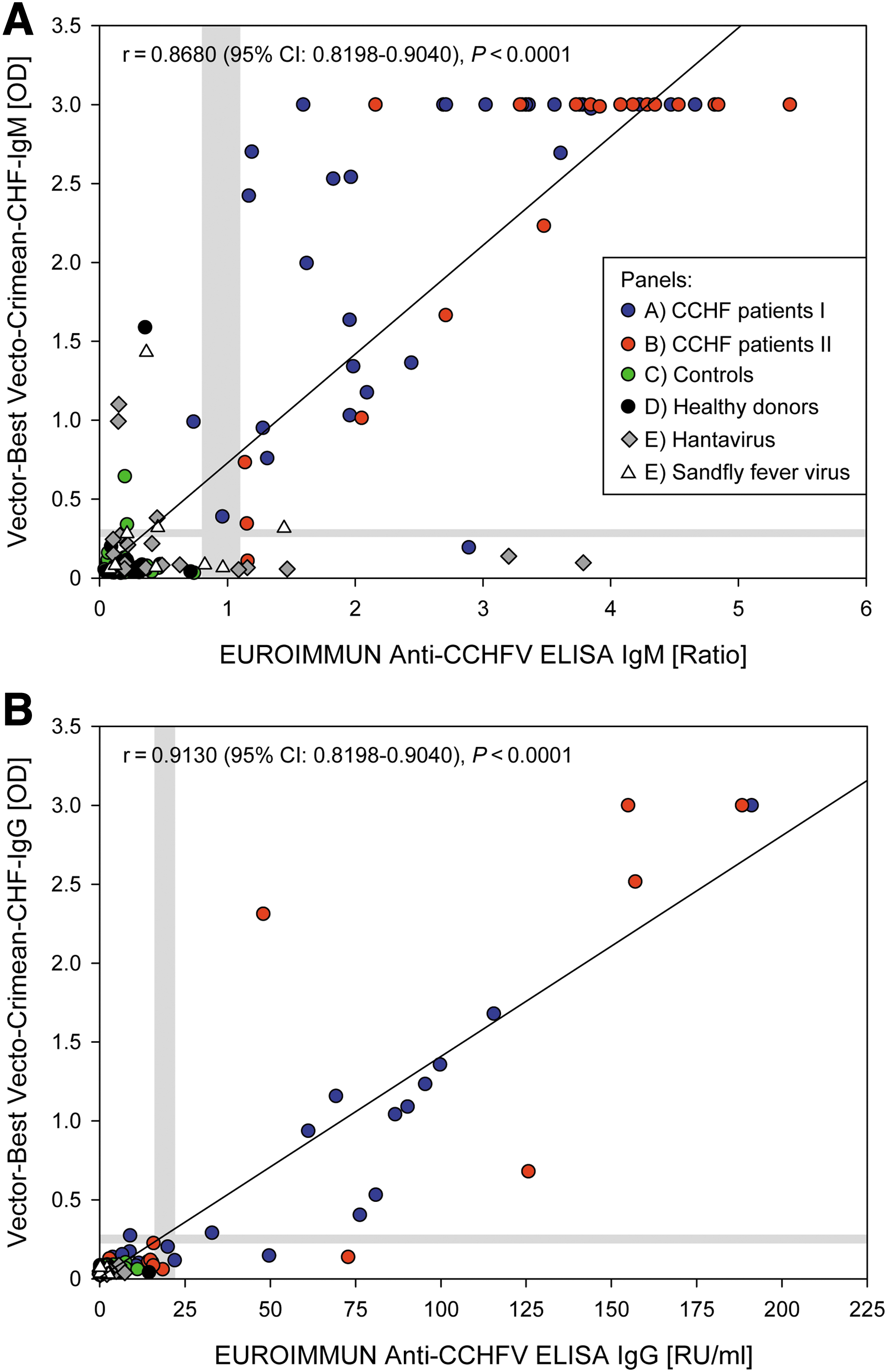
Correlation between anti-CCHFV levels measured by Vector-Best ELISA versus EUROIMMUN ELISA. (
Concordance Between Qualitative Enzyme-Linked Immunosorbent Assay Results (Irrespective of Indirect Immunofluorescence Assay Precharacterization)
Borderline results in ELISA were considered positive.
The positive, negative, and total agreement between the EUROIMMUN IgG ELISA and the Vector-Best IgG ELISA amounted to 16/18 (88.9%), 115/120 (95.8%) and 131/138 (94.9%%), respectively. According to kappa statistics, the interassay agreement was classified as substantial (ĸ = 0.791) (Table 3). The quantitative results of both IgG ELISAs demonstrated very a strong positive, significant correlation (r = 0.9130, p < 0.0001) (Fig. 2B).
Discussion
CCHF (re-)emergence poses a major public health threat considering the associated contagion risks, potential lethality, and difficulties in disease prevention, treatment, and control (Ergonul 2012). Therefore, rapid case identification and adequate infection control measures are crucial in outbreak management. This in turn requires efficient surveillance, sufficient clinical and laboratory capacities, as well as availability of reliable, simple-to-use, validated, and easily accessible diagnostic assays for use in endemic regions (Maltezou et al. 2010, World Health Organization 2019). Commercial assays fulfilling these criteria enable local laboratories to perform fast CCHF serodiagnosis at moderate biosafety levels, thereby overcoming the common approach of shipping relevant samples to reference laboratories (abroad). This would result in reduced time and costs per analysis as well as diminished effort and risks associated with the shipment of highly contagious material.
Several commercial and in-house CCHFV serology tests are used in research and diagnostics (Fernandez-Garcia et al. 2014, Bartolini et al. 2019, Mazzola and Kelly-Cirino 2019), the EUROIMMUN IFA and Vector-Best ELISAs being the most commonly applied commercial assays (Vanhomwegen et al. 2012, Emmerich et al. 2018, 2021). To our knowledge, this is the second study (after Emmerich et al.) assessing the performance of the EUROIMMUN anti-CCHFV IgM and IgG ELISAs (Emmerich et al. 2021), which were recently brought to the market for in vitro diagnostic purposes (CE-IVD).
ELISA performance was evaluated against the EUROIMMUN IFA, which is used for routine diagnostics at the study site. The recombinant IFA method is based on eukaryotic cells expressing virus antigens in their native confirmation, including posttranslational modifications, resulting in high sensitivity, whereas the fluorescence staining patterns aid the assessment of signal specificity. According to the manufacturer, this IFA provides a sensitivity and specificity of 97.2% and 97.5% for IgM, and 89.5% and 100% for IgG, respectively (EUROIMMUN 2022). Similarly, a study by Vanhomwegen et al. (2012) found 93.9% sensitivity and 98.9% specificity for the IgM IFA as well as 86.1% and 100% for the IgG IFA.
Using the IFA as reference, the EUROIMMUN ELISAs yielded sensitivities of 98.0% for IgM and 47.1% for IgG in acute-phase samples (panels A+B: 8.2 ± 4.3 DPSO, range 0–18 DPSO), at specificities of 86.4% and 100%, respectively. Consistent with our results, Emmerich et al. (2021) reported for the EUROIMMUN ELISAs sensitivities of 100% (IgM) and 52% (IgG) in the acute phase of infection (9.8 ± 2.3 DPSO, range 6–14 DPSO), at 98.3% specificity. The relatively low sensitivity of the IgG ELISA compared with IFA may be caused by differences in the preparation and presentation of antigens, such as the competence of recombinant eukaryotic IFA cell substrates to produce authentic quaternary structured antigens. Importantly, the limited sensitivity of the EUROIMMUN IgG ELISA among acute-phase samples does not constitute a diagnostic gap, since serodiagnosis of acute infections is primarily based on IgM testing.
Detection of IgG, however, is of major relevance for disease monitoring, epidemiology and surveillance purposes. In that respect, the value of the EUROIMMUN IgG ELISA is reflected by a sensitivity of 98.8% among cases with subsided CCHF (≥28 DPSO), as reported elsewhere (Emmerich et al. 2021).
Comparison between the EUROIMMUN and Vector-Best IgM ELISAs demonstrated almost equal sensitivities (98.0% vs. 95.9%) and specificities (86.4% vs. 84.7%). The limited specificity in IgM detection was primarily due to cross-positive reaction rates among hantavirus- or sand fly fever virus-seropositive samples, which amounted to 27.6% and 31.0% for the EUROIMMUN and Vector-Best IgM ELISAs, respectively. Similarly, in another study, an anti-CCHFV IgM positivity rate of 5.6% was reported for hantavirus-infected patients, but not for sand fly fever virus- or Toscana virus-infected cases (EUROIMMUN 2021a, 2021b). Hence, cross-reactions within the Bunyavirales order cannot be excluded for either assay. Emmerich et al. (2021) reported 100% sensitivity (100% specificity) for the Vector-Best IgM ELISA in acute-phase sera, whereas Vanhomwegen et al. (2012) found only 87.8% sensitivity (98.9% specificity) in a mixed panel of acute and convalescent cases (5 to 49 DPSO).
Moreover, our data revealed that the EUROIMMUN IgG ELISA was 11.8% more sensitive than the Vector-Best IgG ELISA (47.1% vs. 35.3%), at equally excellent specificity (100%). In other studies, sensitivity of the Vector-Best IgG ELISA ranged between 12.0% among acute cases (Emmerich et al. 2021) and 80.4% in samples collected during the acute and convalescent phase (Vanhomwegen et al. 2012), each at 100% specificity. Overall agreement between the qualitative results of both ELISA systems amounted to 84.1% (ĸ = 0.673) for IgM and 94.9% (ĸ = 0.791) for IgG in the present study, indicating substantial agreement. Interestingly, Emmerich et al. (2021) found almost perfect agreement between the EUROIMMUN and Vector-Best IgM ELISAs based on acute (ĸ = 0.97) or convalescent (ĸ = 0.95) samples, whereas agreement between the IgG ELISAs was only slight (ĸ = 0.18) in the acute phase and substantial (ĸ = 0.79) in the convalescent phase.
These differences in sensitivity and agreement indicate that the diagnostic performance of the test systems varies with respect to the phase of infection (Emmerich et al. 2021). The nature of the antigen used in the Vector-Best ELISAs may be an explanation for some of the discrepant results, but this remains speculative as information on the coated antigen (e.g., CCHFV strain, whole-virus antigen or recombinant N protein) is publicly not available (Emmerich et al. 2018, 2021, Bartolini et al. 2019).
Limitations of this study include the low number of samples in each panel, resulting in wide CIs and the need to interpret results with caution. Moreover, samples for the assessment of sensitivity in convalescent patients were not available, leading to limited information on assay performance at later stages of disease.
Conclusion
The novel EUROIMMUN Anti-CCHFV IgM ELISA reliably detects acute CCHF cases based on high sensitivity, specificity, and agreement rates compared with established commercial assays. Assay performance in late convalescent and subsided infections was not addressed here, but an independent study (Emmerich et al. 2021) already revealed the value of the IgG ELISA for disease monitoring, epidemiology, and surveillance purposes. Since equipment and evaluation expertise are less complex than for other serological methods, these ELISAs are highly suitable for on-site laboratories involved in outbreak assistance.
Footnotes
Acknowledgments
We want to thank all the physicians, assistant health personnel, and laboratory staff involved in the management of these CCHF patients.
Authors' Contributions
Y.C., K.S., J.M.K., and G.K. were responsible for the conception and design of the study. Y.C. and G.K. performed the sample collection and assay runs. A.Ö.K., O.K., E.L., J.M.K., and S.S. were involved in data analysis and communication. The original draft was written by S.S. All authors had access to the data, revised and edited the article, and approved the final version.
Author Disclosure Statement
A.Ö.K., O.K., E.L., J.M.K., S.S., and K.S. are employed by EUROIMMUN Medizinische Labordiagnostika AG, a manufacturer of diagnostic reagents. The other authors declare no competing interests. Company staff were involved in data analysis and writing of the article. However, the contributions of EUROIMMUN employees were based exclusively on scientific grounds and transparent to and reviewable by all coauthors.
Funding Information
Assays and consumables were funded by EUROIMMUM Medizinische Labordiagnostika AG.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.