
Abstract
Hemorrhagic fever with renal syndrome (HFRS) is caused by Hantaan virus (HTNV) and Seoul virus infection in Asia. The clinical manifestation of HFRS is characterized by the rapid loss of renal function (acute kidney injury) and thrombocytopenia. The specific immune mechanisms that cause thrombocytopenia in HFRS are not well described. The growth arrest-specific 6 (Gas6) protein and TAM (Tyro3, Axl and Mer) receptors have been recently shown to play prominent roles in immune regulation, and high plasma levels of Gas6 may predict the severity of diseases. The association of TAM receptors with several autoimmune diseases has been investigated, although the relationship between TAM receptors and these diseases remains unclear in HFRS. Therefore, the aim of this study was to evaluate the clinical significance of Gas6 and TAM receptor expression in HFRS. The concentrations of Gas6 in the plasma from 144 patients and the expression of TAM receptors on monocytes from 117 patients were quantified. The relationship between Gas6 levels and disease course, severity, and clinical parameters was analyzed. We first found that the plasma Gas6 levels were significantly higher in HFRS patients, whereby they were positively correlated with white blood cell counts and negatively correlated with platelet counts. The expression of Tyro3 was increased on monocytes in HFRS patients compared with that in controls. Taken together, our data indicate that elevated plasma Gas6 levels is associated with the severity of disease during HTNV infection in humans, suggesting that Gas6 may play an important role by binding with Tyro3 on monocytes, which will be assessed in future studies.
Introduction
H
Growth arrest-specific 6 (Gas6) is a vitamin K-dependent protein that activates a family of receptor tyrosine kinases, including Tyro3, Axl, and Mer, which are known as TAM receptors (22,26). Tyro3 is mostly expressed in the central nervous system, kidneys, ovaries, and testes (6). Axl is widely expressed in most human cells, including hematopoietic, epithelial, and mesenchymal tissues (15). The expression of Mer is predominantly found in the ovaries, testes, prostate, lungs, and kidneys and to a lesser extent in the thymus, spleen, liver, small intestine, colon, and placenta (11). Gas6 can activate either the TAM receptors as a soluble factor or through opsonized phosphatidylserine (PS) on apoptotic cells (ACs) and serve as a bridging molecule between ACs and the TAM-positive phagocytes. Several functions of the TAM receptors have been described, such as mediation of clearance of ACs (1), stimulation of cell growth and proliferation (10), stimulation of hemostasis (2), and modulation of inflammation (4). For these functions, Gas6 serves as a bridge to mediate cell–cell interactions by binding both to the TAM receptors and to PS residues, which are exposed on activated platelets, injured endothelial cells, and apoptotic bodies (5,20,24). These interactions are crucial for phagocytosis and the clearance of ACs and platelets (5,20,24).
Gas6 is overexpressed in various inflammatory and autoimmunity processes. In patients with systemic lupus erythematosus, elevated serum levels of Gas6 are associated with nephritis and cutaneous vasculitis (27). Other studies have shown that Mer receptor-mediated macrophage phagocytosis is mediated mainly through soluble Gas6 as a ligand stimulating the uptake of ACs (21). This study was the first to show increased Gas6 expression in the plasma of patients with HFRS. Interestingly, the highest expression of the TAM receptors was observed for Tyro3 on monocytes in HFRS patients, which may indicate that soluble Gas6 mediates the regulation of thrombocytopenia in patients with HFRS.
Materials and Methods
Sample preparation
A total of 101 blood samples were harvested randomly from HFRS patients during the acute stage of disease, and 85 samples were harvested randomly during the convalescent stage. Twenty-six blood samples from healthy adult volunteers were obtained as normal controls. The plasma samples and the peripheral blood samples were collected and stored as previously described (23). The clinical diagnosis of HFRS was confirmed by the detection of immunoglobulin M (IgM) or IgG antibodies to HTNV in the patients' serum specimens. Based on the classically defined five stages of HFRS, the patients were divided into the acute phase (including the febrile, hypotensive, and oliguric stages) or the convalescent phase (including the diuretic and convalescent stages). HFRS disease severity was classified on the basis of the clinical and laboratory parameters used in the diagnostic criteria for HFRS in China as follows: (1) mild: mild renal failure without an obvious oliguric stage; (2) moderate: obvious symptoms of uremia, effusion (bulbar conjunctiva), hemorrhage (skin and mucous membrane), and renal failure with a typical oliguric stage; (3) severe: severe uremia, effusion (bulbar conjunctiva and either peritoneum or pleura), hemorrhage (skin and mucous membrane), and renal failure with oliguria (urine output, 50–500 mL/day) for 5 days or anuria (urine output <50 mL/day) for 2 days; and (4) critical: for those with more than one of the following symptoms during severe disease: refractory shock, visceral hemorrhage, heart failure, pulmonary edema, brain edema, severe secondary infection, and severe renal failure with either oliguria (urine output 50–500 mL/day) for >5 days or anuria (urine output <50 mL/day). The study involving human materials was approved by the Ethical Review Board of the University, and written informed consent was obtained from each HFRS patient or their guardians under a protocol approved by the Institutional Review Board of the Tangdu Hospital and the Fourth Military Medical University. The related information was used anonymously.
The clinical information of the subjects
A total of 186 plasma samples from 144 HFRS patients and 26 healthy donors were examined. The patient information is summarized in Table 1.
Gas6, growth arrest-specific 6.
Enzyme-linked immunosorbent assay
The levels of Gas6 in the plasma were measured with an enzyme-linked immunosorbent assay kit (R&D Systems) according to the manufacturer's protocol. Plasma samples (100 μL) were used for each test. The optical densities were determined at 450 nm. The concentration of Gas6 in the tested samples was estimated from a standard curve as calculated with serially diluted reconstituted Gas6 standards.
Flow cytometry
A total of 1 × 106 peripheral blood mononuclear cells were stained with fluorescent antibodies for analysis by flow cytometry. The antibodies used in the study were specific for Mer (anti-Mer-PE, clone 125518, R&D Systems), Tyro-3 (anti-Tyro-3-PE, clone 96201, R&D Systems), Axl (anti-Axl-APC, clone 108724, R&D Systems), and CD14 (anti-CD14-FITC, clone 61D3, eBioscience). Matched isotype controls were used as negative controls. The monocytes were gated based on their forward and side scatter characteristics. The data were analyzed using FlowJo 7.6.1 software (Oregon).
Detection of Gas6 binds to Tyro3 by confocal microscopy
The THP-1 cell line and HTNV strain 76–118 were prepared and stored in our laboratory. From 3 × 105 to 5 × 105 THP-1 cells were seeded in cell culture chamber slides (Thermo Scientific) and infected with HTNV virus (multiplicity of infection [MOI] = 1) for 48 h and then treated with 50 ng/mL Gas6 (R&D Systems) for another 1 h. Cells were then fixed in paraformaldehyde 4% for 15 min after washing twice in phosphate buffered saline (PBS). After the removal of the fixative by extensive wash in PBS, the samples were blocked with normal goat serum for 30 min at room temperature and then incubated with mouse antihuman Tyro3 monoclonal antibody and rabbit antihuman Gas6 monoclonal antibody (R&D Systems) diluted at 1:500 for overnight at 4°C. Antibody in excess was removed by washing in Phosphate Buffered Saline with Tween-20 (PBST) and slides were then incubated with goat antimouse Alexa Fluor® 488-conjugated antibody and donkey antirabbit Alexa Fluor 647-conjugated antibody(R&D Systems) for 1 h at 37°C. The slides were finally incubated with Hoechst 33258 (Beyotime, China) and pictures were taken by confocal laser-scanning microscopy (FluoView FV1000, Olympus, Japan).
Statistical analyses
Statistical analyses were performed using SPSS for Windows v 13.0 (SPSS, Inc.) and GraphPad Prism v 5.0 (GraphPad Software, Inc.). An unpaired Student's t test was used for comparing the disease and healthy control samples when the data showed a normal distribution. Otherwise, the Mann–Whitney U test was used. Correlations between the continuous data were assessed using the spearman correlation coefficient. A p value of less than 0.05 was considered statistically significant for all tests.
Results
Levels of Gas6 in patients with HFRS
The plasma Gas6 levels were elevated during acute phase in HFRS patients compared with the normal controls (14,825 [5,688–46,518] pg/mL vs. 5,386 [734–10,763] pg/mL, p < 0.001) and decreased during the convalescent phase (8,656 [5,742–30,115] pg/mL, p < 0.01), but remained higher than the normal control levels (p < 0.05) (Fig. 1A). Between the different severity groups, the level of Gas6 in the critical and severe groups was significantly higher than that in the mild and moderate patient groups (p < 0.01) and the control group (p < 0.001) (Fig. 1B). The acute and convalescent phase plasma Gas6 levels also showed the same tendency between the 32 observed patients (Fig. 1C).
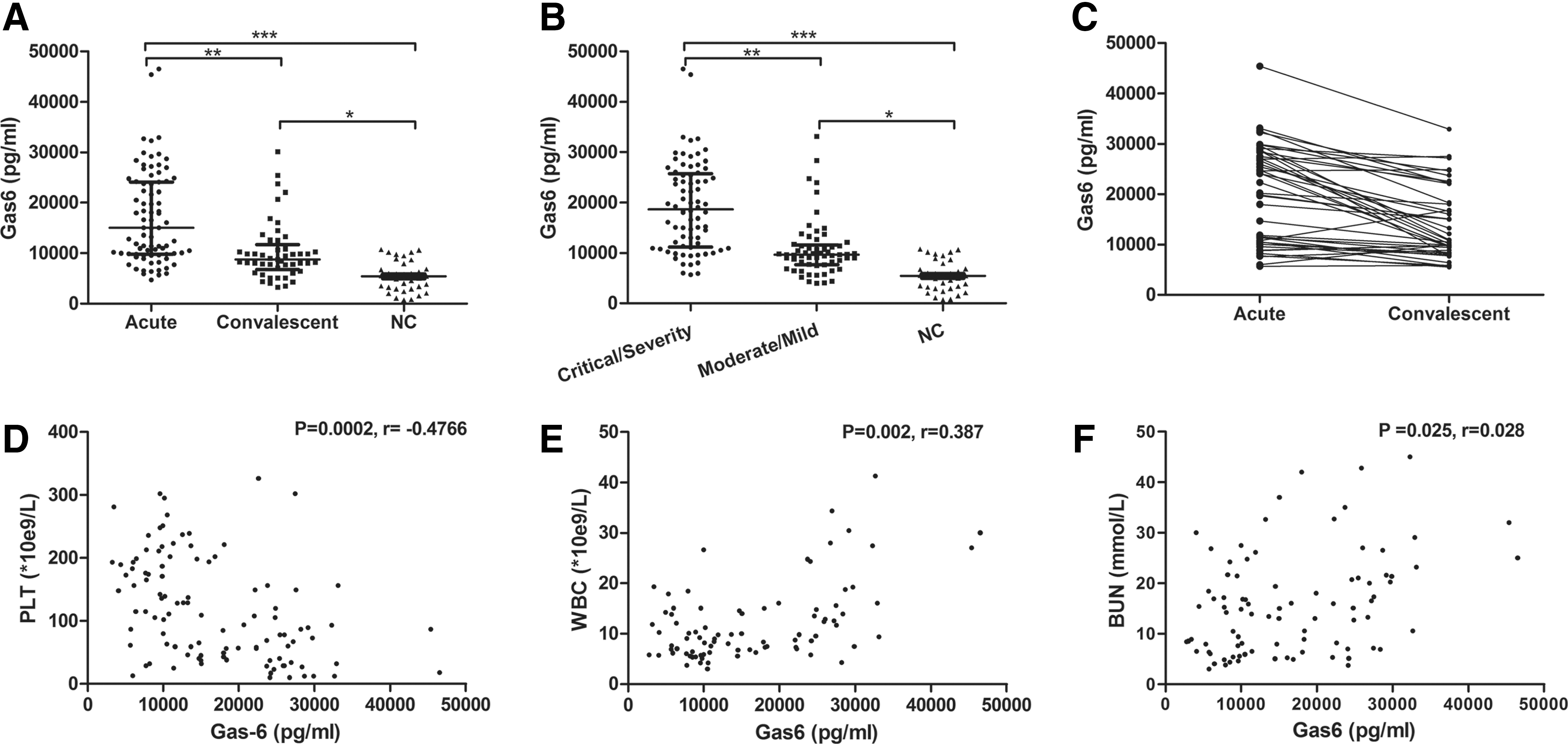
Comparison of plasma Gas6 levels in different groups of hemorrhagic fever with renal syndrome (HFRS) and its correlation with the observed clinical parameters.
Plasma Gas6 levels correlated with the clinical parameters
To determine the relationship between the plasma Gas6 level and the patients' clinical parameters, all 186 samples were analyzed for Gas6 expression. Plasma Gas6 levels were negatively correlated with the platelet counts (PLT) (r = −0.4766, p = 0.0002, Fig. 1D), positively correlated with the white blood cell counts (r = 0.387, p = 0.002, Fig. 1E) and blood urea nitrogen (r = 0.028, p = 0.025, Fig. 1F) in the patients.
Expression levels of TAM receptors on monocytes from HFRS patients
Studies have shown that Gas6 serves as a bridge by binding to both TAM receptors and to PS residues exposed on apoptotic bodies, thereby mediating clearance of ACs. Therefore, we assessed the expression of the TAM receptors on monocytes from HFRS patients, and the results showed that the expression of Tyro3 was significantly higher than that in controls (both p < 0.01, Fig. 2A), whereas there were no significant differences in monocyte Axl and Mer levels between the different groups, although Axl and Mer levels were marginally higher (p = 0.049 and p = 0.047, respectively) in the convalescent phase than in the controls (Fig. 2B, C).
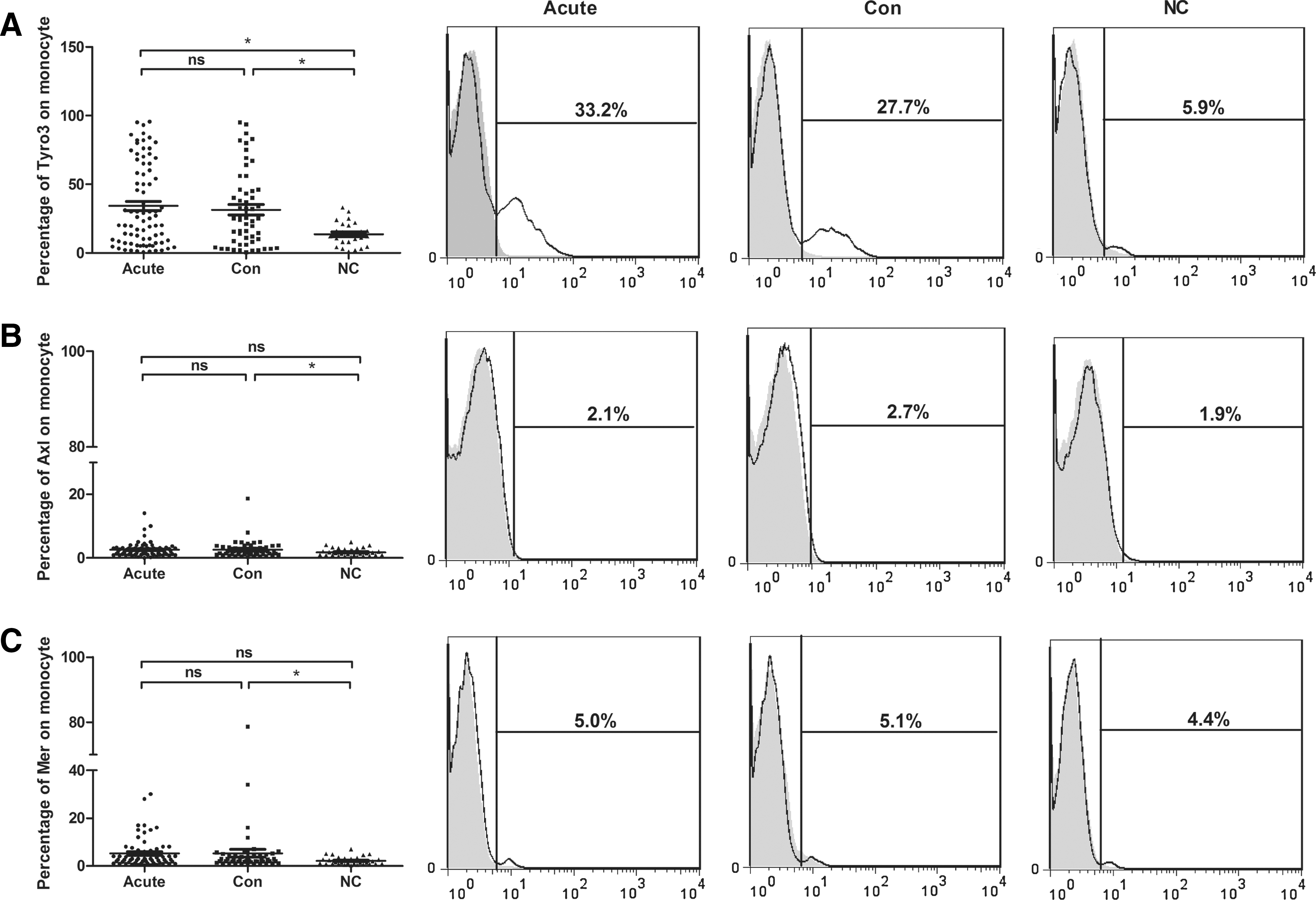
Expression of TAM receptors on monocytes from HFRS patients.
Confocal laser-scanning microscopy analysis of Gas6 binds to Tyro3
Immunofluorescence staining was used to detect the binding of Gas6 and Tyro3 in THP-1 cells after HTNV infection. Confocal laser scanning microscopy (CLSM) images on chamber slides are shown in Figure 3. The expression levels of Tyro3 in THP-1 (Fig. 3 Tyro3), those of Gas6 (Fig. 3 Gas6), and the colocalized Gas6 and Tyro3 are shown in Figure 3 to be merged. In addition, the Gas6 protein contains an N-terminal glutamic acid-rich Gla domain and a C-terminal sex hormone binding globulin (SHBG) domain comprising two Laminin G (LG) domains (13,14). The LG domains are required for TAM binding and the activation of postreceptor signaling pathways (25). They suggested that Gas6 may bind to Tyro3 on HTNV-infected THP-1 cells in vitro, at least partially.
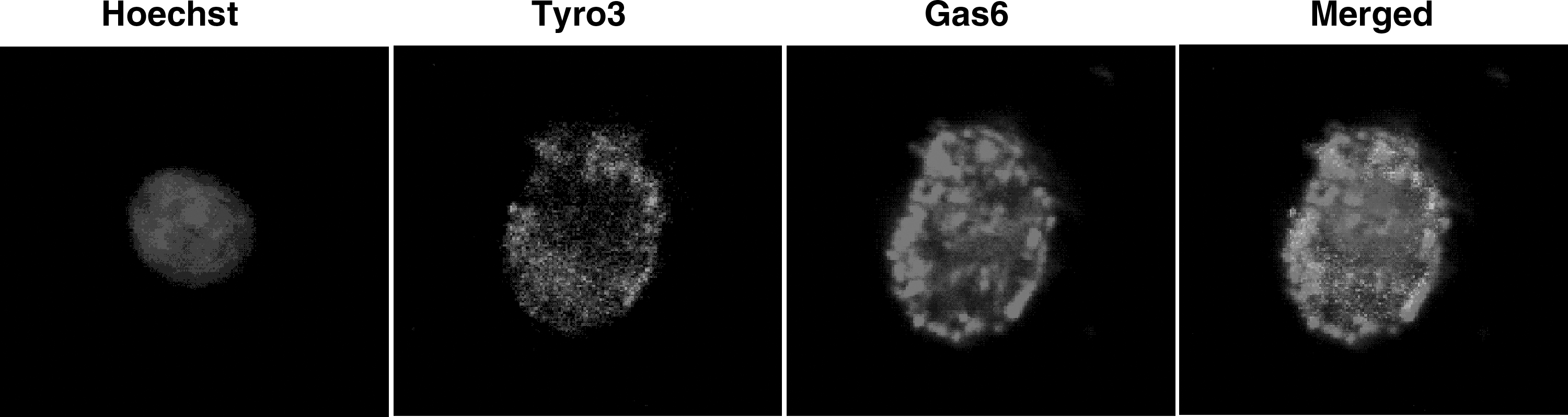
Confocal laser-scanning microscopy images of THP-1 cells after HTNV infection. Cells stained for nuclei (Hoechst 33258), Tyro3(Alexa Fluor® 488), and Gas6 (Alexa Fluor 647). Panels represent images taken at the level of nuclei(40 × ). HTNV, Hantaan virus.
Discussion
Despite recent progress in understanding the mechanism for thrombocytopenia in HFRS, the immunological component of this disease has remained unclear (28). Identifying the expression of the TAM receptors on monocytes will aid in understanding the role of Gas6 in the clearance of ACs, including apoptotic platelets.
In this study, we demonstrated for the first time that the plasma Gas6 level and the expression of the TAM receptor Tyro3 on monocytes were substantially elevated in HFRS patients. Furthermore, the elevated plasma Gas6 levels were negatively correlated with the platelet counts. Nadir platelets have been identified as a major diagnostic feature in patients with HFRS (7), which indicates a correlation between increased plasma Gas6 levels and thrombocytopenia during HTNV infection. To better clarify the correlation between the Gas6 levels and thrombocytopenia in HFRS, we further analyzed the changes of Gas6 in different types of HFRS patients and the expression of the TAM receptor Tyro3 on monocytes from the patients. The results showed that the levels of Gas6 in patients with critical and severe disease forms during the acute stage were significantly higher than those in patients with mild and moderate disease and the controls (p < 0.05). In addition, the Tyro3+ monocyte proportions in patients in the acute and convalescent phases were significantly higher than those in the controls. Although Axl and Mer levels were higher in the convalescent phase than those in the controls, when remove the peak point, there were no significant differences between the different groups. Figure 3 shows that Gas6 could bind to Tyro3 in vitro, which indicates that Gas6 may play an essential role in HFRS as a thrombocytopenia marker.
A decrease in the number of platelets is a common finding among patients with viral hemorrhagic fever (8). There are several immunological mechanisms that destroy platelets, including the sequestration of platelets by macrophages at the infection site and/or in the spleen in patients with severe fever and thrombocytopenia syndrome because of viral infection (12), platelet–leukocyte aggregation and subsequent phagocytosis by monocyte/macrophages (9), and destruction mediated by platelet–virus-associated antibodies in patients with secondary dengue virus infection (18). However, the immunological mechanisms underlying thrombocytopenia in patients with HFRS disease are not known.
In a model of lupus-like autoimmune syndrome, there is some evidence that Mer-mediated macrophage phagocytosis is mediated mainly through the soluble bridge ligand Gas6 (21). Similarly, the TAM receptor Mer enables M2c macrophages to clear early ACs more efficiently and mediates AC clearance by CD14brightCD16+ monocytes through soluble Gas6. Gas6 molecule serves as phagocytic opsonin based its structure with N-terminal Gla domain binding to PS-containing phospholipids including apoptotic platelets, and a C-terminal SHBG-like domain that interacts with the TAM receptors on phagocytes (29). In addition, several studies have focused on the role of TAM receptors in infection by viruses, such as vaccinia virus, cytomegalovirus, Lassa fever virus, and HIV (3). These enveloped viruses display PS as a so-called eat me signal on the extracellular membrane surface in a process termed “apoptotic mimicry” (17). Whether exposure of PS on the surface of ACs and activated platelets leads to the binding of elevated Gas6 in the local environment and the C-terminal SHBG-like domain of Gas6 interacting with Tyro3 on monocytes in HFRS should be assessed in future studies.
In conclusion, elevated plasma Gas6 levels were associated with the severity of HFRS disease and were negatively correlated with the platelet counts. In addition, Gas6 may cooperate with the Tyro3 receptor on monocytes to participate in phagocytosis during HTNV infection. These results provide insights into the understanding of the immunological mechanisms of thrombocytopenia in HFRS.
Footnotes
Acknowledgments
This study was supported by the National Program on Key Basic Research Project (973 Program, No. 2012CB518905), the National Natural Science Foundation of China (No. 81501362), and the Natural Science Basic Research Project in Shaanxi Province (No. 2014JM4124).
Author Disclosure Statement
No competing financial interests exist.