
Abstract
Background:
Highlighting the individual, host–vector interactions, and environmental risk factors for knowlesi malaria were consequential toward more focused and effective prevention and control strategies. This study aims to identify the individual, host–vector interactions, and environmental risk factors for Plasmodium knowlesi malaria among at-risk communities in Peninsular Malaysia.
Materials and Methods:
A case–control study was conducted involving laboratory-confirmed cases of P. knowlesi malaria, while a locality-matched individual with no history of fever and tested negative for malaria was taken as control. Univariate and multiple logistic regression were applied to evaluate the potential risk factors among respondents using IBM SPSS Statistics for Windows, Version 26.0.
Results:
Results showed higher cases among males as compared to females (76.1% vs. 23.9%). Multiple logistic regression analysis showed being male is 3.51 higher risk (p < 0.001) to become a case. Respondents whose place of work or study is near the forest edge have 44.0% lower risk (p = 0.030), while those living in the Orang Asli village were 56.0% lower risk as compared to the organized village to become a case (p = 0.035).
Conclusion:
These findings demonstrated that gender emerges as an independent individual risk factor while residing near a forest edge, in an Orang Asli village, or occupying workers’ longhouses situated in hilly areas lowered the environmental risk among respondents. These findings attested that alternative directions must be considered in addressing the known risk factors associated with this type of malaria and the design of prevention and control programs should be tailored to the unique characteristics of each population.
Introduction
The four plasmodia’s malaria groups known to the world—falciparum, malariae, vivax, and ovale—have caused a significant burden to the world, particularly the tropical countries. To add to this burden, in 1932, Knowlesi and Das Gupta discovered another malaria parasite, known as Plasmodium knowlesi, which is a type of monkey malaria. However, despite this early discovery, uncertainties surrounding its zoonotic potential caused it to be “left out” and thought to be only sporadic in nature (Moyes et al., 2014).
In recent years, there has been a significant increase in the number of cases and severity of this disease, which is affecting not just Southeast Asia but also gives rise to the possibility of global transmission. Studies have shown that the increase in human activities in previously sparsely populated areas, as well as the increase in the number of ecotourists, including in Malaysia, are among the main factors related to habitation and behavior that lead to the risk of acquiring this malaria of nonhuman primate origin (Wong et al., 2015). Additionally, the unavoidable intersection of human and monkey habitats due to large agricultural activities carried out by villagers, along with the adaptive abilities of both the parasites and the vectors, such as drug and insecticide resistance and behavioral adaptation, have further diminished the geographical gap between the two species. This proximity has led to a shared infestation by Anopheles mosquitoes, which served as the vector for malaria transmission to humans (White, 2008; Sabbatani et al., 2010; Ramasamy, 2014).
In Malaysia, there have been more than a few reported fatal cases of knowlesi malaria. Important practical lessons learned from the discussion of these cases include that humans can and do acquire monkey malaria if they share the same habitat, as the vector is attracted to both humans and monkeys (Singh and Daneshvar, 2013). Looking back at the epidemiology triad of disease, the interaction between agent–host–environment needs to be stopped to control the disease. The host, especially humans, plays a vital role in this interaction. This should be the core of inquiry, which helps researchers to identify all possible risk factors that put certain populations at higher risk of getting knowlesi malaria than others (the at-risk communities) (Fornace et al., 2019).
Individual risk factors play an important role in contracting this disease. A study conducted in Sabah between 2012 and 2015 (Grigg et al., 2017) has highlighted a few significant findings in terms of individual risk factors. For gender, findings show that men were four times more likely to have P. knowlesi infection than women, but although male farmers were more likely to contract monkey malaria, they were not at higher risk of contracting other types of malaria. Indoor work such as shopkeeping, traditional female household duties, and studying was associated with a lower risk of P. knowlesi malaria in these communities. In addition, humans working on the fringes of the forest are at risk of contracting knowlesi malaria, as well as in the forest itself when they carry out activities (Daneshvar et al., 2009). Apart from that, a few other studies also highlighted findings in terms of individual-level factors, such as that parasitemia and disease severity increase with age, severe knowlesi malaria is not yet reported in children less than 12 years old, and the youngest reported death to be 31 years (age range between 31 and 84) (Barber et al., 2013; Rajahram et al., 2016).
Regarding environmental risk factors, findings in a study conducted in Sabah highlighted that the agricultural sector contributes to the highest number of cases (82.2%), followed by forest-related activities such as logging and the collection of forest products (17.5%). In another study, in Kapit, Sarawak, the result shows that Anopheles latens mosquitoes prefer to feed humans and macaques at ground level. However, at a higher elevation, they prefer to feed macaques more than humans (Tan et al., 2008). In addition, humans who live in mountainous areas are at higher risk of getting infected. A combination of certain topographical regions, with the addition of climate suitability, also contributes to its population’s susceptibility toward malaria (Abiodun et al., 2016). Apart from that, Anopheles balabacensis, which is the main vector for P. knowlesi, breeds mostly in-ground pool water. Thus, rainfall and temperature play an important role in knowlesi malaria transmission. However, excess rainfall would also result in the flushing of the breeding site of the Anopheles mosquito (Barber et al., 2012; Abiodun et al., 2016).
In terms of host–vector interaction factors, previous research (Barber et al., 2013; Collins, 2012) shows that close proximity to the forest could bring humans into contact with the macaques and vector. The same study mentioned above, which was conducted in Sabah (Barber et al., 2013), reported that this is a significant risk factor as most of the traditional villages in Sabah are located near the forest edge and the source of income is usually related to forest products, thus increasing the chances of human–vector–animal contacts. In addition, the change in land use patterns has created an increased opportunity for the spillover of infections from monkeys to humans, which is through closer associations with natural reservoir hosts or access to infected vectors (Collins, 2012). Apart from that, population movement can precipitate or increase malaria transmission (IOM, 2013). As people move, they can increase their risk of acquiring the disease through the ways in which they change the environment and through the technology they introduce, for example, through deforestation and irrigation systems. Such activities result in increased exposure and host–agent interaction among workers to the vector.
Highlighting the specific risk factors, namely individual, host–vector interactions, and environment, in the epidemiological disease triad of P. knowlesi malaria infection is of paramount importance toward more focused and effective prevention and control strategies (Chin et al., 2021). Additionally, this will ensure the infection will cease as the main threat to Malaysia’s success of the National Malaria Elimination Strategic Plan. Thus, this study aims to identify the individual, host–vector interactions, and environmental risk factors for P. knowlesi malaria among at-risk communities in Peninsular Malaysia.
Material and Methods
Sampling and participants
The data collection was elicited through an interviewer-guided questionnaire. All laboratory-confirmed cases of P. knowlesi malaria patients were registered and notified to the online vector disease reporting system, Vekpro Online System, by the district health office, and primarily resided in the three preidentified study areas for a minimum of 3 weeks from January 2020 until December 2021 were included as cases. These three preidentified locations were the districts of Gua Musang (4.8843° N, 101.9682° E) in the state of Kelantan, Kuala Lipis (4.1843° N, 102.0542° E) in the state of Pahang, and Kota Tinggi (1.7289° N, 103.8991° E) in the state of Johor, Malaysia. Two of these locations (Gua Musang and Kuala Lipis) were in the eastcoast region, while Kota Tinggi is in the southern region of Peninsular Malaysia. The three preidentified areas mentioned above were selected because they are the three districts that recorded the highest number of cases of P. knowlesi malaria in Peninsular Malaysia in 2018 (Azlan et al., 2023).
Additionally, just as cases, a locality-matched individual with no history of fever and tested negative for malaria through a blood slide and PCR of the same duration was taken as a control. To determine whether age and gender were among the variables that significantly affect the status of respondents, these two variables were not matched between the case and control. Additionally, due to the complexity of the informed consent process for respondents whose ages were below 18 years old, only individuals aged 18 years or more were included in the study. The final number of the sample included for analysis was concluded after removing those who were relocated, had access issues, died, and closed the logging area. The flowcharts for selections of cases and controls are shown in Figures 1 and 2.
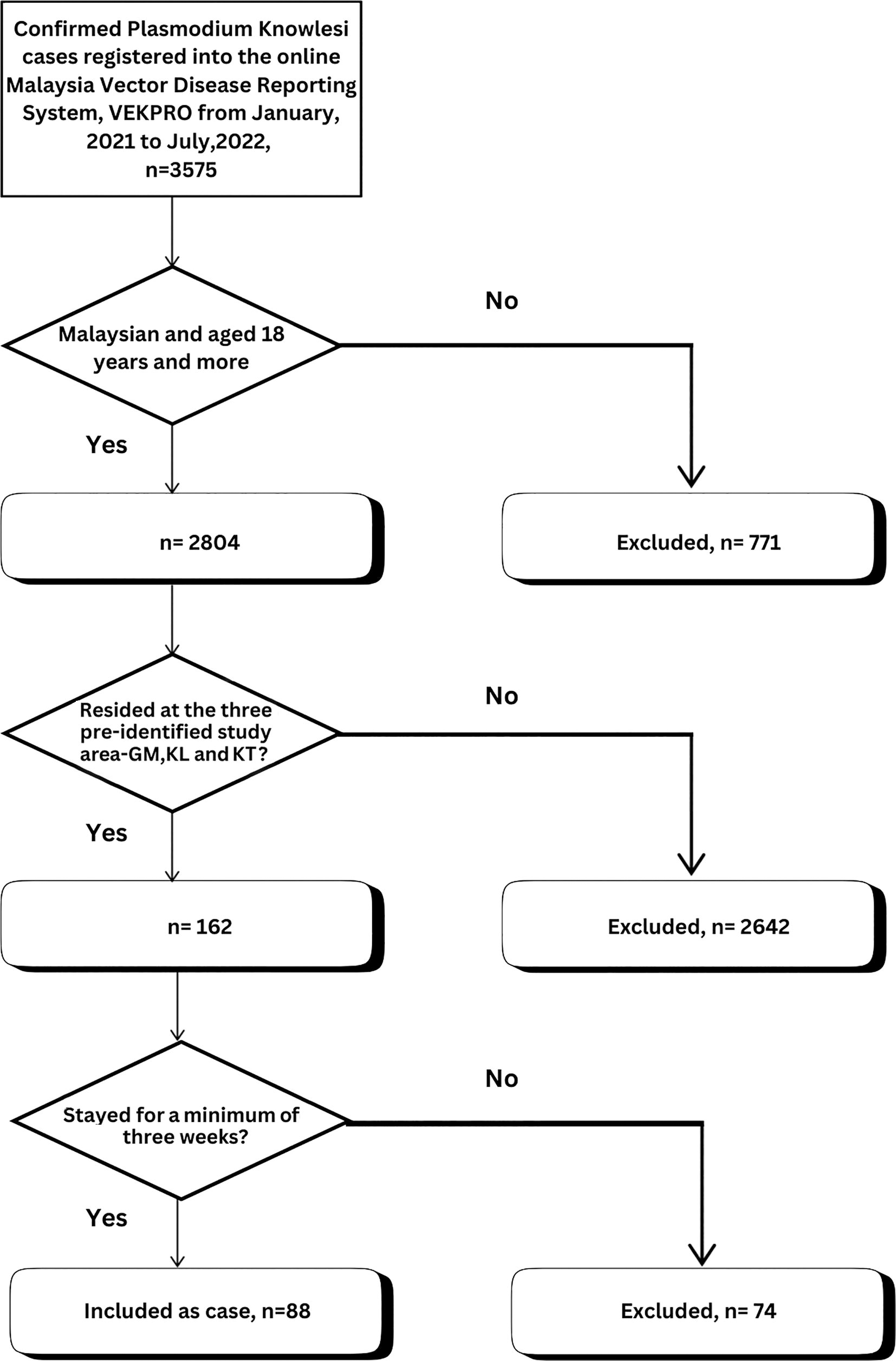
Flowchart for selections of cases. GM, Gua Musang; KL, Kuala Lipis; KT, Kota Tinggi.

Flowchart for selections of control.
For sample size, to detect the proportion difference of 0.12 with an alpha of 0.05 and power of study of 80.0%, we aim to get 150 cases and 600 controls to achieve a ratio of 1:4. This calculation was done using ScalexProp version 1.0.2 by Naing, 2016. However, over 2 years of data collection from 2020 to 2021 coincided with the nationwide movement control order imposed by the government due to the pandemic COVID-19 affecting the country. As a result, the total number of cases in the country, including the study locations, has reduced. We managed to get 88 cases with 352 controls to maintain the 1:4 ratio set for the study design after excluding. To ensure the sample size has enough power, a post hoc power was calculated based on the proportion of males among case and control (significant risk factors), and the result shows a post hoc power of more than 80.0%. Thus, validating the sample size achieved.
Measures
The tool used for data collection was a questionnaire. It was part of the more extensive questionnaire developed for nationwide research that aims to identify the most suitable multidisciplinary health intervention approach to improving knowlesi malaria health behavior among at-risk populations in Peninsular Malaysia. Thus, for this current study, the variables extracted were divided into individual, host–vector interactions and environment characteristics of the respondents’ house and housing areas, as well as their place of work and study.
The questionnaire on individual characteristics includes respondent’s status which is classified as either case or control based on the criteria stated above, their age in years (current year), gender as male or female, ethnic group which was classified as either Malay, Aborigine (“Orang Asli”), Indian, or others where they have to state their actual ethnicity, nationality as Malaysian or non-Malaysian, number of household members living together, smoking status as either current and ex-smoker or nonsmoker, working status as working or not working which may include pensioners, housewives, and last any history of being diagnosed with chronic diseases and required treatment from hospitals or clinic.
Focusing on the host–vector interactions, the questions asked include activities that have the potential for the interactions to occur. These include the geographical conditions of their working address, which is either forest, forest edge, hilly, near river or riverine areas, any presence of in-ground pool water, or others, whereby they have to state the geographical conditions of the place, whether they notice the presence of any macaques during the mentioned activities, and subsequently indicate the species of macaques observed/noticed, either the long-tailed, pig-tailed, others, or unknown species. As a guide and to help the respondents recall the said activities, durations were set at 4 weeks prior to the data collection to minimize the recalled bias.
Last, on the environmental characteristics, variables asked were the geographical conditions of their home, which are either forest, forest edge, hilly, near river or riverine areas, any presence of in-ground pool water, or others whereby they have to state the geographical conditions of the place. Additionally, respondents must indicate their type of house as either traditional bamboo, traditional wooden, brick, wooden longhouse, or others where they have to state the type of house where they resided. The last question under the domain of environmental characteristics is whether they like to sleep or rest at the open compound of the house, and to indicate the exact time of the day—either morning, afternoon, early evening, or during the night.
All the items in the questionnaire have been reviewed for their content relevancies by experts in the field of public health, health promotion, health communication, and environmental health, as well as pretested during a session conducted among populations with the same criteria but not part of the sample, to ensure its language clarity, feasibility, readability, consistency of style, and formatting.
Specimen collection and management
The specimen collection was performed following the Management Guidelines of Malaria in Malaysia (Ministry of Health Malaysia, 2014). The patient’s finger is sterilized by alcohol and allowed to dry at room temperature. Then the fingertip is pricked with needle or lancet. The thick and thin films were prepared on one slide. A thick film is prepared by stirring drops of blood in a circular motion with the corner of the slide. For thin film, the smooth edge of the slide was placed, and the blood was spread by adjusting the angle between the slide and spreader to 45°. The surface was then smeared with a consistent sweep along the surface. The thin film is fixed with methanol after drying at room temperature. The slides were then read within 1 h after they reached the nearest hospital or health clinic by a laboratory technician.
For PCR, either whole blood in Ethylenediaminetetraacetic acid (EDTA) or dried blood spots on filter paper specimens were used for analysis. For whole blood via venipuncture, specimens in EDTA bottle were kept in a biohazard plastic bag and transported in a cold chain (4°C) within 3–4 h (−20°C if the transportation required longer period). Additionally, for dried blood spot prepared on filter papers (Whatman Grade 1), ∼125 µL of blood were blotted on the filter paper and leave to air dry. The specimen was then labeled with participant details, the date of sample collection, and the initials of the person responsible. The specimen were then transported to the laboratory at room temperature in a separate biohazard zip-lock plastic bag within 48 h. In Malaysia, PCR tests are carried out at some full specialist hospitals, research centers, and public health laboratories. For this study, samples were sent to the National Public Health Laboratory (MKAK) at Sungai Buloh, Selangor, for analysis.
Ethical Considerations
The study was approved by the National Medical Research Register, Malaysia (NMRR-19-962-47606). A general description, including an informed consent form, was included in the first part of the questionnaire with assurance that all the information would be kept confidential. All respondents signed the informed consent form themselves before embarking on the study. As stated above, due to the complexity of the informed consent process for respondents whose ages were below 18 years old, only individuals aged 18 years or more were included in the study.
Additionally, researchers verbally explained briefly to the respondents about the study and why they were chosen to be one of the respondents. They were also informed of their rights to withdraw at any time and how the information they give will be used. The respondents will then be given some time to read through the consent form themselves and ask for clarification (if there is any) before agreeing and signing the form. As for the researcher, we adhered to the principle of the Declaration of Helsinki and the Malaysian Good Clinical Practice Guidelines throughout the research.
Statistical Analyses
Data collected were entered and analyzed using IBM SPSS Statistics for Windows, Version 26.0. All continuous variables were described using mean with standard deviation and/or median with interquartile range, whereas categorical data as frequency and percentages. Univariate logistic regression was applied to evaluate the potential individual, host–vector interactions, and environmental risk factors for knowlesi malaria among respondents in this study. To maximize the potential of the variables listed, all were subjected to multiple logistic regression analyses regardless of the p values and their significant status to find their association with knowlesi malaria case status while adjusting for cofounders.
Results
Basic sociodemographic characteristics of the respondents
A total of 440 respondents participated in the study, with 88 cases and 352 locality-matched controls. There were equal distributions of gender among total respondents, 57.0% versus 43.0%; however, the proportion was noted to be higher for males among cases as compared to females (76.1% vs. 23.9%). For age, the mean age (38.8 ± 14.5) was noted to be lower among cases as compared to the control (40.6 ± 14.7). Additionally, more than 90.0% of the respondents were Malaysian, and more than half were of the Malay ethnicity group (56.8%). Apart from Malay, the second highest proportion of other ethnic groups was the Aborigines (“Orang Asli”) at 30.5%, followed by Indonesian at 5.7%. Chinese and Bangladeshi shared a proportion of 2.0% each, and the rest were less than 1.0% (Indian, Sabahan ethnicity of Dusun, Myanmar, Thailand, and Pakistan).
Focusing on the cases, the proportion was also noted to be highest among Malay at 55.7%, followed by the Aborigine at 28.4%, and Chinese at 4.5%. Furthermore, collectively, the minimum age of respondents was 18 years old, while the maximum age was 84 years old. This youngest age was reported among both cases and controls, while the oldest age of 84 was among the controls (Table 1).
Respondents’ Basic Sociodemographic Characteristics
Total N = 144 (Yes = 88, No = 352).
After the descriptive analysis of the respondents’ basic sociodemographic characteristics, the analysis was then continued to the univariate and multivariate logistic regression to evaluate the potential individual, host–vector, and environmental risk factors for knowlesi malaria among respondents in this study (Tables 2–4). All the variables were subjected to multivariate analysis, regardless of their significant status during the univariate analysis. The reason was that we wanted to maximize the potential of all the variables listed as the factors that affect their status. Additionally, all the variables tested in the analysis were identified as significant factors by previous studies. Thus, we wanted to prove the same hypothesis among our respondents.
Individual Risk Factors for Knowlesi Malaria Infections Among Respondents
Total N = 144 (Yes = 88, No = 352).
p < 0.05.
CI, confidence interval; LL, lower limit; UL, upper limit.
Host–Vector Interactions Factors for Knowlesi Malaria Infections Among Respondents
Total N = 144 (Yes = 88, No = 352).
p < 0.05.
Environment Risk Factors for Knowlesi Malaria Infections Among Respondents
Total N = 144 (Yes = 88, No = 352).
p < 0.05.
Individual risk factors for knowlesi malaria infections among respondents
Variables analyzed for individual risk factors (Table 2) include gender, age, smoking status, working status, number of households living together, and history of any chronic medical illness recorded. Regarding gender, both unadjusted and adjusted logistics regression analysis shows that the risk to become a case was significantly higher among males as compared to females (OR = 2.91 [95% confidence interval {CI} = 1.71, 4.96] and adjusted odds ratio [AOR] = 3.51 [95% CI = 1.81, 6.82], p < 0.001). However, for age, the analysis shows that with an increase of 1 year of age, the risk of becoming a case will lower by 0.01%. Even so, these results were found to be not significant even after controlling for the confounding effects of other variables (odds ratio [OR] p-value of 0.265, AOR p-value of 0.131).
Moving on to the next individual risk factor, results show that the risk to become a case was 1.39 times higher (95% CI = 0.86, 2.25) among current or ex-smokers as compared to a nonsmoker. However, when proceeding to multiple logistics regression analysis, the result becomes reversed, with the risk becoming 28.0% lower for current or ex-smokers as compared to a nonsmoker. Nevertheless, both levels of analysis were found to be not significant with p values of 0.178 and 0.261, respectively.
On the next individual risk factor, which is the working status, analysis shows that the risk to become a case was significantly 1.81 times higher (95% CI = 1.05, 3.13) among those who work as compared to those not working or housewives and students. However, when proceeding to control the other variables, results show that the risk was still higher with 1.13 times (95% CI = 0.59, 2.20) more among those who work, but the result becomes not significant with a p-value of 0.713.
Regarding the number of households living together, analysis shows that with the addition of one household member, there is an increase of 5.0% risk of becoming a case (OR = 1.05 [95% CI = 0.97, 1.15]). Moreover, after controlling for the confounding effect of other variables, the risk increased to 7.0% (AOR = 1.07 [95% CI = 0.98, 1.17]). Nevertheless, both levels of analysis were found to be not significant with p values of 0.245 and 0.153.
The final individual factor included in this study was any history of medical illness recorded among respondents. It was found that those with a history of medical illness have a 1.33 times higher risk (OR = 1.33 [95% CI = 0.71, 2.52]) to become a case as compared to those without any reported chronic medical illness. The same was reported for the multiple logistics’ regression analysis of the variable, whereby the risk was found to be almost two times higher (AOR = 1.95 [95% CI = 0.95, 3.99]) among those with a history of chronic medical illness, as compared to those without the history. Unfortunately, just like the other individual risk factors listed in this study, it was found to be not statistically significant as the risk factors for knowlesi malaria infections (p values of 0.374 and 0.067).
Host–vector interactions risk factors for knowlesi malaria infections among respondents
Moving on to the host–vector interaction factors as a risk for knowlesi malaria infections among respondents, variables listed were geographical condition of the place of work or study, reported noticing the presence of macaques near the house, place of work/or place of study during the past 4 weeks, and last the type of macaque species observed (Table 3).
For the geographical condition of the place of work or study, analysis shows that for respondents whose place of work or study was near the forest edge, their risk to become a case was 35.0% lower as compared to those whose place of work or study was not at the forest edge (OR = 0.65, 95% CI = 0.41, 1.04). During the simple logistics regression analysis, the result was not statistically significant with p-value of 0.070; however, during multiple logistic regression analysis, the result still shows the same lower risk trend at 44.0% (AOR = 0.56, 95% CI = 0.34, 0.95), but it has become statistically significant with p-value of 0.030. Other than forest edge, all other types of geographical conditions of the place of work or study, namely forest, an area with ground pool water, hilly areas, rivers, and bushes, did not statistically increase or lower the risk for respondents to become a case.
The second last host–vector interactions factor included in this study was noticing the presence of macaques near the house, place of work, or place of study during the past 4 weeks. Results of the analysis performed show that the risk was 1.26 higher (OR = 1.26, 95% CI = 0.76, 2.08) among those who reported noticing the presence of macaques near their house, place of work, or place of study during the past 4 weeks as compared to those who did not report such presence. When controlling for the confounding effect of other variables, the same higher risk trend was noted with those who reported noticing the presence of macaques to have 1.18 times higher risk (AOR = 1.18, 95% CI = 0.69, 2.02). Unfortunately, both levels of analyses were found to be not statistically significant with p values of 0.368 and 0.540, respectively.
Moving on to the last host–vector interactions factor, which is regarding the species of macaque observed, the results of the analysis show that the risk of becoming a case was higher if they reported observing the long-tailed macaques (OR = 1.42, 95% CI = 0.88, 2.30), pig-tailed macaques (OR = 1.71, 95% CI = 0.76, 3.86), or even if they were unsure of the species (OR = 1.24, 95% CI = 0.51, 2.98), as compared to if no such observations were reported. However, for observing other species of macaques, the risk was found to be lower (OR = 0.87, 95% CI = 0.53, 1.43). Even after controlling for confounders, the same trend was observed with calculated odd ratios of between 0.78 and 1.72 for all types of observations. Nonetheless, despite all the observations reported, none of the mentioned risk factors was found to be statistically significant factors that increase the risk of respondents becoming a case.
Environment risk factors for knowlesi malaria infections among respondents
The analysis then moved to the last factor, which is the environmental risk factors (Table 4) for knowlesi malaria infection among respondents. Variables listed were the type of housing area, type of house, geographical condition of the housing area, and any habit of resting or sleeping outside of the house or in an open area during the night.
Focusing on the type of housing area, the result shows that the risk to become a case was 64.0% (OR = 0.36, 95% CI = 0.18, 0.76) significantly lower (p = 0.0.07) among those living at the Orang Asli village as compared to those living at an organized village. And when controlling the confounding effect of other variables, the same trend was noted, whereby the risk was notably 56.0% lower (AOR = 0.44, 95% CI = 0.20, 0.94) as compared to the organized village, with a p-value of 0.035. For other types of housing areas, namely traditional villages and government scheme housing areas such as Federal Land Development Authority (FELDA) and Federal Land Consolidation and Rehabilitation Authority (FELCRA), respondents who stayed at both of these housing areas do not have a significant risk to become a case as compared to those who stayed at the organized villages, even after controlling for the confounding effect of other variables (p values 0.051 and 0.092, respectively).
For the type of house, the analysis shows that those respondents who stayed in a brick house have a significant 94.6% lower risk to become a case as compared to other types of houses (OR = 0.054, 95% CI = 0.01, 0.50; p = 0.010). Even after adjusting for confounding effects, the risk remains significantly 91.0% lower (AOR = 0.09, 95% CI = 0.01, 0.76). The same trend was seen for respondents who stayed at a wooden workers’ longhouse. Their risk to become a case was noted to be significantly 94.0% lower (OR = 0.06, 95% CI = 0.01, 0.57) as compared to other types of houses. And when controlling for other variables, the result was still statistically significant with a p-value of 0.018.
Focusing on a traditional wooden type of house, the risk too was found to be significant at 93.0% lower (OR = 0.07, 95% CI = 0.01, 0.69; p = 0.022) as compared to other types of houses. However, when controlling for the confounding effect of other variables, the result becomes not statistically significant, albeit showing the same lower risk (AOR = 0.11, 95% CI = 0.01, 1.01; p = 0.051). When analyzing the risk of respondents staying in a traditional bamboo house to become a case, as compared to those who stayed in other types of houses, the results were found to be significant during a simple logistics regression analysis with 92.0% lower risk (OR = 0.08, 95% CI = 0.01, 0.88; p = 0.010). However, during multiple logistic regression analysis, the result was found to be not statistically significant (AOR = 0.13, 95% CI = 0.01, 1.39).
Moving to the next environmental factor, which is the geographical condition of the housing area, analysis shows that houses situated in hilly areas were a significant protective factor for the occupant from becoming a knowlesi malaria case. The risk was found to be 39.0% lower (OR = 0.61, 95% CI = 0.38, 0.98; p = 0.041) as compared to those houses that were not situated in a hilly area. When proceeding to the multiple logistics regression analysis, the result remains significant at 48.0% lower (AOR = 0.52, 95% CI = 0.31, 0.87; p = 0.012). The same trend was observed for houses situated at the forest edge. The result echoed the result on the geographical condition of the place of work or study, whereby the risk was found to be 47.0% lower (OR = 0.53, 95% CI = 0.32, 0.89; p = 0.016) as compared to those houses that were not situated at the forest edge. Other than the forest edge and hilly areas, all other geographical conditions of the housing areas listed, namely forest, ground pool water, river, and bushes, were all found to be not statistically significant to increase or lower the risk for respondents to become a case.
Regarding the last environmental risk factor on the habit of resting or sleeping outside of the house or in an open area during the night among respondents, results of the analysis show that those who have these habits were 1.67 times more likely (95% CI = 1.04, 2.69; p = 0.033) to be infected and become knowlesi malaria patients as compared to those who do not have these habits. However, when proceeding with the multiple logistic regression analysis, results were found to be not statistically significant, although the risk was still high among those with the habits (AOR = 1.36, 95% CI = 0.82, 2.24; p = 0.231).
Discussions
This study was conducted to identify the individual, host–vector interactions, and environmental risk factors for P. knowlesi malaria among at-risk communities in Peninsular Malaysia.
The analysis of this study highlighted seven significant findings. The first one is that being male is 3.51 higher risk (p < 0.001) to become a case as compared to females. The second is respondents whose place of work or study was near the forest edge have 44.0% lower risk as compared to those whose place of work or study was not at the forest edge (p = 0.030). The third is regarding housing area, whereby the risk to become a case was notably 56.0% lower among those living in the Orang Asli village as compared to the organized village, with a p-value of 0.035, while the fourth and fifth were on type of houses, whereby respondents who stayed in a brick house had a significant 91.0% (p = 0.027) and stayed at a wooden workers’ longhouse had a 94.0% (p = 0.018) lower risk to become a case as compared to other types of houses. The two last significant findings were on the geographical condition of the housing area, whereby analysis shows that houses situated in hilly areas and forest edges were a significant protective factor for the occupant from becoming a knowlesi malaria case, with 48.0% and 47.0% lower risk, respectively, as compared to those houses that were not situated in both areas.
Discussing each of the points, in general, the majority of the previously published studies were in line with the findings of the current study regarding gender roles in the risk of contracting knowlesi malaria (William et al., 2013; Cooper et al., 2020; Naserrudin et al., 2022). The male gender has always been reported as at higher risk to get this disease as compared to females, and these findings were shared globally and across countries and states. The seemingly gender-biased theory was proposed based on the socioeconomic structure of the community, particularly in a country like Malaysia, whereby most of the outdoor type of jobs were dominated by males, which coincided with the natural biting condition of the disease’s vector (William et al., 2013; Cooper et al., 2020). Additionally, other socially related practices of some of the community, for example, the preferences to sleep or rest in outdoor open areas and do other social activities, were also particularly favored by the male gender. Such practices increased the potential transmission of the disease through biting by the mosquito, as well as possible interactions with the reservoir, the macaques (Monroe et al., 2015; Quaresima et al., 2021; Okiring et al., 2022). Apart from that, the United Nations Development Program, UNDP (2015), in their discussion paper on Gender and Malaria, listed, among others, a few other possible explanations for the gender-biased condition related to malaria. These include access to malaria-related information, prevention, and treatment, as well as dress and cultural norms. Nevertheless, a study conducted in the northern part of Sabah, Malaysia, and Palawan, the Philippines, contradicts most of the evidence whereby their results show serological testing evinced that gender was not related to P. knowlesi infection, and both genders had equal exposure to P. knowlesi based on their antibody response to P. knowlesi antigens, albeit a higher proportion of women were detected with asymptomatic infections (Fornace et al., 2018).
Bringing into the line of the next points, which fall under the domain of host–vector interactions, having a place of work or study near a forest edge will significantly lower the risk of becoming a knowlesi malaria case. This is a finding that contradicted the widely accepted and proven hypotheses on the transmission of malaria to humans about the interactions between the two species. Areas near the forest edge that usually have low-level vegetation such as bushes were identified by much previous literature as critical resting spots and shaded refuges between vectors’ larval habitats and humans’ places of activity. Thus, there was a positive correlation between the work and study activities at the forest edge and malaria prevalence (Durnez et al., 2013; De Oliveira et al., 2013; Grigg et al., 2014; Hawkes et al., 2019; MacDonald and Mordecai, 2019). However, despite this plausible explanation, there was also a growing body of evidence that directed the hypothesis in the other direction, as shown in this current study. According to studies conducted in the Amazon Forest (Tucker et al., 2017; Chaves et al., 2021), even though the interactions were initially high between the host and vectors in this area, the ongoing work or study activities at the forest edge may inevitably cause more deforested landscapes where there will be more forest cover removed. As a result, this forest clearing will expose the vector’s larval habitats to sunlight, subsequently reducing larval populations in the areas. Therefore, the adult vectors will also be reduced, which lowers the risk of the transmission of the disease to humans.
The last four significant risk factors were under the environmental risk, whereby living in the Orang Asli village and having either a brick house or wooden workers’ longhouse in the hilly areas will significantly lower the risk of becoming knowlesi malaria case. Based on the previous literature (Jiram et al., 2016; Macherera et al., 2017; Meireles et al., 2020; Munajat et al., 2021; Wetzler et al., 2022), aboriginal people are among one of the at-risk populations for the infections of malaria. There are many socio-behavioral factors of these populations, such as the location of their village, which is often near the forest area, and the way they use the forest as their main source of income, which has made it favorable for them to be infected with malaria, including knowlesi malaria. Nevertheless, a study conducted by Taek (2019) on the traditional practice of the aboriginal people in West Timor, Indonesia, has shown that these indigenous ethnic groups have been practicing a traditional way to prevent them from becoming malaria cases. The practices include both herbal (drinking herbal concoctions, inhaling the vapor of boiled medicinal plants, massage with a paste of medicinal plants, etc.) and nonherbal techniques such as repelling mosquitoes using the smoke of burned aromatic plants.
On the second finding regarding staying at either brick or wooden workers’ longhouse will significantly lower the risk to become knowlesi malaria cases, there were several explanations and evidence that supported the finding from the current study. First, it is related to the structure of a household building with the risk for malaria infection. Findings from a few studies (Wanzirah et al., 2015; Ippolito et al., 2017; Tusting et al., 2017) conducted to link the structure of houses with malaria risk have shown that houses constructed of brick, wood, or cement blocks, which are usually also accompanied by metal roofs, have fewer gaps and without eaves in between. Such builds have led to reduced potential for mosquito entry and subsequently lesser risk of being bitten by infected vectors as compared to houses made of traditional materials such as bamboo, clay, or various debris. The next is regarding the preventive behaviors adopted by workers and their managers through collaborations with the district health office. Few programs were conducted to reduce the risk of knowlesi malaria among this high-risk population, including insecticide-treated bed nets and indoor residual spraying (Aung et al., 2022; Phok et al., 2022).
The last significant finding that lowers the risk of getting knowlesi malaria was regarding the geographical condition of the housing area that was situated in the hilly areas. Hilly areas are known for their higher altitude and lower temperature. These two criteria are among the conditions that are less favorable for both the larval and adult stages of the vectors. These were also supported by previous studies (Bødker et al., 2003; Siya et al., 2020) that show a varied effect of higher altitudes and low temperatures on mosquitoes, such as halting the parasite development in the vectors, lowering the transmission due to the low vector densities, and reducing the proportion of infective mosquitoes. Nevertheless, while this finding supports and gives hope in the effort to reduce the risk of malaria, caution should always be exercised given the trend in climate change, particularly the increase in temperature, which creates ambient conditions at or within the higher altitude, thus creating new potential environments for the vectors.
Conclusion
It is notable to mention a few of the limitations met by this current study. First, as the respondents included in this study were only those from the three preidentified areas, those cases outside of the three areas will not be counted. Second, as stated in the methodology section, due to the complexity of the informed consent process, we only include cases aged 18 years old and above. Thus, there is a possibility that we missed this population. The next limitation was that the questions required respondents to recall their experiences during the past 14 days. These will raise the possibility of recall bias on the information provided. And last, since the tools for data collection are questionnaires, information bias would be the issue that warrants a cautious interpretation of the results.
In conclusion, to prevent and control knowlesi malaria within the epidemiological triad of agent, host, and environment, it is crucial to interrupt their interactions and recognize each factor’s distinct role. For the at-risk communities in Peninsular Malaysia, gender emerges as an independent individual risk factor, with males exhibiting a probability of being affected more than three times higher than females. Conversely, residing near a forest edge, living in an Orang Asli village, or occupying a brick or wooden workers’ longhouse situated in hilly areas reduces the interactions between hosts and vectors, thereby significantly lowering the environmental risk associated with contracting knowlesi malaria within this population by a considerable range of 39.0–94.0%.
These findings attest that the prevention and control programs should be tailored to specific populations, avoiding a one-size-fits-all approach. Furthermore, wider-reaching research that encompasses broader geographical areas, more at-risk populations, and integrating behavioral components should be conducted for a more in-depth look into these highly potential areas for improvement.
Footnotes
Acknowledgment
The authors declare that this article is original, and apart from the preprint unreviewed version in the Europe PMC (![]() ) and Research Square (https://doi.org/10.21203/rs.3.rs-3710689/v1) sites, it has not been published before and is currently not under consideration for publication elsewhere. The authors would like to express our appreciation to the Ministry of Higher Education Malaysia and the Ministry of Health Malaysia for their support in this study. The team thanked the district health offices, particularly the assistant environmental health officers of Gua Musang, Kelantan; Kuala Lipis, Pahang; and Kota Tinggi, Johor, for their assistance in this research. Last, this article is dedicated to the late Dr. Rosemaliza Mohd Kamalludeen for her invaluable contribution as a research member before she passed away.
) and Research Square (https://doi.org/10.21203/rs.3.rs-3710689/v1) sites, it has not been published before and is currently not under consideration for publication elsewhere. The authors would like to express our appreciation to the Ministry of Higher Education Malaysia and the Ministry of Health Malaysia for their support in this study. The team thanked the district health offices, particularly the assistant environmental health officers of Gua Musang, Kelantan; Kuala Lipis, Pahang; and Kota Tinggi, Johor, for their assistance in this research. Last, this article is dedicated to the late Dr. Rosemaliza Mohd Kamalludeen for her invaluable contribution as a research member before she passed away.
Authors’ Contributions
E.M. is the principal investigator of this study. H.P., E.M., A.A.A., M.R.H., M.R.S., A.I., S.G., and H.D. were involved in the conceptualization of this study. H.P., E.M., A.A.A., M.R.H., M.R.S., A.I., S.G., and H.D. were involved in instrument development. S.G. and H.D. helped in the data collection. H.P. and M.R.H. contributed to the data analysis. H.P., A.A.A., S.G., and H.D. drafted the article. E.M., M.R.H., and M.R.S. reviewed and edited the article. All authors read and approved the final article.
Availability of Data and Materials
The final datasets are available on reasonable request to the corresponding author.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This research was funded by a grant from the