
Abstract
Background:
The largest documented outbreak of hemorrhagic fever with renal syndrome occurred in Primorje-Gorski Kotar County, Croatia, in 2021, marking the first-time cases of hantavirus infection recorded outside of the known endemic region in the north of the county.
Aim:
To identify the factors contributing to the spread of the outbreak and to compare risk factors for acquiring hantavirus infection in the endemic and newly affected regions.
Methods and Results:
A total of 189 cases were confirmed by positive Puumala IgM/IgG antibodies (93.6%), and 13 probable cases were identified by clinical and epidemiological data (6.4%) using a structured questionnaire. Of the 179 cases with available clinical data, 59 (33.0%) were hospitalized. Three cases received hemodialysis, and no deaths were reported. Among 170 cases with information on exposures, 66 (38.8%) reported occupational risk. Cases in the northern part of county were more likely to have been infected in early spring (OR 27.1, 95% CI 2.93–250.7), to report seeing a rodent (OR 6.5; 95%CI 2.3–18.4), and to know someone with hemorrhagic fever with renal syndrome (HFRS) (OR 3.0; 95%CI 1.2–8.0) than cases from the southern part of the county. Data from Croatian Forests Ltd. suggested that an unusually good production of beech seeds in 2020 may have contributed to an increased rodent population in 2021. However, average temperature, rainfall, and humidity data from 2021 did not illustrate a significant difference from previous years (Kruskal–Wallis p = 0.837, p = 0.999, p = 0.108).
Conclusion:
The 2021 HFRS outbreak was likely fueled by an abundant rodent population and virus transmission in rodent hosts. Human activity, environmental factors, and the ensuing animal–human interactions have spread hantavirus infection from Croatia’s mountainous region to a previously nonendemic coastal area with a Mediterranean climate.
Introduction
Hemorrhagic fever with renal syndrome (HFRS) is a zoonotic disease caused by several hantaviruses of the Orthohantavirus genus, Hantaviridae family (European Center for Disease Prevention and Control, n.d). Hantaviruses are usually adapted to a specific rodent or related rodent species as their host. The Orthohantavirus puumalaense (PUUV), which is carried by the bank vole (Myodes glareolus), is responsible for the majority of HFRS cases in Europe and causes a relatively mild form of the human disease. The Orthohantavirus dobravaense (DOBV), which is infrequently recorded and carried by the yellow-necked mouse (Apodemus flavicollis), is responsible for a more severe infection in humans (ECDC, n.d; Filippone et al, 2019). In Croatia, in addition to PUUV and DOBV detected in humans and rodents, Orthohantavirus dobravaense (Saaremaa virus) has been identified in striped field mice (Apodemus agrarius), Orthohantavirus tulaense in common and field voles (Microtus arvalis, Microtus agrestis), and Orthohantavirus seewisense in shrews (Sorex araneus) (Bjedov et al, 2016; Kuhn and Schmaljohn, 2023; Ledina et al, 2002; Scharninghausen et al, 2002; Vilibic-Cavlek et al, 2017).
Hantaviruses are horizontally transmitted among rodents through infected excreta (saliva, urine, and feces) by indirect contact or directly through hostile rodent behavior (Hinson et al, 2004; Kariwa et al, 1998; Voutilainen et al, 2015). Rodents are most infectious one to two months after infection (Bernshtein et al, 1999; ECDC, n.d.; Voutilainen et al, 2015). Infection in rodents does not typically produce overt disease and can persist throughout their lifespan (Bernshtein et al, 1999).
The main route of infection in humans is the inhalation of aerosol and dust contaminated by rodent excreta. Other, less frequent routes of transmission are direct contact with infected material or consumption of infected water or food (ECDC, n.d.; Heymann, 2022; Witkowski et al, 2017). Humans are considered to be the end hosts (Heymann, 2022). In humans, HFRS usually presents in five stages as follows: febrile, hypotensive shock, oliguric, polyuric, and convalescent (Avšič-Županc et al, 2019). There have been no reports of clinical hantavirus reinfection (Van Epps et al, 2002).
In Europe, most hantavirus infections are recorded in Scandinavian, Central European, and Balkan countries. The highest reported incidence is in Finland (1164 cases in 2020; 21.1/100,000) (ECDC, 2015, 2023). The first cases of HFRS in Croatia were recorded in 1952, and the first outbreak occurred in 1967 among forestry workers in Plitvice Lakes (Radosevic and Mohacek, 1954; Vesenjak-Hirjan et al, 1971). Subsequent smaller outbreaks were linked to military activities; 1989 in Velika Gorica, 1991 in the Novska area, and 1995 in Dinara Mountain, Mala Kapela, and Slavonia (Ledina et al, 2002; Mulić and Ropac, 2002; Tadin and Cvetko Krajinović, 2009). Croatia experienced its largest outbreak in 2002, with 401 cases, (9.0/100,000) (Kuzman et al, 2003). Since then, outbreaks have become more frequent, with the last outbreak occurring in 2021 (334 cases; 8.6/100,000) (CIPH, 2022). Hantavirus infections are now being reported throughout the whole territory of Croatia, with the exception of coastal counties (CIPH, 2022).
In Primorje-Gorski Kotar County (PGKC), the first recorded HFRS cases date from 1987. Several smaller outbreaks occurred in subsequent years as follows: in 2002 (47 cases, 15.8/100,000), in 2012 (28 cases, 9.4/100,000), and in 2014 (51 cases, 17.4/100,000) (Teaching Institute of Public Health Primorje-Gorski Kotar County, 1987–2021). HFRS outbreaks are usually associated with exposure in Gorski Kotar (Borčić et al, 1991; Kuzman et al, 2003; TIPH PGKC, 1987–2021). Gorski Kotar is a 1273-km2 forested mountainous region that accounts for 35% of the county’s territory (Institution for Physical Planning of Primorje-Gorski Kotar County, 2014) that is popular for hunting, hiking, and other outdoor leisure activities. In 2021, the largest outbreak of HFRS to date occurred in PGKC, with 202 cases (76.1/100,000) (CIPH, 2022; Fig. 1). For the first time, cases of hantavirus infection were recorded in the southern part of the county, beyond the previously documented endemic region. As the size and extent of this outbreak were unexpected, we investigated to describe the outbreak, identify factors contributing to its spread and geographic distribution, and to compare risk factors for acquiring hantavirus infection in endemic and new regions.
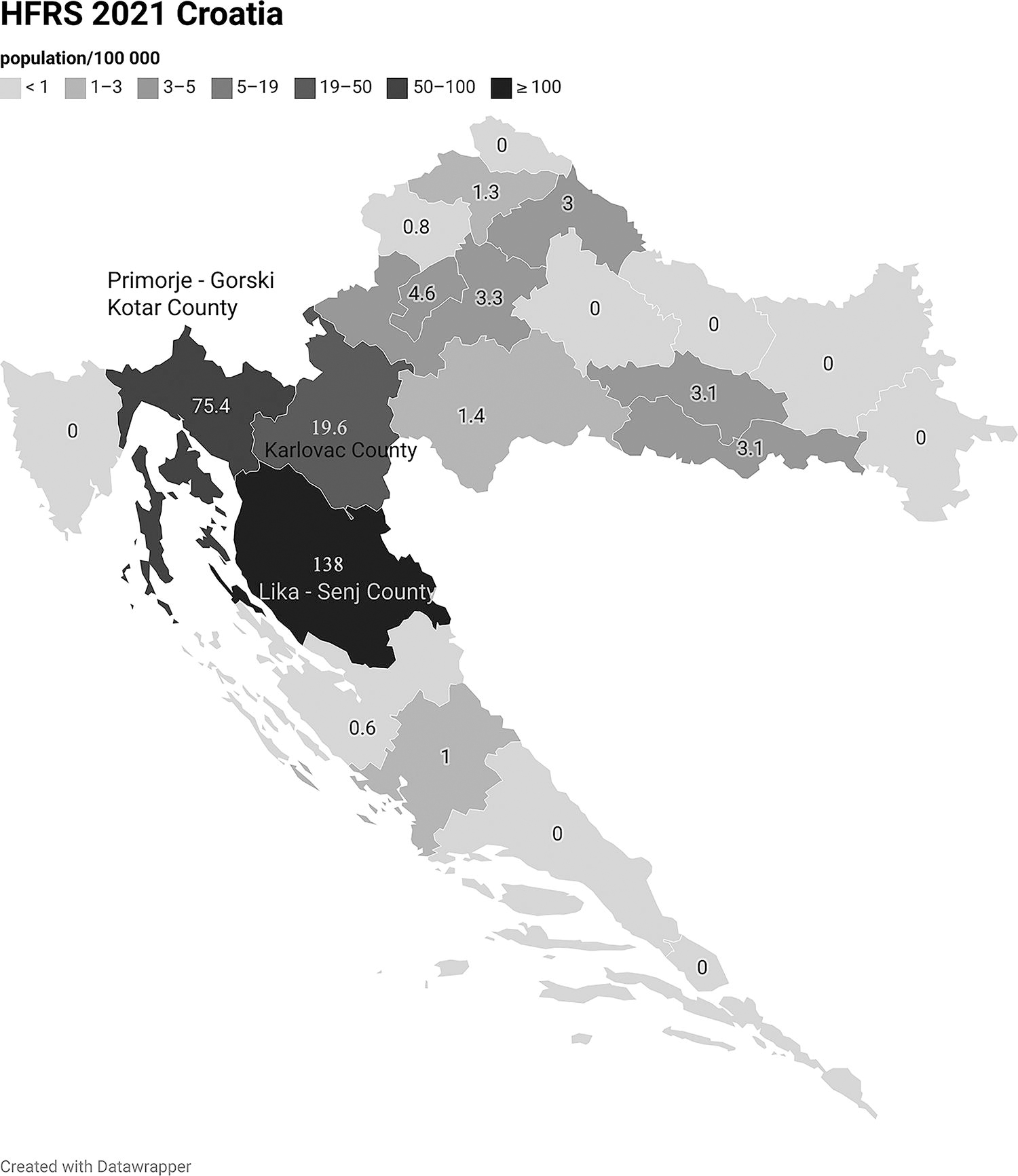
Incidence rate of hemorrhagic fever with renal syndrome (HFRS) in 2021, Croatia.
Materials and Methods
Outbreak region and case classification
PGKC had a population of 265,419 in 2021 (Croatian Bureau of Statistics, 2022). Rijeka is the largest city, located on the coast with a Mediterranean climate. In the north is the region of Gorski Kotar with a mountain climate (Croatian Meteorological and Hydrological Service, 2023; Primorje-Gorski Kotar County, 2020a). Gorski Kotar’s highest mountain peaks are over 1400 m, with an average altitude of 700–800 m. Winter temperatures drop below zero degrees Celsius, with snow cover and a precipitation of 100–150 mm per month (Meteoblue, 2023a; PGKC, 2020a). According to the Köppen climate classification, the area of Gorski Kotar has a warm humid climate with hot summers and mild winters, combined with areas with a humid subarctic boreal climate (Filipčić, 1998). It borders Slovenia in the north and Karlovac County in the east. Between coast and Gorski Kotar, the climate transitions from this cooler humid climate zone to a transitional, mixed mountainous Mediterranean area in the southern part of the county (PGKC, 2020b). We classified cases into five groups, reflecting geographical/climate zones, based on the presumed location of exposure/infection. Group 1 participants were exposed in Gorski Kotar and neighboring territory (northern area), Group 2 in the southern area of the county, and Group 3 in Rijeka and the islands. Cases who reported exposure outside PGKC were assigned to Group 4, and cases without data on exposure were assigned to Group 5.
Case finding
HFRS has been a reportable disease in Croatia since 1986 (ECDC, 2014). HFRS cases are typically reported by hospital clinicians, and a smaller number are identified by primary health care physicians and reported to the regional epidemiological service of the Teaching Institute of Public Health in PGKC (TIPH PGKC). In 2023, we extracted case data from January to December 2021 from the regional surveillance system, applying the national case definition (CIPH, 2012). Confirmed cases had clinically compatible symptoms (fever, renal insufficiency, oliguria, and/or hemorrhages) and met laboratory criteria (hantavirus-specific antibody response: IgM and IgG). Probable cases had clinically compatible symptoms with at least one of the following epidemiological links: transmission from animals to humans through contact with infected rodents and their excreta in nature (inhalation of dust during cleaning, tidying of premises and gardens) or exposure to ingestion of contaminated food or drinking water.
Structured questionnaire
In 2021, epidemiologists conducted interviews with cases to gather information on their activities related to hantavirus infection and clinical symptoms. For this study, the same cases were interviewed in 2023 using a new structured questionnaire for additional information about probable exposure and outcomes. Investigators also referred to available medical information to validate case reports. Furthermore, information regarding the proximity of a person’s residence to forested regions was also acquired. Cases were queried about any direct or indirect contact with rodents, as well as use of personal protective equipment and preventive measures against acquiring HFRS. Cases were asked about their occupational and recreational activities in the five weeks prior to symptom onset, and epidemiologists assigned estimated GPS coordinates based on reported activities known to be associated with hantavirus infection. In 2021 and 2023, out of the 22 cases not available for an interview, three were unwilling to participate, and 19 were without a valid contact number or did not respond to the invitation letter.
Laboratory investigation
In the 2021 outbreak, serum samples were collected and tested for the presence of hantavirus antibodies using immunochromatographic rapid tests for PUUV and DOBV/HTNV (ReaScan® Puumala IgM/Dobrava-Hantaan IgM, Reagena, Toivala, Finland) or indirect immunofluorescence assay (Hantavirus mosaic; Euroimmun, Lübeck, Germany) for detection of IgM and IgG antibodies for the orthohantaviruses as follows: PUUV, DOBV, HTNV, SEOV, SAAV, and Sin Nombre.
Environmental data
Data on the production of European beech seed (Fagus sylvatica L.) in the Gorski Kotar region were gathered from Croatian Forests Ltd., Forest Administration Delnice, which is a public company responsible for managing forest areas in the Republic of Croatia. Five qualitative categories were used to classify the seed yield from 2017 to 2021 as follows: no recorded seeds, “poor” production (minimal quantities of seeds are recorded in some trees), “low” production (fewer trees are producing seeds, sometimes only found in a certain area), “good” production (trees are bearing seed in a moderate amount, almost through the whole territory), “very good” production (all trees have high seed production), and “excellent” production (mast year, all trees are bearing a large number of seeds).
Meteorological data
Meteorological data for individual years from 2017 to 2020, and for the overall period 1991–2020, including temperature (degrees Celsius), relative humidity (%), precipitation (millimeters), and snow cover (centimeters), were obtained from the Croatian Meteorological and Hydrological Service for Delnice, the city in the middle of Gorski Kotar.
Statistical methods
We described variables of person, place, and time in absolute numbers and proportions. To establish differences between two categorical variables, the chi-squared or Fisher exact test was used. For a small group (n < 30) or for data that were not normally distributed the Wilcoxon rank-sum test was applied to establish differences between two groups or the Kruskal–Wallis test to establish differences between more than two groups. The threshold for statistical significance was set at p < 0.05. Logistic regression analysis was used to explore exposure factors associated with HFRS in Gorski Kotar compared with cases in southern county, using a forward stepwise method. IBM SPSS Statistics Version 23 and StataCorp LCC Stata/IC 14.2 analytical software were used for data analysis.
Results
Cases in this outbreak most frequently experienced high fever (177/180; 98.3%), myalgia (131/180; 72.8%), and back pain (107/179; 59.8%). The other symptoms reported were headache (140/180; 77.8%), oliguria (57/180; 31.7%), visual disturbances (37/178; 20.8%), abdominal pain (30/180; 16.7%), cough (10/179; 5.6%), breathing difficulties (9/180; 5.0%), and purpura (6/179; 3.4%). One-third of the patients were admitted to hospital (59/179, 33.0%); the rest were treated as outpatients or in the community. Out of 179 patients, 53 had comorbidities (29.6%). Median length of hospital stay was 7 days (range 1–30 days). Three participants received hemodialysis (1.7%), and no deaths were reported. There were 189 confirmed cases (n = 202; 93.6%) infected by the Puumala virus and 13 probable cases (6.4%).
Group 1 (Gorski Kotar and neighboring territory, northern area) included 142 (70.3%) cases; Group 2 (southern part of the county) included 28 (13.8%) cases; and Group 3 (Rijeka and islands) accounted for only 3 (1.5%) cases (Figs. 2 and 3). Three cases (1.5%) in Group 4 were presumably exposed outside the county, and Group 5 included 26 (12.9%) participants with no data available.
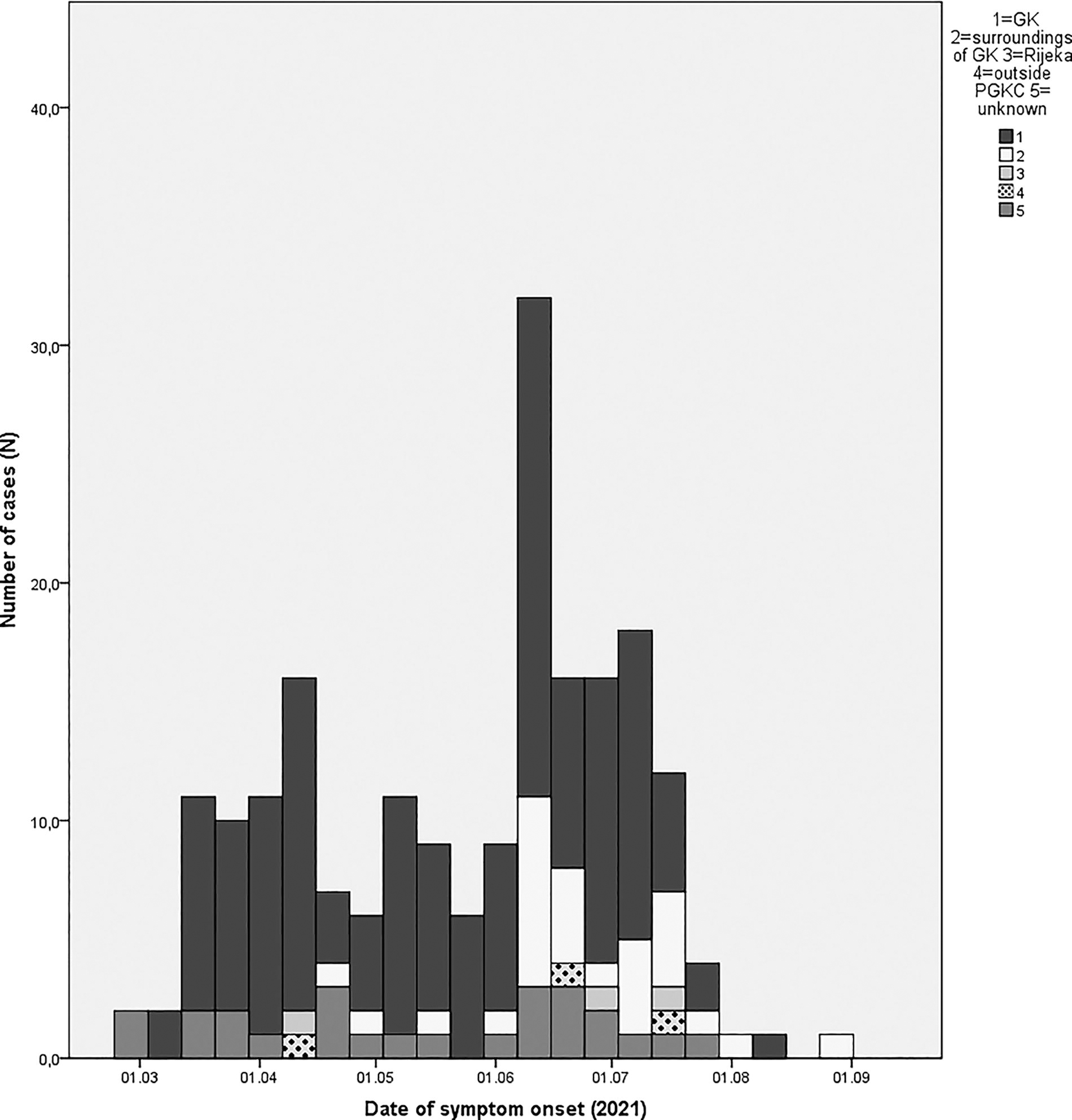
Cases of hemorrhagic fever with renal syndrome by date of symptom onset and probable location (Group 1–5) of exposure (n = 201), Primorje–Gorski Kotar county, 2021.

Geographic distribution of cases based on probable exposure location (169 cases; 197 locations) in Primorje-Gorski Kotar County.
The first reported case in 2021 had disease onset on February 28th, with the last case onset on August 25th. The greatest number of cases became ill in June (70/201; 34.8%) (Fig. 2).
Of the total 174 cases with geolocation data, 142 (81.6%) were most probably infected at one site; for 26 cases (14.9%), two positions were assigned, and for one case, three positions were used (0.6%) (Fig. 3). Two cases had numerous possible exposures; therefore, they were not presented on the map (1.2%), and three cases were most probably infected outside the county (1.7%) (not presented).
When comparing probable exposure, cases in Group 1 were more likely to be infected in the early spring compared with cases in Group 2 (34.8% vs. 3.7%, p < 0.05). Cases in Group 1 carried wood more frequently (70.1% vs. 46.4%, p < 0.05) and were more often engaged in occupational activities, which exposed them to rodent environments (44.0% vs. 14.8%, p < 0.05) than those in Group 2. Those in Group 1 were more likely to have observed rodents (87.6% vs. 53.6%, p < 0.05) and were more conscious of HFRS (89.0% vs. 57.7%, p < 0.05). In comparison to Group 2, cases who were assigned to Group 1 were more likely to report knowing other individuals with HFRS (66.0% vs. 35.7%, p < 0.05) (Table 1).
Sociodemographic and Exposure Characteristics of Groups 1, 2 and all HFRS Cases
Regarding occupational exposure in both groups, (66/170), 22.7% (15/66) of cases worked in sawmills, 21.2% (14/66) were employed as woodcutters, 18.2% (12/66) were forestry workers, and 37.9% had other occupations (25/66) (mountain rescuers, game warden, field police officer, etc.). In this study, 72.3% (73/101) of nonoccupationally exposed participants likely became infected near or at their residence, compared with 57.6% (38/66) of occupationally exposed participants (p = 0.049).
Cases in Group 1 [Gorski Kotar and neighboring territory (northern area)] were more likely to have become ill in early spring (OR 27.1, 95%CI 2.93–250.7), to report seeing a rodent (OR 6.5; 95%CI 2.3–18.4), and to know someone with HFRS (OR 3.0; 95%CI 1.2–8.0) compared with cases infected in the southern part of the county (Table 2).
Factors Associated with Infection Among Group 1 Cases [Northern Area (Gorski Kotar and Neighboring Territory)] Compared
CI, Confidence interval; OR, Odds ratio.
The year 2018 had “very good” production of beech seed (Fagus sylvatica L.), and “good” production was recorded in 2020. There were no seeds recorded in the years 2017, 2019, and 2021, and there was no mast year recorded from 2017 to 2021.
There was no statistical difference in the annual average amount of rainfall, temperature, or humidity in 2021 and the period preceding the outbreak (1991–2020) (p = 0.837, p = 0.999, p = 0.108). No statistically significant difference was observed in the average annual amount of rainfall, value of temperature, or humidity between the individual years from 2017 to 2021 (p = 0.755, p = 0.932, p = 0.161). In the winter before the 2021 outbreak, 7 days were listed with more than 30 cm of snow, but the average winter temperature in 2020/2021 (1.9°C) was similar to the average winter value from 1991 to 2020 (1.8°C) (Table 3).
Climate Characteristics of Delnice, Gorski Kotar from 1991 to 2021 Period
Differences between 1991–2020 and 2021 were tested.
Differences between 2017 and 2021 were tested.
Missing data from July to October.
Discussion
According to ECDC report, hantaviruses have expanded throughout Europe, reaching new territories and becoming more prevalent in endemic areas (ECDC, n.d.). In 2021, a large number of cases were documented both within and outside this recognized endemic area of Gorski Kotar in PGKC (Borčić et al, 1991; Kuzman et al, 2003, TIPH PGKC, 1987–2021). The majority of cases were reported in the northern area (Gorski Kotar and neighboring territories), but the first known cases were reported from the southern and coastal part of the county. The 2021 outbreak appeared to start in the Gorski Kotar region, where the highest risk for acquiring infection was in early spring compared with the southern part of the county (Table 2). This outbreak illustrates that hantavirus infections have spread from the mountainous northern climate zone to the coastal Mediterranean climate. Based on the geolocation data of probable exposure and the distribution of cases, as well as exposure information, we hypothesize that this outbreak was driven by significant virus transmission among rodents. The 2021 outbreak also expanded to nearby counties, including Lika-Senj County (138/100 000) and Karlovac County (19.6/100,000) (Fig. 1), as well as the nearest countries to the east, such as Bosnia and Herzegovina, which saw an upward trend in the number of cases compared with previous years (Salimović-Bešić et al, 2023). The outbreak also spread to the west, with Slovenia reporting the highest rate to date (566 cases; 27.2/100,000) (Veterinary faculty, University of Ljubljana, 2021).
Interactions between humans and rodents, whether direct or indirect, play an important role in the HFRS outbreak. Human population distribution, leisure and occupational activities, and urbanization could determine the extent of an outbreak. Since the last population census in 2011, the Gorski Kotar area and neighboring municipalities have experienced a population decline. This trend particularly impacted the Gorski Kotar region, where the population decreased from 23,011 to 18,954 in 2021 (15 people/km2). In the southern neighboring municipalities (Klana, Jelenje, Čavle, Bakar, and Vinodol Municipality), the population declined from 26,395 to 24,799 in 2021 (46 people/km2) (TIPH PGKC, 1987–2021). Within the sparsely populated Gorski Kotar region almost one-third of participants were presumably exposed at or near their place of residence (73/101; 72.3%).
To assess the activities related to hantavirus infection, individuals were interviewed about their presumed exposure. Participants frequently carried wood (65.7%), lived near the forest (66.3%), and had other woodland recreations (55.2%). These are typical activities, particularly among mountain inhabitants. However, other exposures, such as hunting (4.0%) and attic cleaning (5.8%), that are commonly linked to hantavirus infection were rare (Deutz et al, 2003; Van Loock et al, 1999). Presumed risk factors did not differ significantly in cases from the northern and southern parts of the county (Table 2). We identified 38.8% of individuals who had been occupationally exposed (66/170), with the majority of them working in the forestry or wood industry (41/66), which are the main professions in the Gorski Kotar area. Hantavirus infection is considered an occupational disease, and it is more prevalent among military, forestry, and agricultural workers (Mulić and Ropac, 2002; Riccò et al, 2021). In the large 2002 outbreak in Croatia, only 13.5% of cases were occupation related (Kuzman et al, 2003), and in a 2010 study in Finland that assessed the disease burden of Puumala virus, only 3% of cases were occupationally related (Makary et al, 2010).
The awareness of existing HFRS (before becoming ill) was quite high (82.0%) among cases. The participants from Gorski Kotar areas were more likely to know individuals with HFRS since the outbreak affected the Gorski Kotar region more intensively (Table 2). HFRS can be prevented using personal protective measures, but the reported usage of protective equipment during activities was quite low, especially wearing a mask (27/173; 15.6%). A similar finding was obtained in a 2011–2012 study in Sweden (Gherasim et al, 2015). It is unlikely that forestry/wood workers would use a mask while working, since it is not required as standard personal protective equipment or is recommended on particular occasions during the work process (Macan and Zavalić, 2019; CIHSW, n.d). However, especially during an outbreak, all people at risk are advised by public health services (radio, TV, news, public health services website) to wear masks (CIPH, 2017). There were no additional educational activities conducted during this outbreak. We did not assess the knowledge of disease transmission; therefore, it is possible that participants are not fully aware of how the disease is being transmitted. In addition, the availability of personal protective equipment at work was not evaluated. This study indicates the need for further education through additional public service information on the usage of protective measures for occupational risk group, as well as for the general public in leisure activities, since we have a new area affected with lower awareness of HFRS.
One of the most important risk factors for acquiring hantavirus infection is seeing rodents or their excreta (Piechotowski et al, 2008; Winter et al., 2009). In this study, far more cases reported rodent observation than in other studies (78% vs. 46 and 60%, respectively) (Gherasim et al, 2015; Van Loock et al, 1999; Vapalahti K et al, 2010). This difference was also more pronounced in the northern area compared with the southern part of the county (Table 2). Croatian Forest Ltd. also reported in 2021 the highest rodent abundance in the last 40 years, particularly in the southern part of the county (Matičić, 2021).
The rodent population in temperate Europe is associated with bumper seed or mast years (Bjedov et al, 2016; Clement et al, 2009; Reil et al, 2015). A large production of tree seed, especially oak and beech, results in an abundance of seed-eating rodent species. A higher number of rodents and HFRS cases in humans are noted in the year after the mast year (Reil et al, 2015). The European beech (Fagus sylvatica) is the main representative of deciduous trees in Gorski Kotar. Beech forests and mixed beech-fir forests predominate in this region (Teslak et al, 2016; Matić et al, 2003). In 2020, the Gorski Kotar region recorded a good production of beech seed. This seed production could be a factor influencing this large outbreak.
Another important environmental factor is temperature: higher temperatures improve beech seed fructification and increase the survival of rodents during winter. In one systematic review, a strong positive association was established between temperature and HFRS occurrence in central Europe (Roda Gracia et al, 2015). Compared to the earlier period, especially with the 1960s, Gorski Kotar and neighboring mountain areas have experienced milder winters, higher average temperatures, greater monthly temperature anomalies, and a slight decrease in annual precipitation (Cindrić et al, 2016; Meteoblue, 2023a; Ugarković and Tikvić, 2011; World Bank Group, 2021). Our study found no difference in average temperature between 2021 and previous years, as it has been suggested that average temperatures have been increasing since 2000 (Meteoblue, 2023b). Other climate factors, such as humidity and precipitation, are not consistently associated with hantavirus outbreaks (Luo et al, 2022; Roda Gracia et al, 2015). The average humidity value and precipitation amount in our analysis did not deviate from the average value from 1991 to 2020 (Table 3). Future projections include a warmer and dry climate in Croatia with ‘new hot spots’, especially in the northern part of Gorski Kotar during the winter period (World Bank Group, 2021). It is inevitable that climate change will probably affect the distribution of zoonotic diseases, sometimes with long-term effects and repercussions.
This outbreak was caused by the Puumala virus. The epidemiological department of TIPH PGKC reported 192 cases of HFRS and no deaths to the Croatian Institute of Public Health in 2021 (CIPH, 2022). Additional cases were identified through active case finding by microbiology laboratories, bringing the total number to 202. Infectious diseases are consistently underreported to our national monitoring system. Perhaps the best example is when, in 2002, 320 cases of HFRS were notified to the Croatian Institute of Public Health, but a study with active case finding identified 401 cases (Kuzman et al, 2003). Given that HFRS usually manifests as a subclinical infection (70–80%) (Vaheri et al, 2023) and that not all confirmed cases were recorded in our surveillance system, it is assumed that the 2021 outbreak underestimated the true burden of infection.
The main limitation of this study was the lack of a control group for determining risk exposure. There were no rodent studies conducted in 2021 to demonstrate the extent of the spread of hantavirus infection in this outbreak. A seroprevalence study in humans would provide additional information, particularly in new areas affected by hantavirus infection. In addition, recall bias could influence our study results because participants might not accurately recall details preceding the outbreak. In 2021, all epidemiological services were still engaged in addressing the COVID-19 pandemic, delaying investigation of this outbreak.
Conclusion
With 202 cases reported in 2021, this was the largest outbreak of hemorrhagic fever with renal syndrome ever recorded in PGKC. This outbreak, as well as others in Croatia, was primarily caused by Puumala virus infection. The outbreak reached neighboring territories and spread to the southern part of the county. Despite the large number of cases, no deaths were reported. However, a significant number of people sought hospital care and experienced serious illness and disruption to daily activities. This outbreak was presumably driven by an expanding rodent population. Good seed production conditions and higher temperatures in the period preceding this outbreak probably contributed to its size and spread. The analysis of risk factors, especially those associated with wood handling, provides inputs for a targeted public awareness campaign, particularly for occupational exposure. Based on results of this study, it would be reasonable to advise health policy makers to raise awareness of the risk of HFRS among the exposed population through active educational campaigns, such as lectures or seminars.
Footnotes
Ethics statement
No ethical approval was required, as this investigation was carried out in compliance with the Croatian Act on Population Protection Against Infectious Diseases.
Authors’ Contributions
M.T.: methodology, validation, formal analysis, investigation, and writing—original draft. D.L.: formal analysis, investigation, and writing—review and editing. L.K. and M.B.: investigation and writing. T.V.Č.: investigation and writing—review and editing. B.K.: conceptualization and writing—review and editing. L.H.: conceptualization and writing—review and editing. O.Đ.R.: conceptualization and writing—review, editing, and supervision.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
No funding was received for this article.