
Abstract
Chronic hepatitis B (CHB) is a worldwide infectious disease caused by hepatitis B virus (HBV). HBV mainly damages liver cells through immune response. The purpose of this study was to determine whether there were dynamic changes of Treg and Th17 cells and to judge the value of these indicators to antiviral treatment. Twenty-two CHB patients and selected 30 healthy adults were enrolled. Results showed that the expression of Treg (5.72±0.46 vs. 4.42±0.17, p=0.0019) and Th17 (3.94±0.64 vs. 2.66±3.12, p=0.0436) cells was significantly increased in CHB patients, as well as the level of interleukin-17 (IL-17) (16.88±5.37 vs. 8.59±3.31; p=0.004). Then, we monitored longitudinally the impact of the treatment with interferon-α and found that the suppression of viral replication induced by interferon-α resulted in a decrease in Treg, Th17 cells, and IL-17; we also found that the percentage of Treg and Th17 cells went up without clear evidence of clinical autoimmune disease at the end of treatment. Thus, Treg and Th17 cells might play an important role in interferon-α treatment to eliminate HBV. The level of changes may be served to determine the antiviral efficacy of interferon-α therapy.
Introduction
C
Increasing evidence demonstrated that HBV mainly damages liver cells through immune response. HBV infection can cause cellular and humoral immune response, stimulate autoimmune response and immune dysfunction, and lead to the imbalance in the ratio of T helper cells, Th1/Th2 (3,7,22,23). Interferon-α (IFN-α) is widely used for it had the effect of both anti-HBV and immunoregulation dual functions in the past decade (2,5). However, the mechanism of interferon-α is not completely clear.
Previous studies showed that the balance of regulatory T (Treg) cells and interleukin (IL)-17+ T helper (Th17) cells also changed in those patients with chronic HBV infection (9,10), and antiviral treatment like NA therapy may rectify it (8,13,28 –30), but there was no study to reveal the changes of Treg and Th17 cells through interferon-α therapy.
Therefore, we studied the expression of Treg and Th17 cells in CHB patients using interferon-α therapy; the purpose of this study was to determine whether there were dynamic changes of Treg and Th17 cells and to judge the value of these indicators to antiviral treatment.
Materials and Methods
Patients
From May 2012 to July 2013, consecutive 30 CHB patients at the Nanjing Jiangbei People's Hospital were prospectively enrolled. All patients were positive for serum HBsAg for >24 weeks and had elevated serum HBV-DNA of >20,000 IU/mL and alanine aminotransferase (ALT) between 80 and 400 U/L (2–10 ULN). The exclusion criteria included the following: (i) use of antiviral or immunomodulating treatment in the past 6 months, (ii) positive pregnancy test in females, (iii) alcoholic liver disease, (iv) radiological evidence of cirrhosis or hepatocellular carcinoma, (v) with hepatitis C virus, hepatitis D virus, or human immunodeficiency virus coinfection, and (vi) accompaniment of diabetes, thyroid dysfunction, autoimmune diseases, and psychological issues. Thirty healthy individuals were enrolled as normal control (control group).
After the enrollment, all patients were subcutaneously administered with interferon α-1b (recombinant human interferon α-1b for injection, CHN; Shenzhen Kexing Biotech Co., Shenzhen, China) 5 MIU every other day. The observation lasted for 48 weeks. All subjects accepted physical examination and serum analysis at week 0, 12, 24, and 48.
The study protocol was approved and monitored by the Ethics Committee of Nanjing Jiangbei Peoples' Hospital, and written informed consent was obtained from the patients.
Flow cytometric analysis
The HU FOXP3 STANG KIT, HU TH1/17 PHNOTYP KIT, and IL-17A KIT were purchased from BD Pharmingen (San Diego, CA). We defined the Treg cells as the population of CD4+CD25+FoxP3+T cells taken from the percentage of total CD4+T cells and defined the Th17 cells as the population of CD4+IL-17A+T cells taken from the percentage of total CD4+T cells. Whole blood from each patient was collected in the heparin anticoagulated Vacutainer tube for Th17 and Treg cell detection and the Vacutainer tube for IL-17A detection. Samples were stained and fixed within the day of collection. To detect Th17 cells, fresh blood (200 μL) was incubated with phorbol 12-myristate 13-acetate (50 ng/mL) and ionomycin (1 mg/mL) in 200 μL RPMI 1640 medium supplemented with 10% fetal calf serum for 4 h. After using BD Cytofix and Perm for 30 min, it was mixed with Th1/Th17 Phenotyping Cocktail (10 μL) for 30 min. To test Treg cells, a sample (200 μL) was first stained with CD4 FITC (20 μL) and CD25 APC (20 μL) for 30 min, fixed with Buffer A (2 mL) for 10 min, washed with a Pharmingen stain buffer, permeabilized cells by Buffer C (0.5 mL) for 30 min, and then FOXP3 phycoerythrin (PE) (10 μL) was added for 30 min; all steps were protected from light. To detect IL-17A, first put IL-17A (13 μL) capture beads and wash buffer (800 μL) into mixing pipe, centrifuged for 5 minutes and removed the supernatant. Second, diluted by 50 μl capture beads diluent, mixed and in dark for 15 minutes, then added serum samples 50 μl continued mix and in dark for 1 hour. The next step added 50 μL detection (1 μL PE detection and 49 μL PE detection diluent) to the pipe, mixed and in dark for 2 h, at last used 500 μL wash buffer and centrifuged 5 min for removing the supernatant and then tested on the flow cytometry at speed of 50 cells/sec. All specimens were tested on the flow cytometry within 3 h. Three-color flow cytometric analyses were performed using FACSCalibur, CellQuest, and FCAP software (Becton Dickinson, San Jose, CA).
HBV-DNA assessment
HBV-DNA levels were determined by real-time polymerase chain reaction (Roche, Pleasanton, CA). The threshold of the HBV-DNA detection limit was 250 IU/mL.
Statistical analysis
Results are reported as mean±standard deviation for percentages. Statistical comparisons between two groups used the independent samples t-test. The one-way ANOVA and Scheffe's methods were used for multiple comparisons. Data analysis was done using SPSS version 13.0 for Windows and the confidence interval was 95% or the p-value<0.05, as there was a significant difference.
Results
Characteristics of CHB patients receiving IFN-α therapy
Treg and Th17 cells were increased in CHB patients compared with control. Twenty-two (73.3%) patients completed the full course of therapy, while 2 (6.7%) patients discontinued treatment due to intolerance and 6 (20%) patients had no response at week 12 and then changed to use NA therapy. Baseline characteristics of patients and healthy individuals are summarized in Table 1.
Treg, Th17, and Th1 cell frequencies are represented in percentage; the levels of cytokines are represented with pg/mL. Data are shown as mean±standard deviation.
p<0.05.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CHB, chronic hepatitis B; HBeAg, hepatitis B e antigen; HBV, hepatitis B virus; IL-17, interleukin-17; SD, standard deviation.
Treg and Th17 cells were significantly increased in CHB patients
We found that there was a significantly higher frequency of Treg cells in CHB patients (5.72±0.46) compared with healthy subjects (4.42±0.17, p=0.0019) (Fig. 1A and Table 2). The frequency of Th17 cells went up in CHB patients and also had a significant difference to the control (3.94±0.64 vs. 2.66±3.12, p=0.0436) (Fig. 1B and Table 2).
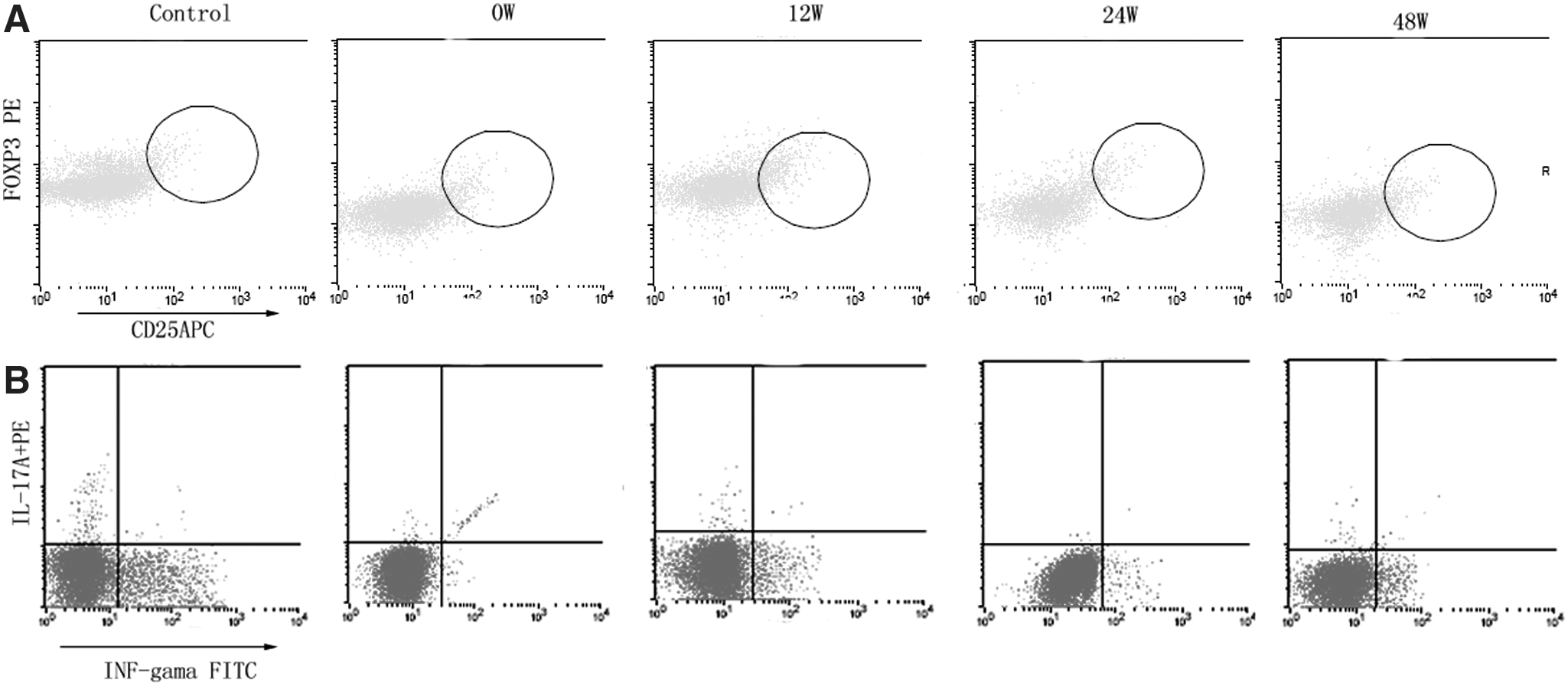
Treg and Th17 cells were significantly increased in CHB patients. The expression of Treg
Treg, Th17, and Th1 cell frequencies are represented in percentage; the levels of cytokines are represented with pg/mL. Data are shown as mean±standard deviation.
Levels of HBV-DNA, ALT, aspartate aminotransferase, and lymphocyte count decreased during interferon-α treatment
During interferon-α treatment, we determined the levels of serum HBV-DNA, ALT level, aspartate aminotransferase (AST), and lymphocyte count at the baseline at 12, 24, and 48 weeks. The HBV replication was considerably lower than that at baseline in all patients; the level of HBV-DNA was reduced from 5.58±1.96 log10 IU/mL to 0.71±1.22 log10 IU/mL at week 48 (Table 2 and Fig. 2A) and this decrease was paralleled in the serum ALT (from 187.5±128.2 to 27.53±4.08 U/L) and serum AST levels (from 99.6±74.1 to 26.48±4.07 U/L) (Table 2 and Fig. 2B, C). However, at the level of lymphocyte (× 109/L), it was decreased from 2.22±0.41 at baseline to 1.51±0.46 at week 24 and then up to 1.73±0.39 at the end of therapy (Table 2 and Fig. 2D); we considered that the lymphocyte count was decreased by interferon-α at first and then tolerated.
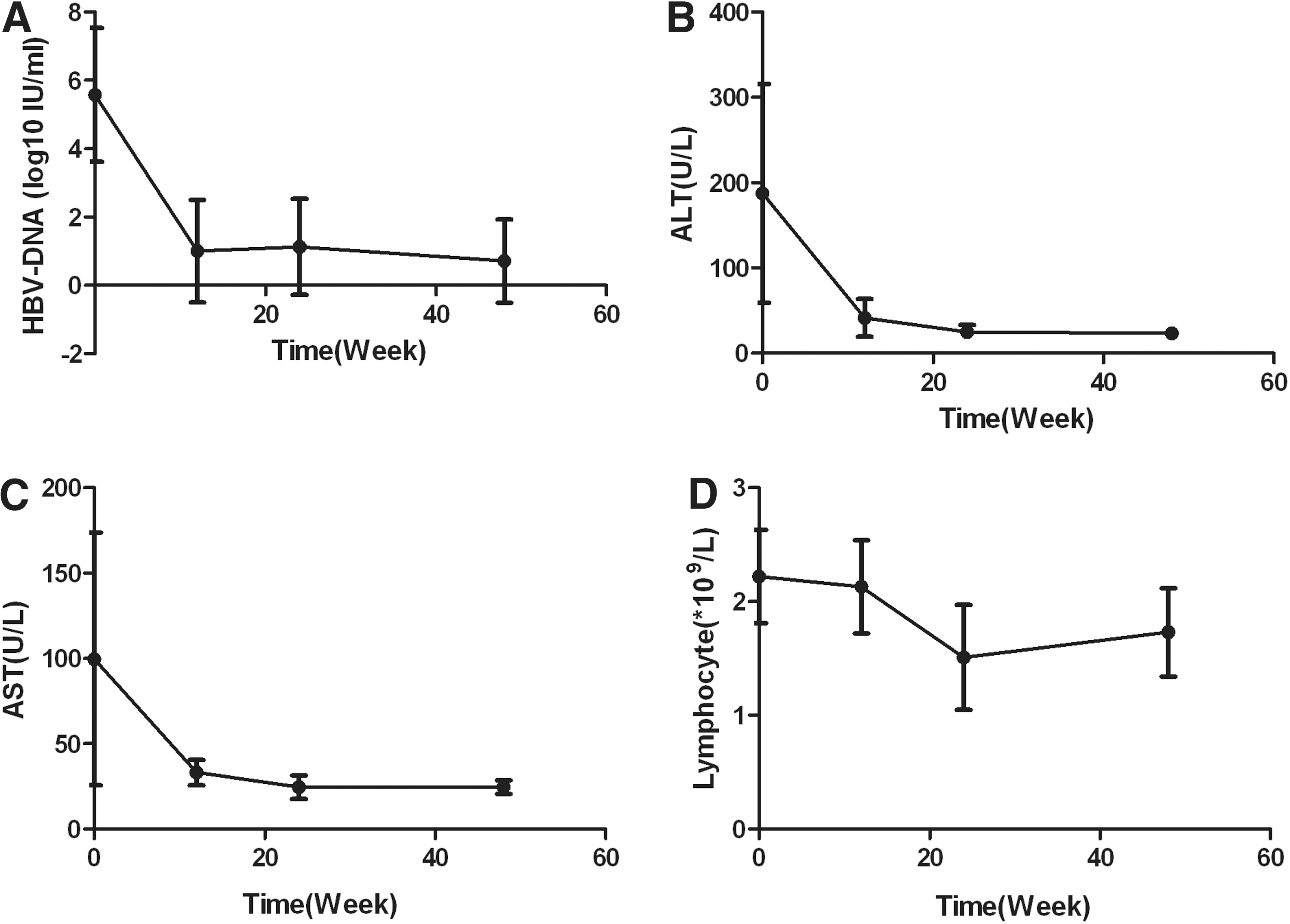
Levels of HBV-DNA, ALT, AST, and lymphocyte count decreased during interferon-α treatment.
At the end of treatment, ALT and AST levels were all normalized; no patient had a loss of serum HBsAg. In 12 hepatitis B e antigen (HBeAg)-positive patients, HBV-DNA was undetectable in 10 patients (83%) and reduced over 2 log10 IU/mL in the other two patients; there were eight cases that achieved loss of serum HBeAg (67%), and two patients (17%) had seroconversion from HBeAg to anti-HBeAg. In HBeAg-negative patients, HBV-DNA was undetectable.
Sustained fluctuations of Treg, Th17, and Th1 cells during interferon-α treatment
We longitudinally determined the proportion of Treg, Th17, and Th1 cells in peripheral blood to assess the effect of interferon-α treatment and found that there were serial fluctuations during treatment. Compared to control, the frequencies of Treg cells gradually decreased from the baseline (5.72±0.46, p=0.0019) to week 24 and then showed a V-type change at week 48 (7.19±1.6, p=0.0019) (Fig. 3A). Likewise, the frequencies of Th17 cells from baseline (3.94±0.64, p=0.0436) normalized through from week 12 to 24 and increased again at week 48 (3.68±0.62, p=0.506), although lacking significant difference (Fig. 3B). Similar to Treg and Th17 cells, Th1 cell expression decreased from baseline (12.08±7.86) to week 12 (5.65±3.9), then went up till week 48 (10.31±3.5), but there was no significant difference between the groups (Fig. 3C). Furthermore, we dissected the Treg/Th17 ratios and found that it increased from baseline 1.88±0.28 to 2.07±0.72 at week 48, but there was no significant difference between the groups (Fig. 3D). Then, we found that Treg and Th17 cells were not positively correlated with HBV-DNA levels during the treatment.
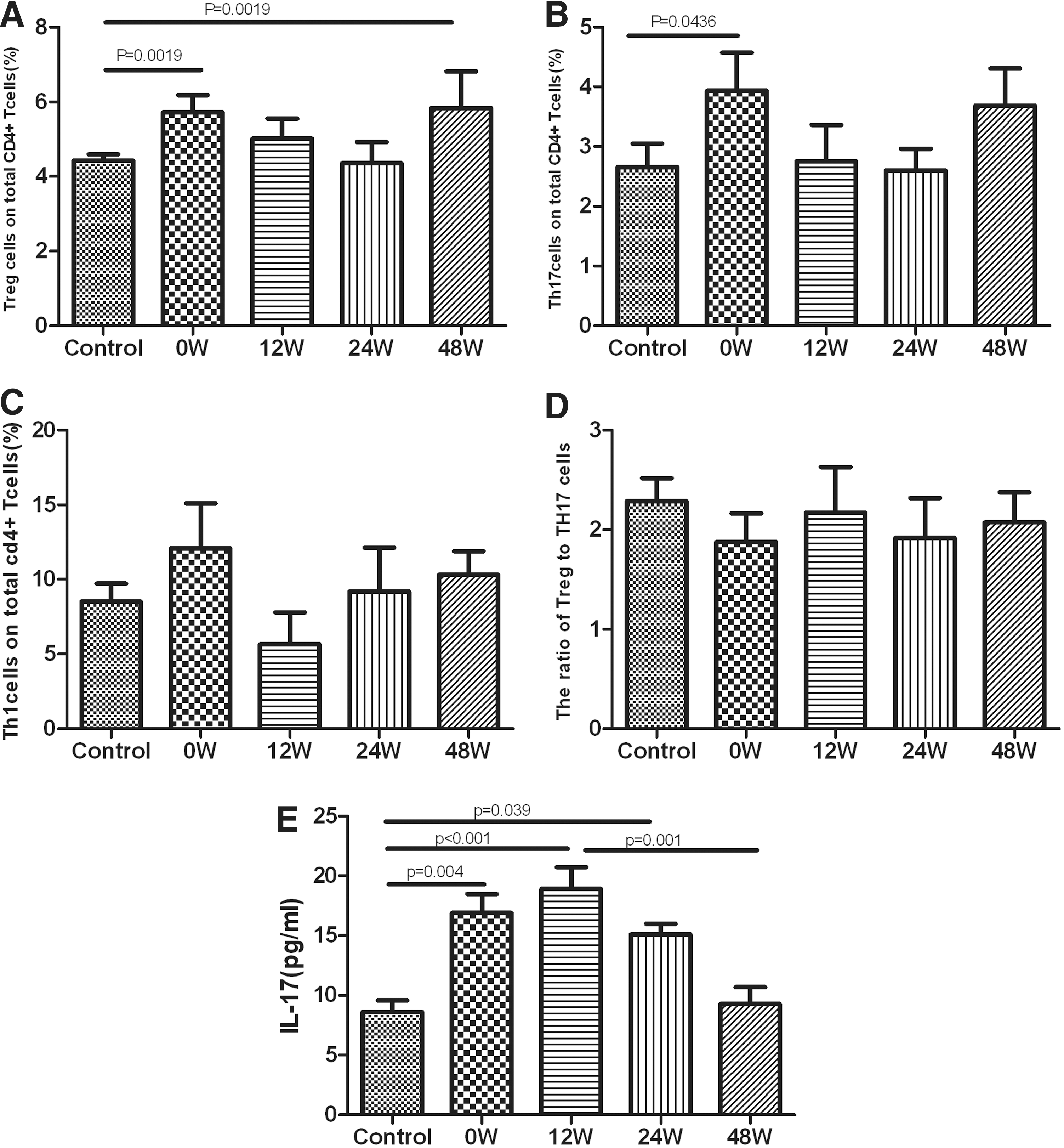
Sustained fluctuations of Treg, Th17, and Th1 cells during interferon-α treatment.
Dynamic change of IL-17A during interferon-α treatment
The levels of IL-17A production were decreased significantly in CHB patients compared to healthy subjects (16.88±5.37 vs. 8.59±3.31, p=0.004), and up to the pike value at week 12 (18.88±6.09), and steadily declined to normal (9.26±4.73) till the end of interferon-α treatment (Fig. 3E).
Discussion
Chronic HBV infection could cause autoimmune reactions to damage the liver cells directly or mediate antibody-dependent cytotoxicity that causes liver damage (16,18,27). Therefore, replication of HBV is a risk of HBV-related liver fibrosis progression (20). Previous studies confirmed that Treg and Th17 cells were significantly higher in patients with chronic HBV infection, especially in the HBV-related acute-on-chronic liver failure patients (26), and it correlated with the degree of inflammatory activity and liver pathology histological activity index (HAI) score (14). Studies also found that patients with HBV infection had a high level of Treg cells, which may contribute to viral persistence (4).
The aim of our study was to monitor longitudinally the impact of the treatment with interferon-α. Our findings showed that the Treg and Th17 cells were increased in CHB patients. In addition, the suppression of viral replication induced by interferon-α resulted in a decrease in the cells, Thus, Treg and Th17 cells might play an important role in interferon-α treatment to eliminate HBV.
Increasing evidences have shown that the response of antiviral therapy with chronic HBV-infected patients is associated with CD4+T-cell activity. NAs such as lamivudine were found to increase the CD4+T-cell response (1), and treatment of telbivudine and adefovir can reduce the frequency of the Treg and Th17 cells with an increase in the HBV-specific T-cell response (6,12,24). In our study, we also found that interferon-α treatment could partially reduce the frequency of Treg, Th17, and Th1 cells within 12 weeks.
Since Treg and Th17 cells are derived from the same original T cells and have the same cell differentiation signaling pathway with TGF-β essential for their differentiation (11,17), Th17 cells can increase the immune response by release of inflammatory cytokines and Treg cells can secrete immunosuppressive cytokines to suppress it, the imbalance between Treg/Th17 related to the occurrence of many diseases. Recent reports have shown that Treg/Th17 could be a useful marker to assess the severity of diseases (19,21). Therefore, we hypothesized that the imbalance between Treg/Th17 may exist in patients with chronic HBV infection and be corrected during anti-HBV therapy. Unexpectedly, we found that the ratio of Treg/Th17 was decreased in CHB and then it increased from 12 weeks, but there was no significant difference between the groups. Unlike NA treatment, the dynamic changes of Treg and Th17 cells during interferon-α therapy did not show the parallel relationship with the decrease of HBV-DNA that may be caused by interferon-α, which could modulate the immune system instead of blocking the duplication of HBV. It suggested that the Treg and Th17 cells balance modulated liver damage in chronic HBV infection or, alternatively, Treg/Th17 imbalance may cause HBV infection to be chronic.
Since interferon-α had dual functions of anti-HBV and immune regulation which, on one hand, resulted in the elimination of HBV-DNA and led to the change of cytokine environment, caused a temporary increase in IL-17 at 12 weeks, on the other hand, it may lead to an increased risk of autoimmune disorders. There was a rising trend in Treg and Th17 cells at the end of treatment and the count of lymphocyte increased at same time, in consideration of Treg and Th17 cells that were defined as the percentages of lymphocyte, therefore, although with no clear evidence of clinical autoimmune disease, it still suggested to us to judge the course and the curative effect of interferon-α treatment.
In conclusion, this study highlighted that the Treg and Th17 cell presence in chronic HBV infection patients was increased and changed during antiviral treatment with interferon-α; these data indicated that Th17 and Treg cells might play an important role in HBV persistence. The level of changes may be served to determine the antiviral efficacy and the degree of immune response of interferon-α therapy, which would help to improve treatment options.
The limited sample population and duration of follow-up in the study precluded us from testing the relationship about HBeAg with Th cells and the risk of clinical autoimmune disease with interferon-α therapy. Likewise, we did not perform functional studies that may help to understand the relationship between cells and interferon-α. We will further investigate the change of Treg and Th17 cells in CHB with seroconversion and the long course of interferon-α therapy. In addition, we will design a cell experiment to conform whether the cells are (dys)functional.
Footnotes
Acknowledgments
The authors thank Fan Yang who provided liver function test assistance. Grant information: this work was supported by a project funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD) (JX10231801) and the project was supported by the Medical Technology Development of Nanjing (YKK11179, YKK14220).
Authors' Contributions
Hao Feng and Jie Yin collected cases and analyzed the data, Hao Feng and Xiaoyin Zhou wrote the first draft of the article. Guoxin Zhang designed the study and proofread the manuscript. Ya-Pin Han tested guidance samples. Su Chen and Li Yang helped deal with specimens.
Author Disclosure Statement
No competing financial interests exist.