
Abstract
Enterovirus infections may be involved in the etiology of type 1 diabetes (T1D), which is strongly associated with certain human leukocyte antigen (HLA) class II haplotypes. Our aim was to assess whether HLA genotypes conferring varying degrees of risk for T1D were associated with enterovirus gut infections. From the general Norwegian population, 190 healthy infants at high-risk for T1D (DR4-DQ8/DR3-DQ2), and 383 infants without this genotype were identified. Non-DR4-DQ8/DR3-DQ2 genotypes were further categorized as conferring either an increased-to-moderate risk (DR4-DQ8 or DR3-DQ2), were protective (DQB1*06:02), or were neutral (all other genotypes). A total of 4626 monthly fecal samples taken between age 3 and 12 mo were tested for enterovirus RNA using real-time PCR. Enterovirus prevalence was 11.5% among high-risk children, and 12.2% in other children (adjusted odds ratio: 1.23, p=0.12). The prevalence was 11.3% in those with increased-to-moderate risk, 13.0% in the protective group, and 12.6% in the neutral group (likelihood ratio test, 3 d.f.: p=0.37). In conclusion, there was no statistically significant association between HLA genotype and the occurrence of human enterovirus gut infections.
Introduction
Type 1 diabetes (T1D) is a polygenic multifactorial disease, and susceptibility is mostly conferred by particular haplotypes of human leukocyte antigen (HLA)-DRB1, -DQA1 and -DQB1 (4), with contributions from certain DRB1*04 subtypes (5,6). Despite the fact that enteroviral infections are usually asymptomatic and self-limiting (7), they are considered possible environmental triggers or accelerators of islet autoimmunity (8,9). Nevertheless, the potential pathogenic mechanism is not known, as is whether a specific enterovirus serotype or sequence motif is responsible for any possible diabetogenic effect. Data from murine models of diabetes autoimmunity suggest that host genetics influence beta-cell damage and diabetes after viral infection (10 –12). Genes within the HLA region are candidate genes for modifying the likelihood or course of viral infection and disease. For instance, HLA has been associated with dengue, hepatitis C, HIV, and Hantaan virus infection (13). It has been speculated that the observed association between enterovirus infection and T1D may be explained by HLA genotype (14). With a few exceptions, studies investigating whether T1D-associated HLA genotypes may modify susceptibility to enterovirus infections have been limited in size, have investigated only patients (not controls), were limited to enterovirus serology, and the results have been inconsistent (15 –24).
The objective of the current study was to test whether the frequency of enterovirus in serial fecal samples from healthy infants differs according to HLA genotypes previously established to confer varying degrees of risk for T1D.
Materials and Methods
Study population
This study involved children participating in the Norwegian prospective cohort study entitled “Environmental Triggers of Type 1 Diabetes: The MIDIA study” (2001–2007) (25). MIDIA tested 46,939 newborns from the general population, which identified the 2.1% of Caucasians carrying the heterozygous HLA-DRB1*04:01-DQA1*03-DQB1*03:02/DRB1*03-DQA1*05-DQB1*02 genotype (often referred to as DR4-DQ8/DR3-DQ2), which confers the highest risk for T1D. This genotype is associated with a 5–10% risk of a T1D diagnosis by the age of 15 y in populations of European origin. From May 2004 to June 2006 the study also recruited a “control cohort” from the general population with HLA genotypes other than DR4-DQ8/DR3-DQ2, on average approximately twice as many children with these other genotypes (the ratio varied slightly during the recruitment period). Children with and without the high-risk genotype were followed in the same manner with monthly fecal samples for viral analysis. The present analysis is based on 4626 fecal samples collected at age 3–12 mo from 190 children with the HLA-DR4-DQ8/DR3-DQ2 genotype, and 383 children without this genotype (Fig. 1). Written informed consent was provided by participating families. The study was approved by The Regional Committee for Medical Research Ethics and the Norwegian Data Inspectorate.
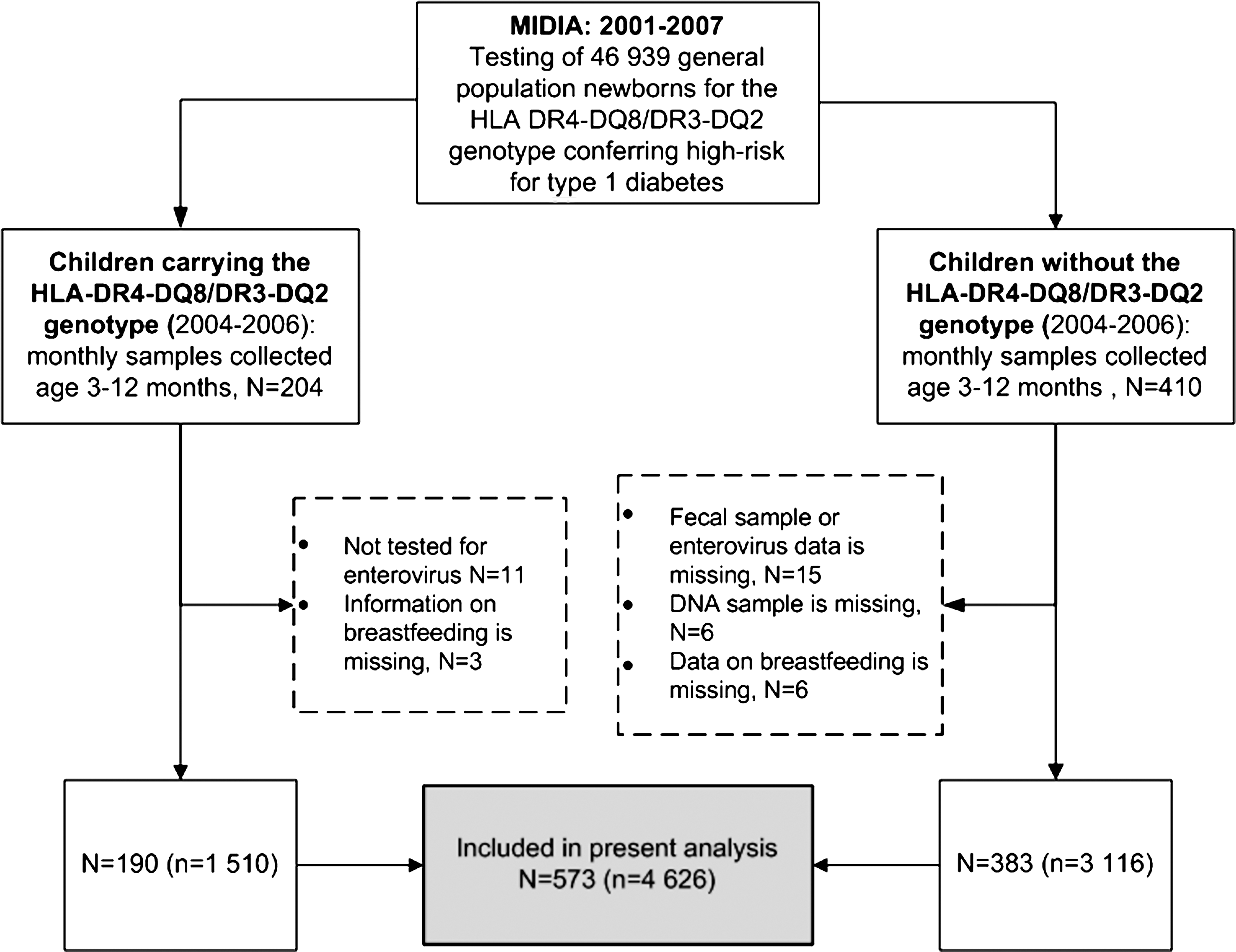
Flow chart illustrating the details of the study's children and their sampling procedure (N, number of children' n, number of fecal samples; MIDIA, Environmental Triggers of Type 1 Diabetes: The MIDIA study).
Detection of enterovirus RNA in fecal samples
Fecal samples were collected, processed, and tested for enterovirus RNA using internally controlled quantitative reverse transcriptase PCR as previously described (7).
HLA typing and grouping
HLA genotyping for identification of high-risk T1D alleles has been described previously (25). Briefly, DQA1 was typed for five broad specificities (DQA1*01, *02, *03, *04, and *05), while only alleles associated with significant T1D risk or protection were included for DQB1 typing (DQB1*02, *03:01, *03:02, *03:03, *03:04, *04:02, *06:02, and *06:03). HLA-DRB1*04 was typed for eight subtypes. Sequences and protocols for the detection of allele-specific PCR products are available from the authors on request.
The children were categorized into four broad HLA risk genotype groups as determined by the odds for developing T1D found in previous studies (4,26 –29). The high-risk genotype was DR4-DQ8/DR3-DQ2. Increased-to-moderate risk genotypes were DQ8/DQ8, DQ8/X, DQ2/DQ2, and DQ2/X (X≠DQB1*06:02). The protective genotype was at least one DQB1*06:02 allele. All other genotypes were classified as neutral or low risk. Furthermore, 11 children who carried DR4-DQ8/DR3-DQ2 with DR4 subtypes other than DRB1*04:01 were excluded from the analyses for the sake of consistency.
Statistical analysis
Association analyses were performed using logistic regression models, with enterovirus infection (yes or no) as the response, HLA genotype (group) and other variables as covariates, and a random intercept to account for potential intra-individual correlation of infections, using STATA version 11 (StataCorp, College Station, TX). Information on breastfeeding and other variables were collected using structured questionnaires completed by the parents when the infants were 3, 6, 9, and 12 mo of age. We adjusted for age, sex, calendar year, season of sample collection, the number of full siblings, and total breastfeedings reported every month, as previously described (3). In accordance with this previous analysis, we included an interaction term in the model to account for the fact that the association between breastfeeding and enterovirus differed by age.
Finally, we conducted sensitivity analyses, for which the main analyses were repeated after restricting to (1) infections with high quantities of enterovirus RNA (defined as higher than the median quantity, 10,000 copies per μL, among positive samples), and (2) infectious episodes (counting only the first enterovirus RNA-positive sample in a series of two or more consecutively positive samples), and (3) prolonged infection episodes (at least two consecutive monthly samples positive for enterovirus RNA).
Results
The summary characteristics of subjects and their samples are shown in Table 1. There were few differences between the groups with and without the high-risk HLA-DR4-DQ8/DR3-DQ2 genotype for T1D, except a slight variation in the season of the samples, which may involve varying ratios of children in the two groups recruited over time. The prevalence of enterovirus infections increased linearly from ages 3 to 12 mo, and varied by season, similarly for children with and without the DR4-DQ8/DR3-DQ2 genotype (Fig. 2).
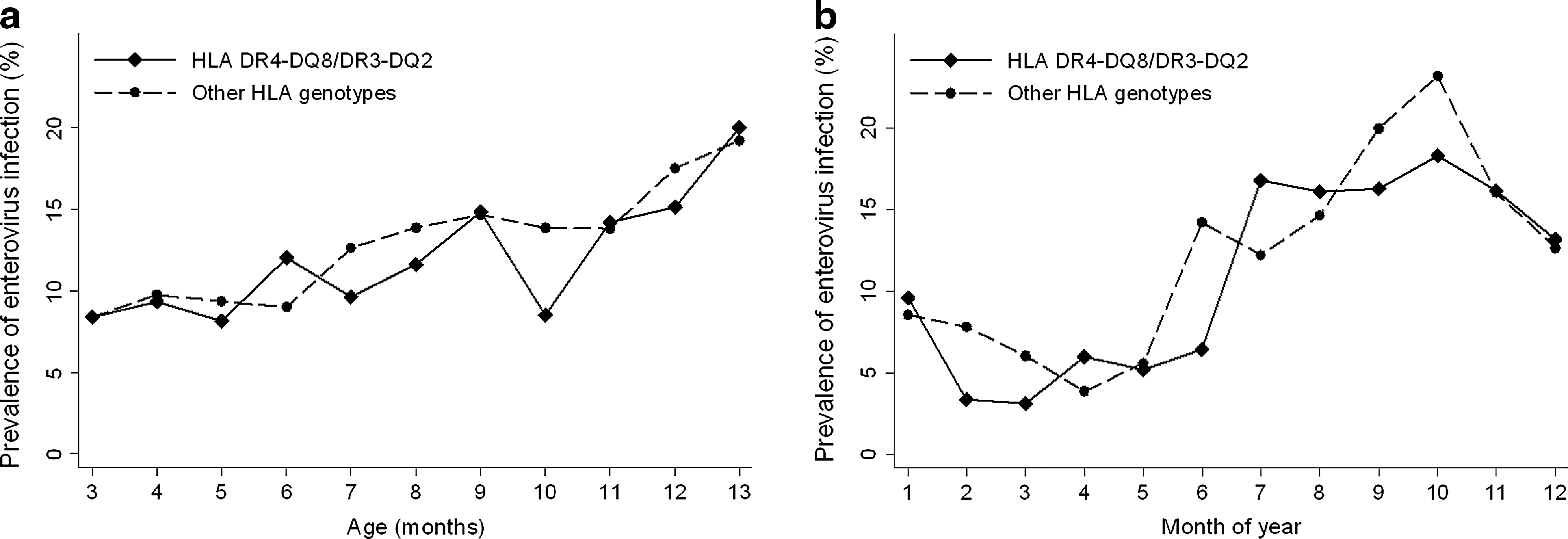
Frequency (%) of enterovirus-positive fecal samples in children with and without the DR4-DQ8/DR3-DQ2 genotype, according to age (
DRB1*04:01-DQA1*03-DQB1*03:02/DRB1*03-DQA1*05-DQB1*02.
The observed prevalence of enterovirus was slightly lower among those with the DR4-DQ8/DR3-DQ2 genotype (11.5%) than for the other genotypes, with the highest observed prevalence among the T1D-protective genotype (13.0%), but the difference was not statistically significant (Table 2). The frequency of enterovirus RNA-positive fecal samples was similar in children carrying at least one DR4-DQ8 haplotype and those carrying at least one DR3-DQ2 haplotype (Table 2). (Associations with enterovirus for the other variables used in the adjusted analysis in Table 2 are shown in Supplementary Table S1; see online supplementary material at
OR was mutually adjusted for the covariates listed in Supplementary Table 1 previously found to predict enterovirus frequency (3), and calendar year.
High-risk: DR4-DQ8/DR3-DQ2=DRB1*04:01-DQA1*03-DQB1*03:02/DRB1*03-DQA1*05-DQB1*02; Non high-risk=other DR-DQ genotypes than the high-risk genotype; Increased-to-moderate risk=DR4-DQ8 homo- or heterozygotes and DR3-DQ2 homo- or heterozygotes; Protective=carrying at least one DQB1*06:02 allele; Neutral=all other genotypes.
Likelihood-ratio (LR) test (3 d.f.): testing the model assumption of the HLA categorical variable (4 categories).
LR test (1 d.f.): testing the model assumption of the HLA high-risk/non-high-risk variable (2 categories). Even after testing for a trend over HLA genotypes assuming an increasing risk for infection with decreasing risk for type 1 diabetes, there was no significant association between HLA and enterovirus prevalence (LR test, 1 d.f.: p=0.15).
LR test (1 d.f.).
OR, odds ratio; CI, confidence interval.
Discussion
To our knowledge, the current study involving testing of more than 4500 fecal samples from 573 children is the largest of its kind. Although there were some suggestive trends, we did not find any statistically significant association between HLA genotypes conferring varying degrees of risk for T1D and the frequency of gut infections with enterovirus in healthy infants. Previously, we suggested a slightly lower enterovirus frequency in those with the DR4-DQ8/DR3-DQ2 genotype than in children without this genotype (3), although HLA genotype was not the major predictor of interest, and therefore appropriate measures such as restriction to comparable dates of birth (and hence dates of enrollment) and age of follow-up in the two HLA groups of children were not taken. After having tested additional samples for enterovirus, restricting to comparable dates of birth and age of follow-up for the groups, as well as further genotyping of non-DR4-DQ8/DR3-DQ2 children in the current study, it seems that our previous finding may have been at least partially biased (3).
It has been speculated that the possible relation between enterovirus and T1D may be confounded by associations or interactions with HLA genotype (14). In addition to general importance for enterovirus epidemiology and immunity, this would have a great impact on the interpretation of studies of enterovirus and T1D (8,9). Most previous studies in the field have been relatively small and limited to serologic testing of enterovirus in patients with T1D (16 –18). One relatively large study found that T1D patients who had the DR3-DQ2 haplotype were less likely to have enterovirus RNA in their blood and/or fecal samples compared to those with other DQB1 genotypes, but the association was not consistent over ethnic groups (15). It should be noted that an observed association between host genotype and enterovirus among patients with T1D could be explained either by a similar association in the general population, or an interaction between enterovirus and HLA in the general population such that the association between enterovirus and T1D differs by HLA genotype (30). It is therefore necessary to assess the potential association between HLA genotype and enterovirus infection among healthy subjects (representative of the general population), not only in patients with T1D.
We are not aware of any previous large scale study in which the association between HLA genotype and frequency of enterovirus RNA has been tested in healthy children. We are aware of two studies of the association between HLA genotype and frequency of anti-enterovirus antibodies, one of which is unpublished (see below). In the Finnish DiMe study of siblings of patients with type 1 diabetes, children who according to serological HLA typing carried HLA-DR3 and/or HLA-DR4 had higher levels of anti-enterovirus antibodies than those with HLA-DR2 (19). Unpublished results from DAISY in Colorado (31) showed that children with high- or moderate-risk HLA genotypes had significantly higher IgM levels for some enterovirus serotypes (coxsackie B1, echo 11, and coxsackie A9), compared to other or low-risk HLA genotypes (M. Rewers, personal communication). This may consequently result in a lower frequency of infection and/or virus quantity for children with HLA T1D-associated haplotypes.
In contrast to our findings, in a recent Finnish article including children positive for T1D-associated autoantibodies (who eventually developed T1D), and matched autoantibody-negative controls, more samples were enterovirus RNA-positive with the high-risk HLA-DR4-DQ8/DR3-DQ2 genotype than in children who carried moderate-risk genotypes with the DR4-DQ8 haplotype (23). However, studies of other cohorts of healthy children with HLA genetic susceptibility toward T1D screened for the development of islet autoantibodies have not found any consistent association between HLA genotypes conferring varying degrees of risk for T1D and enterovirus infections as defined by serology or the presence of enterovirus RNA in serum or fecal samples (20 –22,24). It should be noted that many of these studies have been small or of moderate size compared to ours.
Limitations
Among the limitations of the current study are the lack of control of past immunity acquired from maternal antibodies and infections occurring before 3 mo of age, and a lack of characterization of the enterovirus serotype present in the positive samples, which has also not been done in other studies. However, to be able to study enterovirus serotype separately with sufficient statistical power will require much larger sample sizes due to the large number of serotypes.
Similarly, we did not attempt to test for all possible alleles within the HLA complex, as most of them are not relevant to diabetes risk, but we focused our study on predefined groups according to the degree of predisposition for T1D. As enteroviruses are shed in feces for weeks after an infection, we likely to detected the majority of enterovirus infections, but we cannot exclude the possibility that a different effect may be seen for virus infections in the blood and those in other organs (i.e., different HLA genotypes may have a different immune response [weaker or stronger]), and therefore in some individuals infections may be more invasive and symptoms more severe.
Potential explanations for our results
Another factor that may be relevant to our results is that T-cell-mediated immune responses probed by viral antigens presented by HLA class II molecules may be weaker in very young children than in older children, who have developed stronger adaptive immune responses (32). While the associations of HLA with autoimmune disease have been strong and well acknowledged (33), there have been few studies finding significant evidence for an association between HLA polymorphisms and infectious diseases, possibly due to a lack of statistical power (34). Although the present study included the largest dataset examined to date of HLA associations with enterovirus RNA, we cannot exclude a weak effect of HLA genotype.
In conclusion, our study did not show any significant association in healthy infants between HLA genotypes known to confer varying degrees of risk for T1D, and the frequency of gut infections with enterovirus.
Footnotes
Acknowledgments
We thank the public health care nurses, in particular Turid Wetlesen and Lene Gustavsen, for their effort in the recruitment to the MIDIA study and follow-up of participating families. The staff at the Biobank, Norwegian Institute of Public Health, helped with sample registration and initial handling. We also thank Prof. Marian Rewers, Barbara Davis Center for Childhood Diabetes, University of Colorado School of Medicine, for access to unpublished results from DAISY. Last, but not least, we express our deepest gratitude to all the families for participating in this study.
This study and the MIDIA project were funded by the Norwegian Organization for Health and Rehabilitation (2008/0182), the Ministry of Health of the Czech Republic (IGA MZ 11465-5), the Research Council of Norway (grants 135893/330, 155300/320, 156477/730, and 166515/V50), the Norwegian Diabetes Association, and Sigurd K. Thoresen's Legacy. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.