
Abstract
Monitoring circulating rubella IgG antibody concentration in children and in women of child-bearing age is an important step in maintaining high levels of rubella immunity and preventing congenital rubella syndrome. The objective of this study was to evaluate the Beckman Coulter Access Rubella IgG assay against the Dade Behring Enzygnost Anti-Rubella-Virus/IgG EIA assay in serum of children (n = 342) immunized with two doses of measles-mumps-rubella-II (MMR-II) vaccine. We found that the two assays had a high qualitative (96%), and quantitative correlation 0.93 (0.92, 0.95), based on a protective antibody concentration of ≥15 IU/mL. The mean rubella antibody concentration measured by both assays was >37 IU/mL; however, 10% of our study participants had low concentrations of circulating rubella-specific antibodies. These findings might indicate a need for additional monitoring of antibody levels as these children reach child-bearing age, or potentially a need for a third dose of vaccine to increase seroconversion.
Introduction
The rubella-specific IgG enzyme immunoassay (EIA) is the quickest and easiest assay used to determine rubella immunity in large numbers of subjects. There are a number of kits currently on the market, and publications are available that compare some of them (7,8,10). The Dade Behring Enzygnost Anti-Rubella-Virus/IgG EIA kit has previously been used in our laboratory to study the humoral immune response following rubella vaccination (14); however, due to its limited availability in the U.S. we had to search for an alterative assay. We chose the Beckman Coulter Access Rubella IgG assay based on its quantitative measure (expressed in IU/mL), high-throughput capabilities, standardization against the World Health Organization (WHO) Reference Preparation, and the Mayo Clinic Immunochemical Laboratory's familiarity with the Access system. Here we report the comparison between the Dade Behring and the Beckman Coulter assays in terms of concordance and reproducibility.
Materials and Methods
Study participants
Descriptions of the identification and recruitment of this study cohort have been previously published (14,15). Briefly, we conducted a large population-based, stratified, random-sample study to assess associations between HLA genes and immune responses to measles-mumps-rubella-II (MMR-II) vaccine in healthy children and young adults in Olmsted County, Minnesota. The study subjects (n = 346) had documentation in their medical records of having received two doses of the MMR-II vaccine (Merck Research Laboratories, West Point, PA), which contains the RA27/3 Wistar strain of the RV. All of the study participants lived in a geographical area that has not had any cases of wild-type RVs circulating during their lifetime. The Mayo Clinic's Institutional Review Board granted approval for the study, and blood was drawn after informed consent and assent was obtained from each individual and parents or guardians of the subjects. Of the 346 original study participants, four did not wish to be included in any future studies, leaving 342 subjects.
Rubella IgG enzyme immunoassays
Serum from each subject was collected from clotted whole blood (5 mL) by room temperature centrifugation at 900 × g. Serum aliquots were stored at −80°C until the immunoassays were performed. Immunoassays from Dade Behring (Enzygnost Anti-Rubella-Virus/IgG enzyme immunoassay; Marburg, Germany) and Beckman Coulter (Access® Rubella IgG; Fullerton, CA) were performed in 2002 and 2007, respectively, in duplicate according to the manufacturer's instructions. These two independent assays were performed using separate aliquots of the same serum. The Dade Behring assay is an enzyme-linked immunosorbent assay (ELISA), which has previously been described in detail (15). The limit for a non-reactive rubella-specific antibody concentration was 4 IU/mL, and our laboratory's coefficient of variation was 4%. The Beckman Coulter Access Rubella IgG assay is an automated, paramagnetic particle chemiluminescent immunoassay for the detection of rubella-specific IgG in human serum. The assay is designed for use on any of the Beckman Coulter Access Immunoassay systems, and was performed on the UniCel® DxI 800 Access® Immunoassay System (Beckman Coulter). Antibody levels are determined from a multi-point calibration curve standardized against the WHO reference preparation for anti-rubella serum. For this assay the limit for a non-reactive rubella-specific antibody concentration was 10 IU/mL, the lower threshold of the analytic measurement range was 0.5 IU/mL, and the coefficient of variation was 6%.
Statistical analysis
Data were descriptively summarized using frequencies and percentages for categorical variables and means, and 95% confidence intervals for continuous variables. Plots of antibody concentrations for both assays suggested moderate to high levels of data skewness; therefore all calculations of summary statistics and all formal statistical analyses for these measures were carried out using log transformed values. The resulting mean values and confidence intervals were then back-transformed and thus expressed in their original sampling units, effectively yielding geometric mean concentration (GMC) values. We visually displayed associations between the two assays using scatterplots and Bland-Altman plots (2). Linear associations were summarized using Pearson correlation coefficients and corresponding 95% confidence intervals. We evaluated the reproducibility of antibody concentrations across assays using Lin's concordance correlation coefficient (11). Briefly, this coefficient measures the degree to which the paired assay values fall on the 45° line through the origin. It can be interpreted as a combined assessment of precision and accuracy, and yields results nearly identical to certain types of intraclass correlation coefficients (13). Analyses were carried throughout and by levels of demographic and clinical characteristics. We used partial correlation coefficients to evaluate the linear association between the two (log-transformed) assays after adjustment for the potential confounding effects of age at enrollment, gender, race, age at first rubella vaccination, and age at second rubella vaccination. According to the manufacturer protocol for the Beckman assay, antibody concentrations equal to or above 15 IU/mL can be considered protective. We categorized all values based on this cut-point and assessed reproducibility of immune status across assays using percent agreement and kappa coefficients. Secondary analyses further subdivided the non-reactive subjects: values below 10 IU/mL were classified as not immune, and values of at least 10 IU/mL but less than 15 IU/mL were classified as equivocal. Percent agreement and kappa coefficients were then recalculated using this three-level categorical variable. The Dade Behring assay indicates a protective immune status when rubella IgG concentrations are ≥7 IU/mL. Because this value is less than what is commonly regarded as the minimum level of protective immunity (17), we chose to not use the Dade Behring limits for our comparison. Analyses were carried out using the SAS version 9 (SAS Institute, Inc., Cary, NC) and S + version 8 (Insightful Corporation, Seattle, WA) software systems.
Results
Table 1 illustrates the demographic and clinical variables of the study population. The age at enrollment ranged from 11 to 19 y and was evenly distributed at each age interval. The study population had near equal gender distribution (53% males), and a large majority of Caucasians (94%) (14,15). The mean antibody concentrations were 37.7 UI/mL and 39.2 UI/mL for the Dade Behring and Beckman Coulter assays, respectively.
95% CI = 95% confidence interval.
A comparison of how each sample was classified as negative or positive by both assays are shown in Table 2. The criterion for a positive classification was ≥15 IU/mL. Further classification of the negative values into negative or equivocal is demonstrated in Table 3.
Percent agreement (95% CI): 96% (94%,98%).
Kappa coefficient (95% CI): 0.7714 (0.6562,0.8866).
95% CI = 95% confidence interval.
Percent agreement (95% CI): 95% (92%,97%).
Weighted kappa coefficient (95% CI): 0.7398 (0.6258,0.8539).
95% CI = 95% confidence interval.
Bland and Altman analysis was performed to look for even distribution across all samples. The mean of the assays was plotted against the difference of the assays and the mean difference and twice the standard deviations were also plotted (Fig. 1). There are no systematic differences in the data if greater than 95% of the samples lie between the standard deviation lines, and 97% of our data points fell between two standard deviations of the mean difference in antibody concentration.
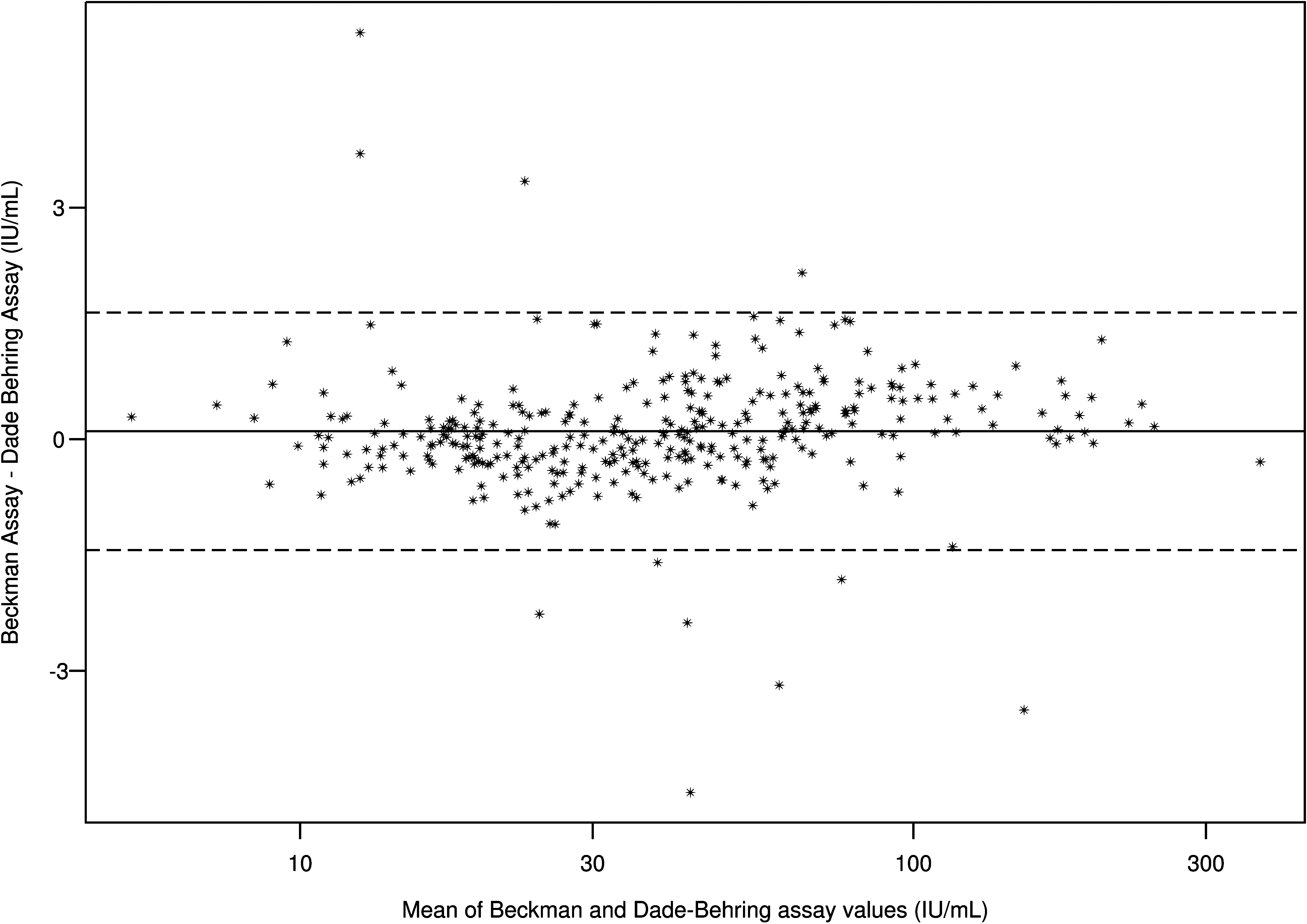
Bland and Altman analysis of the Beckman Coulter and Dade Behring Rubella IgG immunoassays. The y-axis shows the Beckman Coulter antibody concentration minus the Dade Behring antibody concentration, while the x-axis is the mean antibody concentration for the two assays. The mean difference in antibody concentration is plotted as the solid line, and the dashed lines represent twice the standard deviations.
Both the Pearson correlation coefficient (r = 0.93; 95% CI 0.92,0.95) and Lin's concordance measure (r = 0.93; 95% CI 0.91,0.94) of the quantitative assay values were very high for the 342 samples. These values remain high when the data are separated into separate variables (Table 1). This shows that the Beckman Coulter assay compares favorably to the Dade Behring assay, regardless of age or gender.
Of the 342 subjects, only 18 subjects (5%) did not agree. This number was determined by taking into account four equivocal assay values. Table 4 illustrates the mean antibody concentration and immune status for those 18 subjects. Of these 18 subjects only one (subject r) was classified as positive by the Dade Behring assay and negative by the Beckman Coulter assay, and one (subject p) was classified as negative by the Dade Behring assay and positive by the Beckman Coulter assay. Subject (p) was very close to being classified as equivocal by both tests, and an additional eight subjects missed agreement by 0.5 IU/mL or less. In contrast, two subjects (subjects c and j) had rubella-specific antibody concentrations of 12.5 IU/mL by the Dade Behring assay, and were classified as highly positive by the Beckman Coulter assay. Each of these samples would require more testing, including a rubella neutralizing antibody assay, to definitively classify their immune status.
Discussion
Our results indicate that the Dade Behring and Beckman Coulter assays had a high level of agreement based on immune status when using a standardized cut-off to determine the level of protective immunity. We demonstrated that rubella antibody concentration did not agree for approximately 5% of the subjects.
One possible reason the rubella IgG test results differed between assays is that each assay uses a different rubella strain, which is in turn different from the strain present in the MMR-II vaccine. The MMR-II vaccine contains the RA27/3 Wistar strain. The Dade Behring assay uses the B-1272 strain and the Beckman Coulter assay uses the HPV 77 RV strain in their assays. It has been shown that strain-specific epitopes of RV exist (4,9); therefore it is possible to have individuals immunized with one strain of RV produce antibodies that are not recognized by the rubella antigen epitopes used in these EIAs. How significant such strain differences are in accurately predicting immunity remains to be seen. An additional limitation is that these assays only measure rubella-specific antibody concentrations, not rubella-neutralizing antibody titers. Neutralizing antibody titers are the gold standard measure of vaccine-induced humoral immune responses, given the prominent role that these antibodies play in rubella immunity (1). However, in a large population-based study like ours, rubella neutralizing antibody assays are not always feasible to perform, as they are cost- and labor-intensive. Also, we did not determine antibody characteristics such as binding avidity and affinity, which would help to determine the quality of the antibody response in addition to the magnitude of the response. Keeping in mind good correlation between neutralizing antibodies and IgG levels, we did not perform neutralization assays on the negative and equivocal samples. However, in our future population-based vaccine studies we will select both negative and equivocal samples and perform neutralizing assays on these.
Because of the racial make-up of Olmsted County, Minnesota, our study population was predominantly Caucasian. There was good rubella IgG antibody concentration correlation for both whites and non-whites; however, because of the small sample size of non-whites, any conclusions about other populations would require further study.
Our results indicate that even after two doses of MMR-II vaccine, nearly 10% of healthy children in Olmsted County, Minnesota, do not have a protective concentration of rubella IgG antibodies. These findings support the growing sentiment that a third dose of MMR may be necessary, or at the very least a screening process should be used to identify high-risk individuals such as women of child-bearing age, who may require a third dose (5,6).
In conclusion, the Beckman Coulter Access system provided excellent agreement with the Dade Behring Enzygnost assay, and can be considered an alternate platform for laboratories unable to access the Dade Behring product.
Footnotes
Acknowledgments
We would like to thank the parents and children for their involvement in this study. We would also like to thank the fellows, nurses, and students from the Mayo Vaccine Research Group for their efforts. We thank the Mayo Clinic Immunochemical Core Laboratory for their work. We acknowledge Cheryl Hart for her editorial assistance in preparing this manuscript. This work was supported by grants AI 33144 and AI 48793 from the National Institutes of Health. This publication was made possible by grant number 1 UL1 RR024150-01 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and the NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. The Mayo Clinic's Institutional Review Board granted approval for the study, and blood was drawn after informed consent and assent was obtained from each individual or parents or guardians of all subjects.
Author Disclosure Statement
Dr. Poland is the chair of a safety evaluation committee for novel non-rubella vaccines being developed by Merck Research Laboratories. No competing financial interests exist for the other authors.