
Abstract
Reactivation of human cytomegalovirus (HCMV) remains a serious problem in immunosuppressed individuals. To investigate whether a change in the immune status can be used as an earlier marker for HCMV reactivation than the traditional PCR analysis, eight chronic lymphocytic leukemia (CLL) patients at risk for reactivation due to commencement of alemtuzumab (anti-CD52) treatment were longitudinally followed. Five series of consecutive weekly blood samples were immunophenotyped by flow cytometry to cover both the innate and adaptive immune responses. Concurrently, patients were monitored by PCR for HCMV reactivation. We found a minor upregulation of the early activation marker CD69 on NK cells immediately before HCMV was detected in circulation by PCR. Interestingly, for the specific immune response, CD69 was highly upregulated on CD3+ T cells, especially for the CD8+ subset, in the two patients experiencing an HCMV reactivation between 6 and 20 d before HCMV viremia was measured by PCR. Moreover, a CD4+:CD8+ ratio lower than 0.6 may indicate a trend toward an increased risk for viral reactivation. In conclusion, an increase in CD69 expression is a promising candidate as an early predictor of HCMV reactivation.
Introduction
Patients refractory to standard therapy such as combined fludarabine and cyclophosphamide are often treated with anti-CD20 humanized monoclonal antibodies against the malignant clone. A third choice of therapy in these patients is alemtuzumab, which is a recombinant humanized IgG1 monoclonal antibody directed against the CD52 antigen (5). Such therapy induces a further level of immunosuppression in these patients, since CD52 is highly expressed on both mature normal and malignant lymphocytes, and is also found on monocytes, macrophages, and eosinophils (6). Alemtuzumab thus targets not only malignant cells, but also affects normal, healthy immune cells by antibody-dependent cell cytotoxicity and complement-dependent cytotoxicity (7,8).
Viral infections are often observed at the beginning of the third week of alemtuzumab treatment, which coincides with the nadir in T-cell numbers (9). Clinically, the human cytomegalovirus (HCMV) is the most common opportunistic infection observed in alemtuzumab-treated patients (10,11). PCR is becoming the gold standard for detecting such reactivation (12,13). However, a lag phase between viral reactivation and PCR positivity has been reported (14), and if a remote laboratory does the PCR test, the results may take days to arrive. We hypothesized that immune alterations might precede PCR positivity, and that flow cytometry could reveal such changes. Inasmuch as most centers are already doing flow cytometric evaluations, this could be a clinically useful approach. To this end, we followed eight CLL patients by five consecutive weekly blood samples immediately after initiation of alemtuzumab treatment. Both the innate and adaptive immune responses were monitored by multiparameter flow cytometry, because both have been shown to be important in the defense against HCMV (15,16).
Materials and Methods
Patient sampling
Eight patients with CLL were enrolled in this study at the beginning of alemtuzumab therapy. Prior to alemtuzumab treatment, each subject had received other types of cytoreductive interventions. Along with other important demographic patient data, the specific therapies are outlined in Table 1. Five consecutive blood samples of 45 mL each were collected in EDTA vacuum tubes weekly for 5 wk. Informed consent was obtained from each individual, and the Central Denmark Region Committees on Biomedical Research Ethics approved the study.
F, fludarabine; C, cyclophosphamide; R, rituximab; H, hydroxydaunorubicin; O, Oncovin (vincristine); P, prednisolone; DHAP, dexamethasone, cytarabine, cisplatin; Ch, chlorambucil; CLL, chronic lymphocytic leukemia; HCMV, human cytomegalovirus; PCR, polymerase chain reaction.
Peripheral blood mononuclear cells (PBMCs) were isolated by density gradient centrifugation using OptiPrep® (Axis Shield, Oslo, Norway), according to the manufacturer's instructions. Subsequently, the PBMCs were cryopreserved in a solution of 70% RPMI-1640 containing NaHCO3, 20% (v/v) heat-inactivated fetal calf serum (Biochrom, Cambridge, U.K.), and 10% (v/v) dimethyl sulfoxide (Sigma-Aldrich, St. Louis, MO), and stored at −135°C until use. Plasma was isolated from the blood samples and stored at −80°C until use.
HCMV diagnosis
The plasma samples were retrospectively analyzed for HCMV-specific IgM and IgG antibodies by enzyme-linked immunosorbent assay at the Department of Clinical Microbiology, Aarhus University Hospital Skejby, Denmark.
Semi-quantitative PCR was done by purifying DNA from plasma using the MagNA Pure LC robot and the MagNA Pure LC Total Nucleic Acid Isolation Kit (Roche Applied Science, Penzberg, Germany). qPCR was performed on two HCMV gene sequences, US17 and UL122. The sequence of the US17 forward primer was 5′-CTGCGTCACGGGTCTAGC-3′, the sequence of the US17 reverse primer was 5′-TGCAGGTAAAGTGCGATCAAG-3′, and the sequence of the US17 probe was 5′-TGATCGGCGTTATCGCGTTCTTGATC-3′ (DNA Technology, Aarhus, Denmark). The sequence of the UL122 forward primer was 5′-ATGAAGCGCCGCATTGAG-3′, the sequence of the UL122 reverse primer was 5′-CGATGGCCCGTAGGTCA-3′, and the sequence of the UL122 probe was 5′-ACTGGGCAAAGACCTTCATGCAGATCTC-3′ (DNA Technology). All probes were labeled at the 5′ end with 6-carboxyfluorescein, and at the 3′ end with 6-carboxytetramethylrhodamine.
Each PCR contained 12.5 μL of TaqMan Universal PCR Master Mix (2×; Applied Biosystems Inc., Foster City, CA), 5 μL DNA, 0.3 μM of each of the two primers, and 0.1 μM of the TaqMan probe. Each reaction was carried out in a separate tube in triplicate. qPCR was performed using the MX3000 PCR instrument (Stratagene, La Jolla, CA), and the amplification conditions were 50°C for 2 min and 95°C for 10 min, followed by 50 cycles of 95°C (15 sec), and 60°C (1 min). The threshold cycle (Ct) value was the point at which the fluorescence exceeded a threshold limit of 0.1. The cut-off Ct of <40 was used to define a sample as positive.
Flow cytometry
Cryopreserved PBMCs were thawed in a 37°C water bath and washed in PBS containing 20% fetal calf serum. Subsequently, the cells were washed in PBS with 0.5% bovine serum albumin and 0.09% NaN3.
Expression of cell surface markers was determined by staining the cells for 25 min with titrated concentrations of the following combinations of antibodies: anti-CD69 FITC (clone L78; BD Biosciences, San Diego, CA), anti-NKG2A PE (clone Z199; Beckman Coulter, Fullerton, CA), anti-CD3 ECD (clone UCHT1; Beckman Coulter), anti-CD19 ECD (clone HD237; Beckman Coulter), anti-CD14 ECD (clone RMO52; Beckman Coulter), anti-NKG2C APC (clone 134591; R&D Systems, Minneapolis, MN), and anti-CD56 PC7 (clone N901; Beckman Coulter). Additionally, the cells were stained with anti-CD3 ECD, anti-CD4 PC7 (clone SFCI12T4D11; Beckman Coulter), and anti-CD8 PC5 (clone B9.11; Beckman Coulter), in combination with either anti-CD69 FITC, or anti-CD62L FITC (clone FMC46; Dako, Glostrup, Denmark), and anti-CD45RA PE (clone 4KB5, Dako). After incubation, the cells were washed twice in PBS with 0.5% bovine serum albumin and 0.09% NaN3, before being fixed in 0.09% (v/v) formaldehyde.
All samples were analyzed within 24 h using an FC500 flow cytometer (Beckman Coulter), collecting approximately 300,000 to 500,000 gated lymphocytes. FlowJo software (TreeStar Inc., Ashland, OR) was used for analysis. To verify the compensation matrices, single-stained samples and “fluorescence-minus-one” (17) samples were employed.
Results and Discussion
To evaluate whether components of the immune system can be used for an early diagnosis of HCMV reactivation, we enrolled five HCMV-seropositive (IgM−/IgG+), and three HCMV-seronegative (IgM−/IgG−) patients diagnosed with CLL. Using a semi-quantitative HCMV-specific PCR, we identified HCMV reactivation in two patients. One patient (case 1) reactivated during the third week of surveillance, whereas the other patient (case 2) reactivated during the fifth week (Table 1). No signs of HCMV disease were observed.
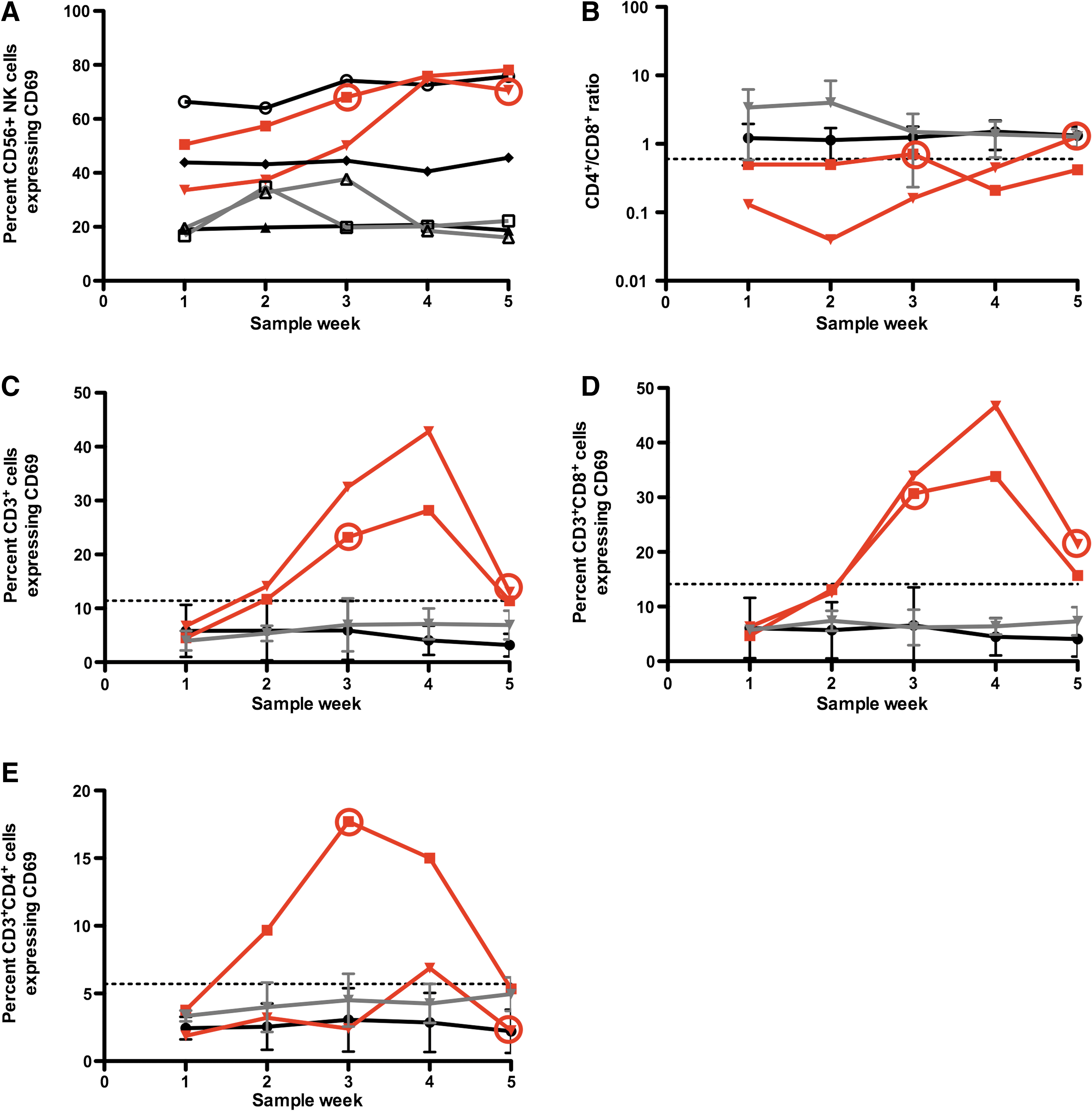
Natural killer (NK) cells are key players during the innate immune response, and they are important for protection against viral herpes infections (15). We therefore examined the NK cell response to HCMV reactivation. Previously we have shown that short-term (24 h) co-culture with HCMV-infected fibroblasts induces a strong expression of the early activation marker CD69 on NK cells in vitro (18), and we hypothesized that the same could also be true in vivo. Corroborating this, we found a slightly increased percentage of NK cells expressing CD69 (Fig. 1A). Conversely, this fraction remained constant in the non-reactivating seropositive controls, but some variation in CD69 expression was found for the seronegative controls. Because 20–80% of the NK cells were already in an activated state (CD69-positive) during all 5 wk of observation, a single measurement of CD69 on NK cells is not an adequate predictor of HCMV reactivation.
(
A positive HCMV serostatus is correlated with an expansion of a subpopulation of NK cells expressing the activating receptor CD94/NKG2C+ in healthy individuals, human immunodeficiency virus-infected patients, and in CLL patients alike (19 –21). We therefore measured the expression of the activating CD94/NKG2C receptor and the inhibitory CD94/NKG2A receptor in our patients. However, no relation to HCMV reactivation was found (data not shown).
Next, the T-cell response was evaluated. In CLL patients, an increase in the number of CD8+ T cells leads to an abnormally low CD4+:CD8+ ratio (22,23). In our study, this ratio was lower for the HCMV-reactivating patients than in the non-reactivating patients (Fig. 1B). Moreover, all non-reactivating HCMV-seropositive and HCMV-seronegative patients had a CD4+:CD8+ ratio above 0.6. For healthy controls the CD4+:CD8+ ratio is approximately 2 (24). Though our sample was small, our data suggest that a CD4+:CD8+ ratio below 0.6 indicates an increased risk of HCMV reactivation.
With respect to CD3+ T cells, patients with HCMV reactivation had a higher percentage of activated (CD69+) T cells than did non-reactivating patients (Fig. 1C). Between 1 and 3 wk before HCMV reactivation was detected by PCR, the percentage of activated T cells in both reactivating patients increased to more than two standard deviations above the mean for non-reactivating seropositive patients (i.e., more than 11.4% of the T cells were CD69-positive).
Subsequently, the T cells were divided into cytotoxic CD8+ and CD4+ helper T cells. The CD8+ T cells behaved very much like the CD3+ T cells, with more than 14% of the CD8+ T cells expressing CD69 in the two reactivating patients, between 6 and 20 d before HCMV viremia was detected by PCR (Fig. 1D). The same tendency was observed for the CD4+ T cells; however, it was not as pronounced as for the CD8+ T cells (Fig. 1E). Together, these data suggest that even though these patients have an abnormal and in some ways highly suppressed immune system, T cells were able to react to HCMV reactivation. For renal transplant patients, Karpinski et al. found a positive correlation between HCMV reactivation and CD69 expression on CD8+ T cells, whereas no correlation was found for CD4+ T cells. However, CD69 expression on T cells could not be used as a diagnostic test for renal allograft rejection (25). We found an increase in CD69 expression up to 20 d prior to when HCMV viremia could be detected by PCR. Even though the clinical setting is different, and different immunosuppressive drugs have been used, both Karpinski's and our study show a positive correlation between CD8+CD69+ expression and HCMV reactivation. Thus our study adds to the understanding of the immune response to HCMV reactivation.
Because the patients were undergoing alemtuzumab treatment, and thus were highly immunosuppressed, we evaluated whether in addition to upregulating CD69, the T cells could also mount a change in phenotype in response to HCMV reactivation. Cells were sub-classified into naïve, central memory, effector, and effector memory cells. At the time of reactivation (week 3 for case 1), an immediate shift in CD8+ T cells from effector memory (CD3+CD8+CD62L−CD45RA+) to effector (CD3+CD8+CD62L−CD45RA−) cells was observed. This shift was followed by an increase in central memory cells (CD3+CD8+CD62L+CD45RA−) 2 wk after reactivation (data not shown). This constitutes a surprisingly normal immune response in these severely immunosuppressed patients, and suggests that immunostimulation would be theoretically possible, even in these patients. The other patient (case 2) did not reactivate until the fifth and final sample, so any changes in phenotype could not be observed. All the non-reactivating patients had a fairly stable percentage of effector cells, whereas some variation in the other phenotypes was observed over time. The changes in CD4+ T-cell phenotype resembled those observed for the CD8+ T cells (data not shown).
In conclusion, this study of a limited number of closely-followed CLL patients has shown that CD69 upregulation on T cells is a candidate for an early immune marker for HCMV reactivation. This finding should be seen in light of the widespread use of flow cytometry in hematological departments, unlike PCR detection of HCMV, which is usually outsourced to other laboratories, which delays the availability of the results. During the routine blood sample staining done in a hematological laboratory, labeling for either CD3 or CD8 in combination with CD69 could easily be included. Naturally, more CLL patients and other patients at risk for HCMV reactivation also need to be evaluated, also for the observation that CD4+:CD8+ ratio below 0.6 is a risk indicator. If the immune changes detailed here are confirmed in larger patient series, they may have important potential as early immune markers that will allow preemptive antiviral therapy of HCMV infection in high-risk patients.
Footnotes
Acknowledgments
The authors are thankful to Dr. Mikkel Steen Petersen and DMSc. Bent Deleuran for critical reading of the manuscript. We are grateful to The Karen Elise Jensen Foundation; the Max and Inger Wørzner's Foundation; the Frits, Georg, and Marie Cecilie Glud's Foundation; and the Harboe Foundation, for financially supporting this study.
Author Disclosure Statement
No competing financial interests exist.