
Abstract
Dengue fever (DF) is often asymptomatic in endemic areas. Asymptomatic infection during a DF outbreak in China, where DF is not endemic, has not been reported until now. In this study a total of 365 subjects from 6 villages were recruited from October 4–7, 2009. Overall, 102 subjects (27.95%) were positive for dengue virus (DENV) IgM, and 14 subjects (3.84%) were positive for DENV IgG and IgM. In different age groups, seropositive rates varied from 12.50% to 50.00% for DENV IgM, and from 0% to 11.76% for DENV IgG. Seroprevalence of DENV IgM was significantly higher than that of DENV IgG. Seroprevalence rates of DENV IgM differed among different villages. However, the seroprevalence of DENV IgM was not statistically significantly different among gender and age groups. Asymptomatic DF infection is prevalent in non-endemic areas.
Introduction
DENV-3 subtype III has been continuously circulating in the Indian subcontinent from the 1960s to the present. The virus was first isolated in East Africa in 1985 in Mozambique, and subsequently from Kenya (1991) and Somalia (1993) (8,14). DENV-3 subtype III was first detected in the American continent in 1994 (Nicaragua and Panama), and the virus has subsequently spread through most of Latin America (3,6,9,12,19).
In 2009, an outbreak of DENV-3 subtype III took place in Yiwu (a central city of Zhejiang Province in Southeastern China), where DF was not endemic (13). One hundred and ninety-six symptomatic cases of DF were identified and no DHF or DSS cases were seen. The date of symptom onset among confirmed or clinically-diagnosed cases ranged from July 20 to October 4. The number of cases peaked in early September and subsided in early October. However, as DENV infection in humans causes a spectrum of illnesses ranging from inapparent or mild febrile illness to severe and fatal hemorrhagic disease, the actual infection rate is unknown during an outbreak in non-endemic areas. This study aimed to investigate the seroprevalence of DENV IgM and IgG in subjects with DF, and to explore the risk factors of inapparent infection.
Materials and Methods
Blood samples
Blood samples were collected between 4 and 7 October, 2009 from subjects in six villages where DF cases were reported, and demographic data information were collected, including age, gender, and place of residence. After collection, the blood samples were kept at 4°C in an ice chest for less than 2 h before transport to the laboratory. All the sera were then centrifuged, decanted, and stored at −80°C until testing.
The experimental research reported in this study was approved by the ethics committee of Zhejiang Provincial Center for Disease Control and Prevention. Human research was carried out in compliance with the Helsinki Declaration. The aims of our study were explained to all participants upon enrollment, and written consent was obtained from all participants. For children, consent from the parent or guardian was also obtained.
Serological testing
Samples were tested for DENV IgM antibodies and DENV IgG antibodies using ELISA tests (Panbio, Brisbane, Queensland, Australia). False-positive results with other flaviviruses, particularly with the IgM ELISA, may occur, but according to manufacturer's guidelines the serological sensitivity and specificity of ELISA testing for anti-DENV IgM are 94.7% and 100%, respectively, and the ELISA for anti-DENV IgG has a sensitivity of 95.4% and a specificity of 100%. They collected 57 samples from patients with primary dengue infection, 83 endemic seronegative samples, and 115 samples from patients with secondary dengue infection. The Panbio ELISA results were compared with the dengue status of the sera to determine the sensitivity and specificity of the assay relative to dengue serological status. Anti-DENV IgM>11 Panbio units, and anti-DENV IgG>11 Panbio units, were considered to be indicative of infection.
Data analysis
Data for DENV seroprevalence among villages, gender, age groups, and numbers of reported cases were analyzed. Chi-square testing, Kendall correlation, and conditional logistic regression analysis, were conducted using SPPS version 13.0 statistical software (Chicago, IL). For the conditional logistic regression (forward), serological status was assigned as a dependent variable, while village, gender, age, number of reported cases, and village×number of reported cases were entered as independent variables. The stepwise probability was set to 0.05 for entry and 0.10 for removal. The classification cutoff was 0.5, and the maximum number of iterations was 20. Omnibus tests of model coefficients were also conducted.
Results
A total of 365 human sera were collected from subjects in six villages (Beiyuan, Chongshan, Qianwang, Fuzhai, Qingsu, and Xiateng). One hundred and seventy-two cases were reported in Qingsu, and in several persons who lived in the villages of Beiyuan (1 case), Chongshan (2 cases), Qianwang (4 cases), Fuzhai (3 cases), and Xiateng (4 cases; Fig. 1). Of these, 160 were male and 205 were female, which were divided into 9 age groups (Table 1). Overall, 102 subjects (27.95%) tested positive for DENV IgM, and 14 (3.84%) were positive for DENV IgG (Table 2). All 14 IgG-positive subjects were also IgM-positive. Seropositive rates of the different age groups varied from 12.50% to 50.00% for DENV IgM, and ranged from 0% to 11.76% for DENV IgG as shown in Table 3.
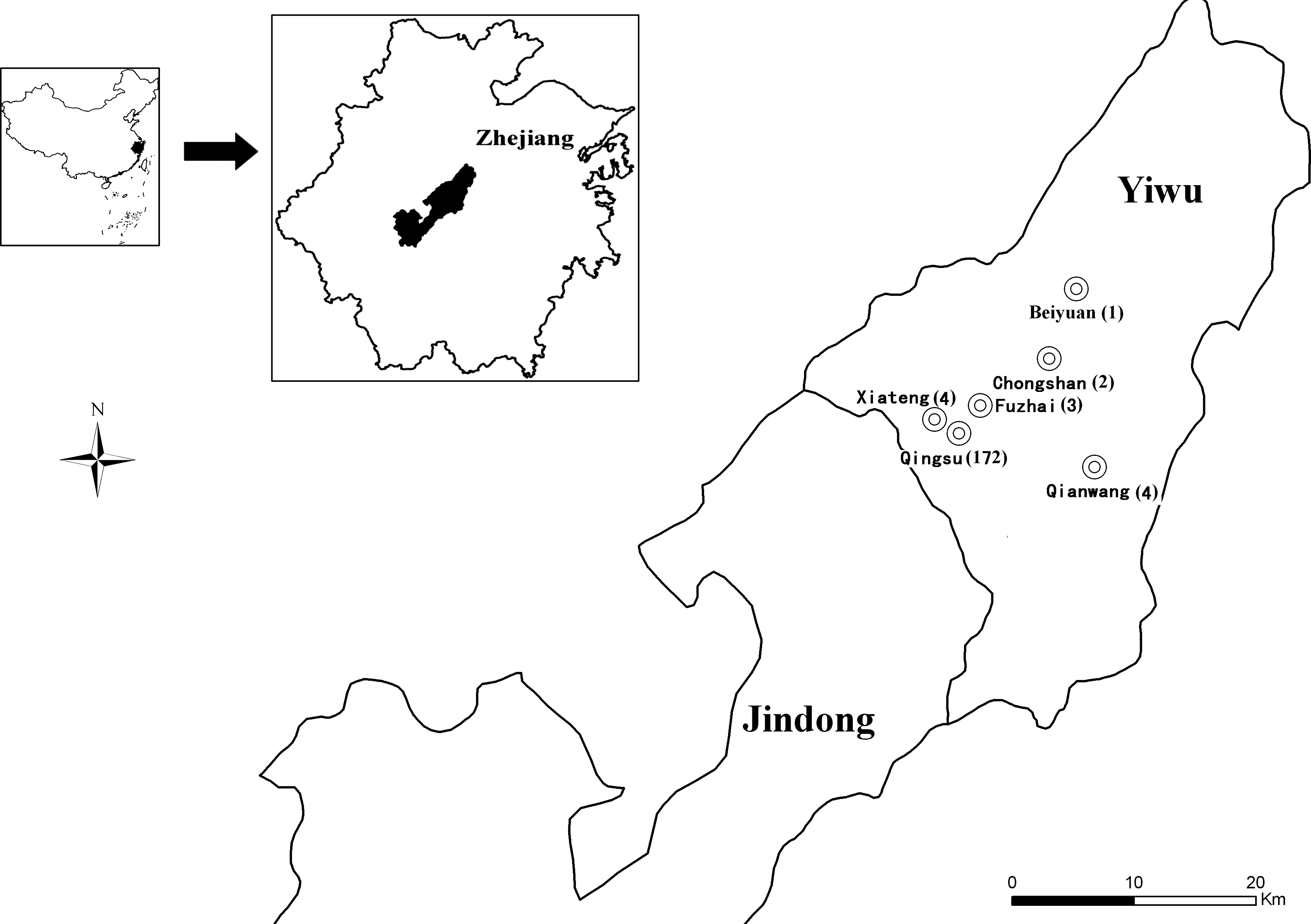
Geographic locations of the six villages where the blood samples were collected.
Of note, seroprevalence of DENV IgM was significantly higher than that of DENV IgG (chi-square 84.202, p=0.000). The seroprevalence of DENV IgM varied significantly among the different villages (0–47.62%; chi-square 19.594, p=0.001). But seroprevalence of DENV IgM was found no statistical difference between males (29.38%) and females (26.83%, chi-square 0.289, p=0.591), and among different age groups (chi-square 12.968, p=0.113). The result of Kendall correlation analysis suggested no significant correlation between the infection rate and the number of reported cases (tau-b=0.414, p=0.251).
The chi-square value in omnibus tests of model coefficients was 3.896 (p<0.05). Furthermore, the overall correct percentage was found to be 72.1%. The variable in the equation was village×number of reported cases. The Wald equation result was 54.826 (p=0.000).
Discussion
Travelers play an essential role in the global epidemiology of dengue virus infections, as viremic travelers carry various DENV serotypes and strains into areas with mosquitoes that can transmit infection (5). Zhejiang Province is a developed region of great economic importance for industry and tourism. Millions of tourists and businessmen from India, Malaysia, Thailand, and other endemic countries for dengue fever come to Zhejiang Province every year. What's more, Zhejiang Province has a humid subtropical climate influenced by the Asian monsoon, with high temperatures and humidity, a climate suitable for the survival of mosquitoes and DENV. Thus far, Aedes aegypti has not been found in Zhejiang Province, but the density of Aedes albopictus was high according to our surveillance, and was considered the primary vector of DF in Zhejiang Province (18). A. albopictus particularly bites in forests during the daytime, and has been known as the forest day mosquito for this very reason. Depending upon the region and biotype, there are differing active peaks, but for the most part they rest during the morning and nighttime hours. They search for their hosts inside and outside of human dwellings, but are particularly active outside. They bite multiple hosts during their development cycle, making them particularly efficient at transmitting diseases.
During this outbreak, Culex pipiens pallens and A. albopictus were the dominant species, clearly outnumbering Anopheles sinensis, Armigeres obturbans, and other minor species. The density of A. albopictus was about 52/h. The Breteau Index (BI), house index (HI), and container index (CI) were 96.10, 73.27, and 42.82, respectively, before the introduction of control measures on September 10. The density of A. albopictus larvae sharply declined, and the BI of all villages in Yiwu stabilized below 5% after October 4.
This outbreak of DF occurred in Zhejiang Province, but DF is not endemic in Zhejiang Province, and all outbreaks were triggered by imported cases. Although researchers reported that DF was often asymptomatic or caused a non-specific febrile illness in endemic areas (10), and the seroprevalence of DENV-specific antibodies was high in areas where dengue infection was sporadic (4), there had been no efforts to explore occult infection during an outbreak in China. Investigation of occult infection is important for DF prevention and control, especially for the prevention of DHF and DSS. Thus it is important to study the actual infection rate during an outbreak in a non-endemic country and explore the risk factors.
When dengue infection occurs in persons who have not previously been infected by a flavivirus or immunized with a flavivirus vaccine, they develop a primary antibody response characterized by a slow increase in specific antibodies. IgM antibodies are the first immunoglobulin isotype to appear. These antibodies are detectable in 50% of patients by days 3–5 after the onset of illness, increasing to 80% by day 5, and 99% by day 10. IgM levels peak about 2 wk after the onset of symptoms, and then decline to undetectable levels over 2–3 mo. Anti-dengue serum IgG is generally detectable at low titers at the end of the first week of illness, increasing slowly thereafter, with serum IgG still detectable after several months, and probably even for life (11,16,20). In this study, the seroprevalence of DENV IgM among people who had no clinical manifestations was 27.95%, indicating that 27.95% of them had been infected by DENV at least 3 days before serum collection. The seroprevalence was much lower than the percentage reported in Malaysia (53.57%), probably because their samples were all from patient household members. However, it was significantly higher than that reported in Thailand (8.8%) (17). We speculated that the seroprevalence rate may correlate with the outbreak level. Furthermore, the fact that the seroprevalence of DENV IgG was only 3.84%, and all these serum samples were also positive for IgM, demonstrated that DENV was not endemic in Zhejiang Province, and those infected had been so no longer than 3 mo. The result that the seroprevalence of DENV IgM was significantly higher than that of IgG indicated that these people were infected recently. Thus they were all apparently infected during the DENV-3 outbreak.
DENV IgM was not detected in Beiyuan. This may be due to the small sample size, or because the single case was imported from another village. Of interest, the seroprevalence of IgM varied significantly among villages. It was significantly higher in Fuzhai and Qingsu than in the other villages. The reasons may be that there were more cases in these two villages, and because the cases were reported earlier. To our surprise, the infection rate was not correlated with number of reported cases, according to our data.
Children and adolescents were recognized as the primary victims of dengue infection in endemic areas (15), but we found the lowest infection rate among persons under 10 y of age. This confirmed that DF was not endemic in Zhejiang Province, and that background immunity for DENV infection was virtually absent. Because there is only one child in every family in China, they are cared for better than adults. As a result, they had less exposure to mosquitoes and lower infection rates. In the logistic regression analysis, only village×number of reported cases remained in the final model, indicating that village and number of reported cases correlated with each other. Also, inapparent infection rates were higher in villages where more DF cases were reported.
To our knowledge, this is the first report of inapparent infection during a DF outbreak in China. This study provides valuable insights into DF transmission in a non-endemic country like China. Some people were unaffected, even though they had been infected with dengue viruses. However, these people may carry DENV and transmit it to mosquitoes, which play a substantial role in the transmission of DF. We should pay more attention to inapparent infection in order to control DF. Our results indicate that many more people were infected than were reported during this outbreak, especially in areas where more cases were reported, and the risk of DHF/DSS is higher if different dengue serotypes are imported.
Footnotes
Acknowledgments
We thank the Yiwu Community Health Centers, the Yiwu Department of Health Service, and the Yiwu Center for Disease Control and Prevention in Zhejiang, China, for their support and assistance with this investigation.
Author Disclosure Statement
No competing financial interests exist.