
Abstract
Objective:
To study the clinical and laboratory characteristics of hemorrhagic fever with renal syndrome (HFRS) in Chinese elderly patients.
Methods:
The clinical data of hospitalized patients diagnosed with HFRS from 2011 to 2022 were extracted from the inpatient record system of the Second Affiliated Hospital of Air Force Medical University. A comparative analysis was conducted between young and elderly individuals regarding the male-to-female ratio, disease classification, clinical laboratory indices, and prognosis.
Results:
Among the patients diagnosed with HFRS, the elderly population accounted for 14.86%, comprising 199 males and 86 females. The proportion of severe-type cases among elderly patients was 25.96%, while the proportion of critical cases was 32.63%. Critically, the proportion of critical-type cases in this age group was significantly higher compared to individuals aged 20–60 years. Comparing the clinical indices of elderly patients with HFRS with different clinical outcomes, our findings revealed deceased cases exhibited significantly higher body temperature, hemoglobin (HGB) levels, and white blood cell (WBC) counts compared to surviving patients. Conversely, albumin (ALB) levels, fibrinogen (FIB) levels, and platelet counts were significantly lower in deceased patients than in surviving patients.
Conclusion:
The incidence of HFRS in the elderly presents a higher proportion of severe-type and critical-type cases and a greater mortality rate compared to younger individuals. Elevated body temperature, HGB levels, and WBC counts, and lower ALB and FIB levels suggest a poorer prognosis.
Introduction
Population aging is a global phenomenon spreading across the world (Jiang and Feng, 2022). The World Health Organization (WHO) defines individuals aged 60 and above as elderly (WHO, 2015). Based on the United Nations criteria, an aging society is defined as a country or region where more than 7% of its population is aged 65 years or older, or more than 10% is aged 60 years or older. China officially entered the stage of an aging society in 2000 (Peng, 2011). The seventh national census conducted in 2020 found that individuals aged 60 and above constituted approximately 18.7% of China’s overall population, totaling around 264 million individuals (Tu et al., 2022). Moreover, those aged at least 65 accounted for roughly 13.5%, equating to approximately 190 million people (Tu et al., 2022). The demand for elderly care in China is expected to increase by 14.02 million individuals by 2030 (Gong et al., 2022). Furthermore, the proportion of China’s population aged over 65 is projected to reach 35% by 2050 (Wang et al., 2022). China has the largest elderly demographic in the world (Gong et al., 2022). The growing population of individuals aged ≥60 years, coupled with rising illness rates, poses a significant challenge to social welfare and health care systems (Kingston et al., 2017; Feng et al., 2021).
The Orthohantaviruses, as zoonotic pathogens, belong to the genus Orthohantavirus within the Hantaviridae family (Sehgal et al., 2023). The Orthohantaviruses are distributed worldwide (Jiang et al., 2017). Currently, a total of 38 Orthohantavirus species have been identified, with at least 24 implicated in the pathogenesis of two major acute infectious diseases in humans: hemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome (HPS) (Sehgal et al., 2023; Noack et al., 2020). China is one of the countries with a heavy disease burden of HFRS (Sun and Zou, 2018). Based on the National Health Commission’s National Monthly Report on Statutory Infectious Diseases and literature spanning from 1950 to 2020, China has recorded a total of 1,688,031 cases of HFRS. Among these cases, there have been 48,260 subsequent fatalities (Jiang et al., 2022). In China, there has been a notable decline in the overall occurrence of HFRS over the past two decades. Nevertheless, certain regions have experienced recurrent outbreaks (Jiang et al., 2022), and the risk of HFRS is expected to remain elevated until the end of this century (Wang et al., 2024).
The primary virus types causing HFRS in China are Hantaan virus (HTNV) and Seoul virus (SEOV), with HFRS caused by HTNV being more severe, while HFRS caused by SEOV is relatively mild (Jiang et al., 2016). The Shaanxi Province, accounting for approximately one-third of total HFRS cases in China (Wei et al., 2021), has a high incidence of HFRS cases, primarily due to HTNV infection (Zhang et al., 2022). Located in northwest China, Shaanxi has been identified as a hotspot for HFRS cases in the country. It is considered a region with high prevalence of HFRS in China, where HTNV infection prevails and severe cases are predominantly caused by HTNV, resulting in substantial fatality rate (Liang et al., 2018; Wang et al., 2017). The current research examines the clinical and laboratory features in elderly individuals with HFRS, as well as the prognostic factors associated with the disease.
Materials and Methods
Data collection
A doctor with specialized training was appointed to oversee data collection. Data were collected from the patient’s initial laboratory test conducted post-admission, with the patient being 3–5 days into the onset of HFRS. Data primarily consisted of: (1) basic demographic information, including gender and age; and (2) observed clinical symptoms such as body temperature, laboratory test results (white blood cell [WBC] count, platelet count, hemoglobin [HGB] level), different clinical presentations, and overall clinical outcome. Exclusion criteria: (1) absence of classification in the original medical record, (2) undiagnosed condition, and (3) brief hospital stay and incomplete clinical data.
Study population
This study enrolled all patients confirmed with HFRS admitted to the Second Affiliated Hospital of Air Force Medical University from January 2011 to December 2022. Based on the standards of the Chinese society and the WHO, individuals aged over 60 are considered as elderly. The clinical data of elderly patients were specifically chosen and compared to that of other populations. A total of 40 elderly patients with mild-type HFRS were randomly selected based on matching conditions of the same gender and age within ±3 years. Additionally, 40 elderly patients with moderate-type, severe-type, and critical-type HFRS were respectively chosen, and clinical test indexes were collected for analysis. A total of 20 death cases were selected as study subjects, with matching criteria of same gender and age within ±3 years. Additionally, 20 surviving elderly patients were chosen to collect their clinical test indicators for subsequent analysis.
Clinical types and criteria for diagnosis
The diagnostic criteria for HFRS are based on the Diagnostic Criteria for Epidemic Hemorrhagic Fever (WS 278-2008) issued by the Ministry of Health of the People’s Republic of China, ensuring confirmation of all cases. All patients had laboratory confirmation of HFRS by detection of specific serum IgM and IgG antibodies to HTNV using the immune colloidal gold technique. According to the recently published expert consensus on the prevention and treatment of HFRS (Hong Jiang et al., 2022), there are four types based on the severity: (1) Mild-type: body temperature <39°C, skin and mucous membrane petechiae, urine protein of “+ to + +,” and no oliguria or hypotensive shock. (2) Moderate-type: body temperature 39–40°C, marked bulbar conjunctival edema, obvious petechiae on skin and mucous membranes, systolic blood pressure <90 mmHg (1 mmHg = 0.133 kPa) or pulse pressure difference <30 mmHg, oliguria, and urine protein of “++ to ++++” during illness. (3) Severe-type: temperature >40°C, neurological symptoms, shock, and oliguria lasting 5 days or anuria ≤2 days. (4) Critical-type: refractory shock, bleeding from vital organs, anuria >2 days, or other serious comorbidities such as heart failure, pulmonary edema, respiratory failure, coma, and severe secondary infection.
Statistical analysis
The SPSS 23.0 software was used for processing all collected data. The χ2 test and Mann–Whitney U test were employed to compare categorical and continuous variables, respectively. The normal distribution of continuous variables was assessed using the Shapiro–Wilk test. Results were presented as median, interquartile range (IQR), mean ± standard deviation (SD), or frequency and percentage. A p value <0.05 was considered statistically significant. The distribution of clinical test indicators was described using median and interquartile intervals, while statistical analysis was performed using the Kruskal–Wallis H test.
Results
Patients’ general characteristics
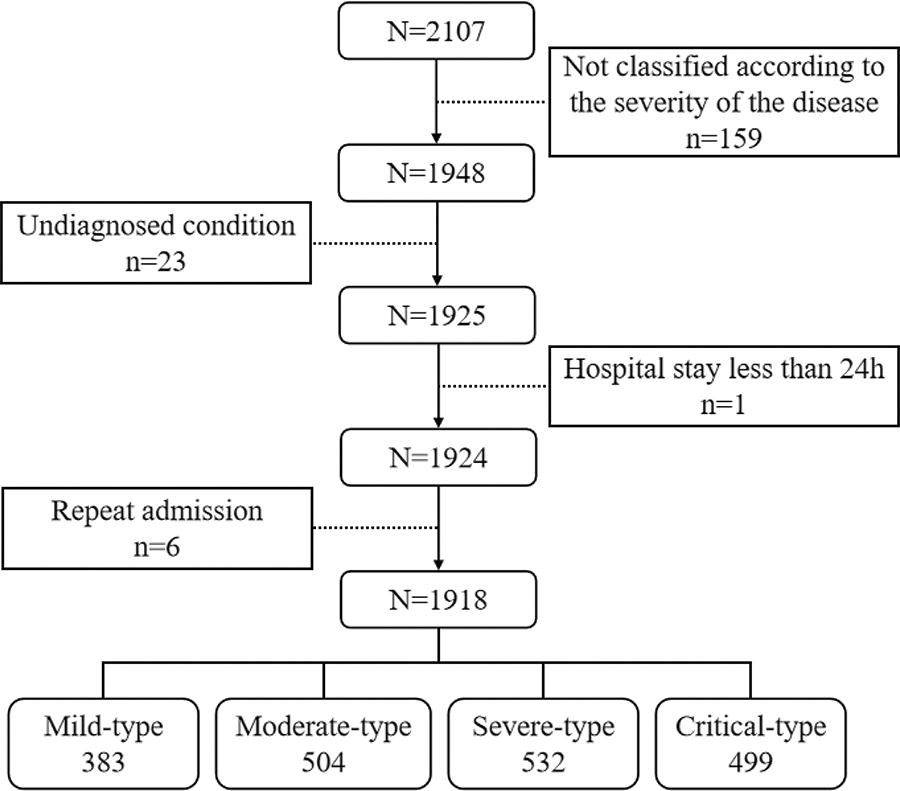
A total of 2107 cases were collected, with 159 cases being excluded, resulting in a final inclusion of 1918 cases (Fig. 1). Among these included cases, there were 1512 males and 406 females, yielding a male-to-female ratio of 3.72:1. The average age was recorded as 42.79 ± 16.02 years old. Out of the total number of patients, 1826 survived, while the remaining 92 unfortunately died. No significant difference in mortality rate was observed between male and female patients. Additionally, there were a total of 285 elderly patients, consisting of 199 males and 86 females; this group accounted for approximately 14.86% of all patients (Fig. 2).
Grouping of the patients.
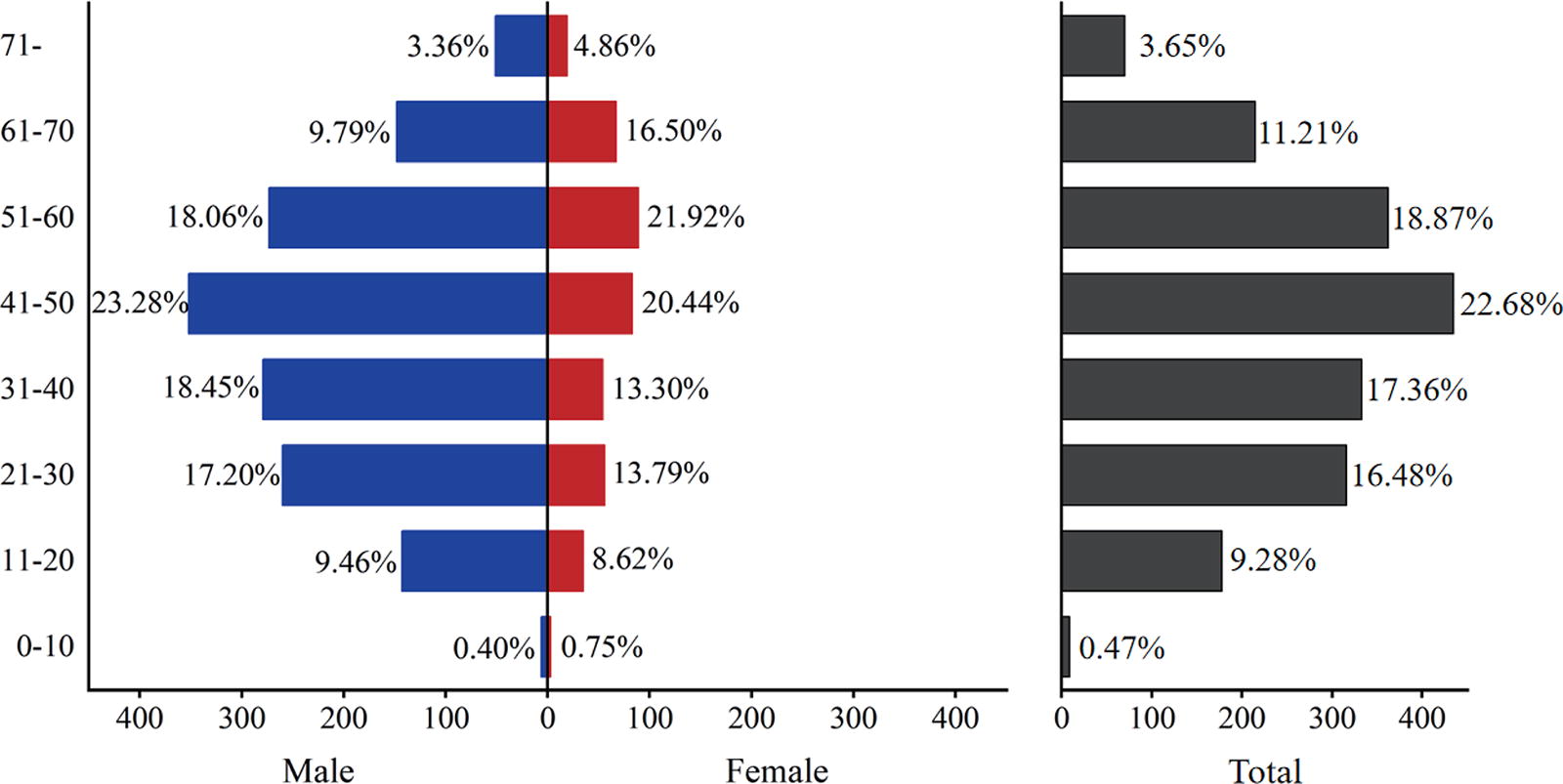
The demographic characteristics of patients in terms of age and gender distribution.
The relationship between gender and HFRS severity
The relationship between gender and HFRS disease severity was examined. Among the cases, 383 were classified as mild-type, 504 as moderate-type, 532 as severe-type, and 499 as critical-type. No statistically significant difference in disease severity was observed between males and females. Disease distribution among patients of different genders is presented in Table 1.
The Relationship Between Gender and HFRS Severity Type
HFRS, hemorrhagic fever with renal syndrome.
Correlation between age and severity of HFRS
With advancing age, there was an observed increase in the proportion of severe-type and critical-type patients with HFRS. Specifically, among the elderly population, 25.96% were classified as severe-type cases while 32.63% were categorized as critical-type cases. Notably, individuals aged over 70 years constituted the highest proportion of critical-type patients, accounting for 34.29% (Fig. 3).
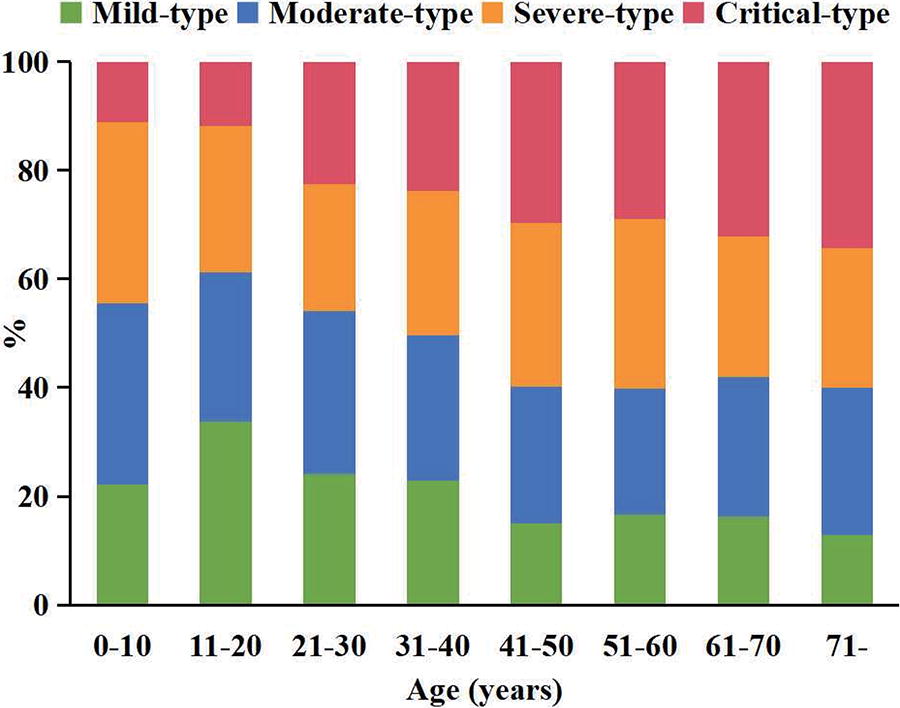
The correlation between age and the severity of HFRS. HFRS, hemorrhagic fever with renal syndrome.
The clinical outcomes of patients across various age groups
The case fatality rate increased with age across all age groups, with the highest rates observed in patients aged 61–70 (6.98%) and over 70 (7.14%). Interestingly, among young adults, the highest fatality rate was found in the 41–50 age group at 6.44%. In the 0–10 age group, although the fatality rate reached 11.1%, there were fewer than 10 cases reported and only one death occurred. It is important to note that these statistical results have limited clinical significance, and further analysis of larger sample data is required (Table 2).
Clinical Outcomes of Patients Across Various Age Groups
Comparison of clinical indices in elderly patients with varying prognosis
There were no significant differences in platelet count, HGB level, and albumin levels among elderly patients with HFRS with different disease types. WBC count was higher in critically type patients compared to mild-type patients, while there was no significant difference in WBC count between medium-type and mild-type patients. Neutrophil count, blood urea nitrogen (BUN), and serum creatinine (Scr) levels were higher in moderate-type, severe-type, and critical-type patients compared to mild-type patients. Prothrombin time activity (PTA) was lower in critical-type patients compared to those with mild-type, moderate-type, and severe-type patients. Fibrinogen (FIB) levels were lower in severe-type patients compared to medium-type patients. Body temperature was higher in critical-type patients compared to moderate-type patients (Table 3 and Fig. 4).
The Distribution of Clinical Index Across Different Groups (Median [P25, P75])
Kruskal–Wallis H test.
Mild-type patients with HFRS as control.
Moderate-type patients with HFRS as control.
Severe-type patients with HFRS as control.
ALB, albumin; BUN, blood urea nitrogen; FIB, fibrinogen; PTA, prothrombin time activity; Scr, serum creatinine; WBC, white blood cell.
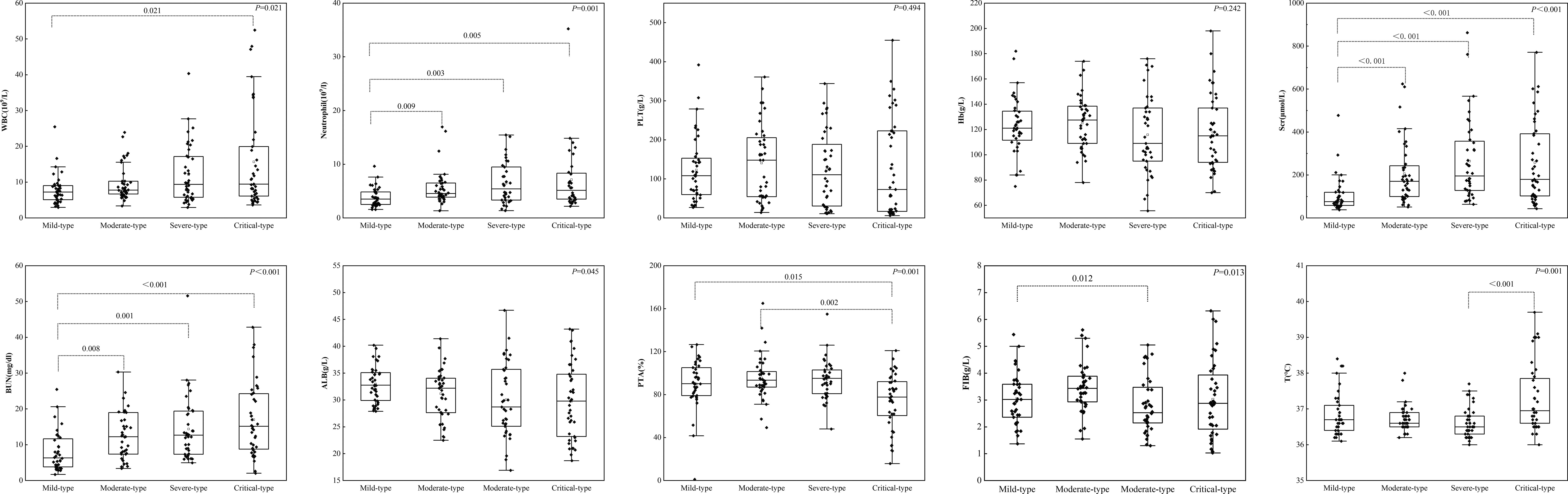
The comparison of clinical indicators among patients with HFRS with different disease severity.
Comparison of clinical indicators in elderly patients with diverse outcomes
Through comparison of the clinical indices of elderly patients with HFRS with different clinical outcomes, the findings revealed that death cases exhibited significantly elevated body temperature, HGB levels, and WBC counts compared to surviving patients. Conversely, albumin (ALB) levels, FIB levels, and platelet counts were significantly lower in deceased patients than in surviving patients. No significant differences were observed in BUN levels, Scr levels, and neutrophil counts (Table 4 and Fig. 5).
Comparison of Clinical Indicators in Elderly Patients with HFRS: Death Versus Survival
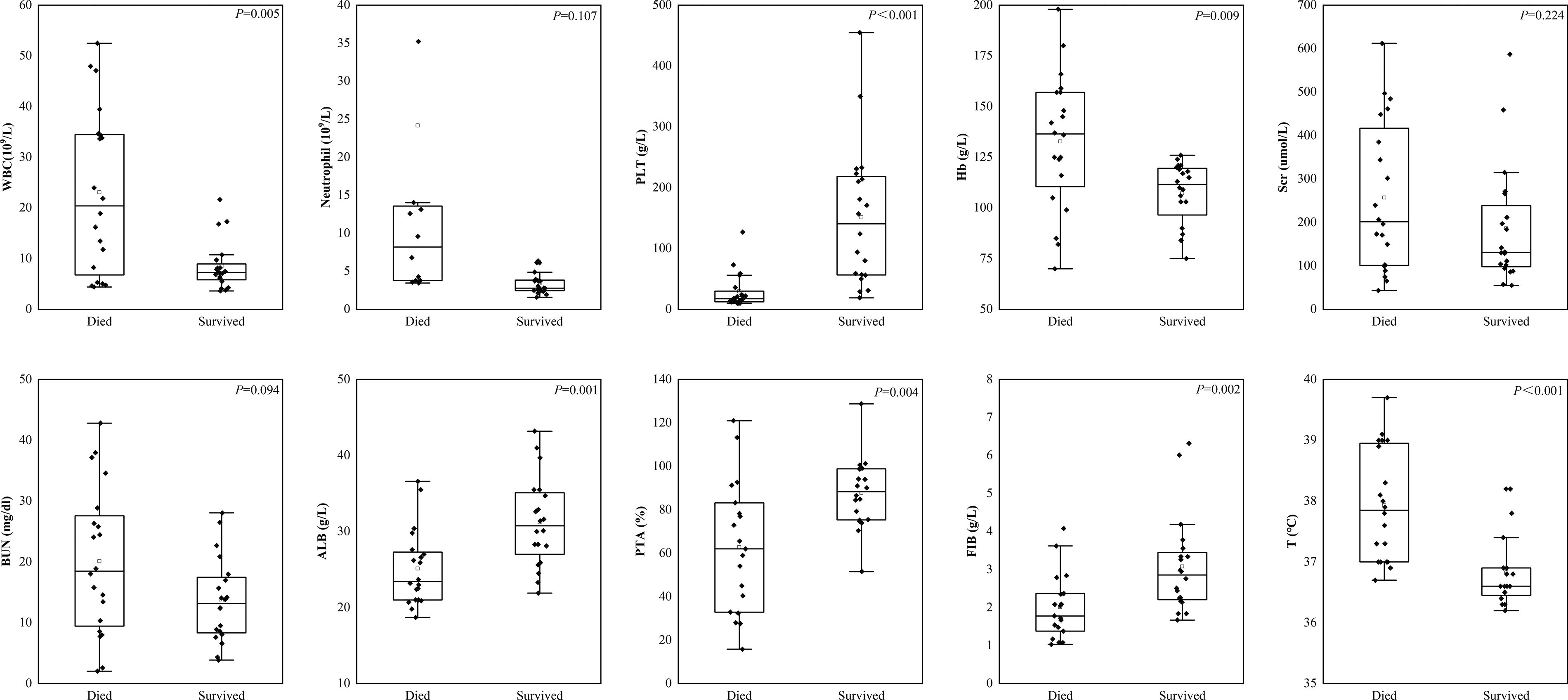
Comparison of clinical indicators in elderly patients with HFRS death and survival cases.
Discussion
Data released by the National Bureau of Statistics of China show that in 2013, the population aged 60 and above reached 202.43 million, accounting for 14.9% of the total national population. Among them, the population aged 65 and above was 131.61 million, representing 9.7% of the total national population. In 2023, China had a population of 296.97 million people aged 60 or above, accounting for 21.1% of the total population. Among them, 216.76 million were aged 65 or above, representing 15.4% of the total population. According to data released by the National Center for Disease Control and Prevention of China, a total of 12,810 cases of HFRS were reported in 2013, resulting in 109 deaths. The incidence rate was 0.95 per 100,000 population, and the mortality rate was 0.01 per 100,000 population. In 2023, a total of 5360 cases of HFRS were reported, resulting in 12 deaths. The incidence rate was 0.3802 per 100,000 population, and the mortality rate was 0.0009 per 100,000 population. As the total number of HFRS cases in China has decreased in recent 10 years, the overall incidence rate declines, while the elderly population grows, leading to a downward trend in HFRS incidence among the elderly in China. This study found that the proportion of elderly patients among HFRS cases is increasing, aligning with the growing proportion of the elderly population in Chinese society. The disease characteristics of HFRS in the elderly population warrant particular attention.
The 2020 China Health Statistics Yearbook revealed that in 2019, 40.01% of hospital discharges involved individuals over 60 years (National Bureau of Statistics of China, 2022). This study found a higher proportion of critical-type HFRS cases among elderly patients compared to young adults, with increased mortality rates in critical-type patients, corroborating the findings. In our previous study involving 2245 patients with HFRS, we found that 30-day mortality rate in patients with HFRS was closely associated with several indicators, including hypertension, hypotensive shock, hypoxemia, neutrophil counts, AST, and APTT (Hu et al., 2024). The decline in organ function, often accompanied by underlying conditions such as hypertension and diabetes, may contribute to increased mortality rates in the elderly. However, further large-scale studies are needed to compare and analyze the prognostic risk factors across different age groups. In 1994, China developed bivalent inactivated vaccines against HTNV and SEOV approved by the Pharmacopoeia of China in 2005 (Liu et al., 2020). While individuals with incomplete vaccination may still experience mild symptoms, HFRS cases occur. Effective immunization requires adequate vaccine doses and booster shots (Chen et al., 2016). The vaccine leaflet indicates that individuals aged 16–60 constitute the primary demographic for initial vaccination. Vaccinating the elderly against HFRS remains an unresolved challenge in China (Jiang et al., 2022).
The WBC count is considered a prognostic indicator for the development of severe HFRS in pediatric patients (Li et al., 2023). This study revealed that elderly patients with critical-type HFRS exhibited higher levels of WBCs compared to those with mild-type HFRS. It has been observed that endothelial cells infected with hantavirus trigger the activation of neutrophils (Strandin et al., 2018). This activation potentially contributes to the severity of HFRS through kidney pathology (Strandin et al., 2018). Our previous study demonstrated a significant association between neutrophil count and mortality risk (Hu et al., 2024), consistent with the results of this current study. Although the use of a simple admission-based biomarker index, known as APRI, has been proposed to identify the risk of unfavorable outcomes in patients with HFRS (He et al., 2023), it was not employed in this study. The combination of WBC count, aspartate aminotransferase, prothrombin time, and FIB has been shown to have satisfactory diagnostic capability for predicting the prognosis of patients with HFRS (Du et al., 2014). However, no significant association was observed between platelet count and disease severity in elderly patients with HFRS.
The development of Orthohantavirus infections has been widely attributed to the immune response triggered by the virus. The cytokine storm triggered by Orthohantavirus infection plays a pivotal role in the pathogenesis of HFRS (Garanina et al., 2019), with macrophage-induced secretion of Tumor Necrosis Factor-α (TNF-α) serving as the central component (Ma et al., 2024). Severe cases exhibited notably elevated levels of Soluble Tumor Necrosis Factor Receptor 1 (sTNFR1), Interleukin-6 (IL-6), IL-8, and IL-10 compared to mild/moderate cases (Kyriakidis and Papa, 2013). The elevation of body temperature is closely associated with the occurrence of a cytokine storm, which results in increased vascular permeability and the extravasation of water and small molecules (Sehgal et al., 2023; Jiang et al., 2016). This clinical manifestation is characterized by elevated hemoglobin levels (HB). It can be inferred that higher body temperatures indicate a more severe cytokine storm (Garanina et al., 2019), as evidenced by deceased patients exhibiting both higher body temperatures and HB levels. Acute renal failure is a critical manifestation in HFRS cases (Sehgal et al., 2023). This study found a significant correlation between BUN and Scr levels and disease severity, consistent with prior literature (Jiang et al., 2016; Tariq and Kim, 2022). Interestingly, fatal cases and survivors did not show statistically significant differences in these three indicators. Disparities between the two groups may not have been fully captured due to the widespread use of continuous renal replacement therapy (CRRT) among hospitalized patients with severe HFRS.
This study has several limitations. First, the data primarily originate from a general hospital, thereby representing the comprehensive situation within this region, but it is important to acknowledge the potential presence of certain biases. Second, the present study addressed the confounding effects of age and sex by employing propensity scores, thereby ensuring comparability among the groups. It is worth noting that elderly individuals often exhibit comorbidities, which can potentially impact prognosis; however, this study did not account for the influencing factors associated with these underlying diseases. Third, the number of clinical indicators included in this study is still relatively limited, and the time period for including laboratory indicators is too broad. This may not effectively capture the dynamic changes experienced by some severe patients upon admission or in subsequent days.
Conclusion
With China’s aging society, the proportion of elderly individuals has increased among patients with HFRS, and the case fatality rate is significantly higher in elderly patients compared to young and middle-aged patients. Upon hospital admission, elevated WBC counts, increased neutrophil counts, and decreased platelet counts were observed in older patients with HFRS, indicative of a higher likelihood of severe disease and mortality. Vaccine development suitable for elderly individuals is critically important to enable active HFRS prevention through vaccination.
Compliance with Ethics Guidelines
The present study has obtained ethics committee approval from the Tangdu Hospital of the Fourth Military Medical University (No. K202108-14).
Footnotes
Authors’ Contributions
H.J. and L.W. contributed to the study conception and design. X.C., Y.J., H.D., W.W., Y.Z., X.Z., and X.W. performed literature preparation, designed graphs and tables, and collected data. Y.J. painted the graphs. The first draft of the article was written by X.C., Y.J., H.D., W.W., Y.Z., X.Z., X.W., and P.B. All authors read and approved the final article.
Author Disclosure Statement
All authors declare they have no conflicts of interest.
Funding Information
This work was supported by the Discipline Innovation and Development Program of Tangdu Hospital of the Fourth Military Medical University, No. 2021LCYJ025, and the Discipline Boosting Program Project of the Tangdu Hospital of the Fourth Military Medical University, No. 2024JSYX010.