
Abstract
The human T-lymphotropic virus 1 (HTLV-1) is the causative agent of HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP). The present study investigated the association between the rs2275913 polymorphism in the IL17A gene and the development of HAM/TSP. Peripheral blood samples were collected from 116 patients (29 symptomatic patients with HAM/TSP and 87 asymptomatic) with a positive diagnosis of HTLV-1. The single nucleotide polymorphism genotyping was carried out by real time quantitative PCR (RT-qPCR) using TaqMan® probes. In addition, serum levels of IL-2, IFN-γ, TNF-α, IL-4, IL-6, IL-10, and IL-17 were measured in 64 infected individuals from the study (47 asymptomatic and 17 HAM/TSP), using cytometric bead array technique. No significant differences were found in genotypic and allelic frequencies between the groups. Analysis of cytokine levels showed highest concentrations of IFN-γ and TNF-α in HAM/TSP patients. The results of the present study, therefore, suggest a lack of association between the rs2275913 polymorphism in the IL17A gene and the presence of HAM/TSP.
Introduction
H
HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP) is a chronic demyelinating and disabling syndrome caused by HTLV-1 and affects 0.25–3.8% of infected individuals, leading to progressive weakness in the lower limbs, erectile dysfunction, bladder and intestine weakness, besides pain in legs and lower back (2,33). Although the pathogenic mechanisms leading to the development of this disease are not well understood, it is known that genetic factors such as polymorphisms in the genes involved in the immune response, as well as viral factors and immunological factors, mainly the balance of proinflammatory and anti-inflammatory cytokines, may be involved in the development of myelopathy (26,30).
In the immune response against HTLV, Th1 cytokines such as IFN-γ, TNF-α, and IL-6 are prominent, whereas Th2 cytokines are reduced, but studies have shown that Th17 cells may be involved in the immunopathogenesis of infection (1,19,33).
Recent studies have shown an association between a single nucleotide polymorphism (SNP) in the IL17A gene, which produces the proinflammatory cytokine IL-17A, and susceptibility to various inflammatory diseases (3,17,22,23,25,31). IL-17A is responsible for inducing cell types to produce other proinflammatory cytokines, chemokines, and metalloproteinases, resulting in the recruitment of neutrophils to the tissue, thereby contributing to inflammation process (5).
One of the polymorphisms of the IL17A gene is G-197A SNP (rs2275913), which can affect the regulation of the IL-17 transcription (9,32). This SNP has been associated with the development of inflammatory conditions of several diseases, such as rheumatoid arthritis, a disease that shares various immunological features with HAM/TSP (22). However, the role of this SNP in the pathogenesis of HAM/TSP remains unknown. Therefore, the aim of the present study was to investigate the association between G-197A polymorphism and susceptibility to HAM/TSP, as well as to evaluate proinflammatory and anti-inflammatory cytokine levels in patients from the northeast region of Brazil infected with HTLV-1.
Materials and Methods
We recruited 87 asymptomatic individuals (52 women and 35 men) and 29 HAM/TSP patients (23 women and 6 men), totaling 116 infected subjects. The mean age of patients was 49.6 years, ranging from 20 to 76 years.
The HAM/TSP was diagnosed according to the World Health Organization diagnostic criteria for HTLV-1-associated diseases (24). A study conducted in Central America showed that the HAM/TSP establishment seems to occur on average 3.3 years after infection (16). Therefore, to minimize the possibility of including patients that still might develop HAM/TSP, we included only asymptomatic patients with more than 3 years of clinical follow-up. All individuals were from the same geographical area, the state of Pernambuco, presenting the same characteristic Brazilian ethnic background.
Peripheral blood samples were collected and the DNA was extracted using the Wizard® Genomic DNA Purification Extraction Kit (Promega, Madison, WI). The G-197A polymorphism genotyping was performed by real time quantitative PCR (RT-qPCR) using the TaqMan® SNP Genotyping Assay Kit (ID C_15879983_10), according to the manufacturer's instructions (Applied Biosystems, ABI, Foster City, CA), under the following conditions: 10 min at 95°C, followed by 40 cycles (15 sec at 92°C followed by 60 sec at 60°C) and 30 sec at 60°C.
The cytokines IL-2, IFN-γ, TNF-α, IL-4, IL-6, IL-10, and IL-17 were measured from the serum of 64 infected individuals (47 asymptomatic and 17 HAM/TSP), using the Human Th1/Th2/Th17 Cytometric Bead Array (CBA) Kit (BD Biosciences, San Jose, CA), according to the manufacturer's instructions. All samples were analyzed on the FACSCalibur™ Flow Cytometer using CellQuest Pro Software (BD Biosciences).
Statistical analyses and associations between groups regarding SNP frequencies were performed using the chi-square test. The SNP frequencies were also tested for Hardy–Weinberg equilibrium. Quantitative analysis of cytokine levels was expressed as mean, and the differences were investigated using Mann–Whitney test. Differences were considered significant at p < 0.05. For these analyses, we used GraphPad Prism 5.0 software.
All procedures performed in this study were in accordance with the ethical standards of the Ethics Committee of the University of Pernambuco (CEP HUOC/PROCAPE–Registration number: CAAE 16973113.5.1001.5192) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All participants of this study gave written informed consent.
Results
IL17A G-197A polymorphism was not associated with HAM/TSP outcome. No significant differences were found related to the genotypic and allelic frequencies between HAM/TSP patients and asymptomatic carriers, regardless of the genetic model for statistical analysis used (Table 1).
Chi-square test.
HAM/TSP, human T-lymphotropic virus 1-associated myelopathy/tropical spastic paraparesis.
However, the present study was the first to address polymorphism in the IL17 gene in patients infected with HTLV-1.
The results of CBA showed significant associations in the levels of IFN-γ and TNF-α in the serum of the groups (Fig. 1). However, no significant differences were observed in the case of levels of IL-2, IL-4, IL-6, IL-10, and IL-17 between the groups (Table 2). IL-17 protein was undetectable in all the samples.
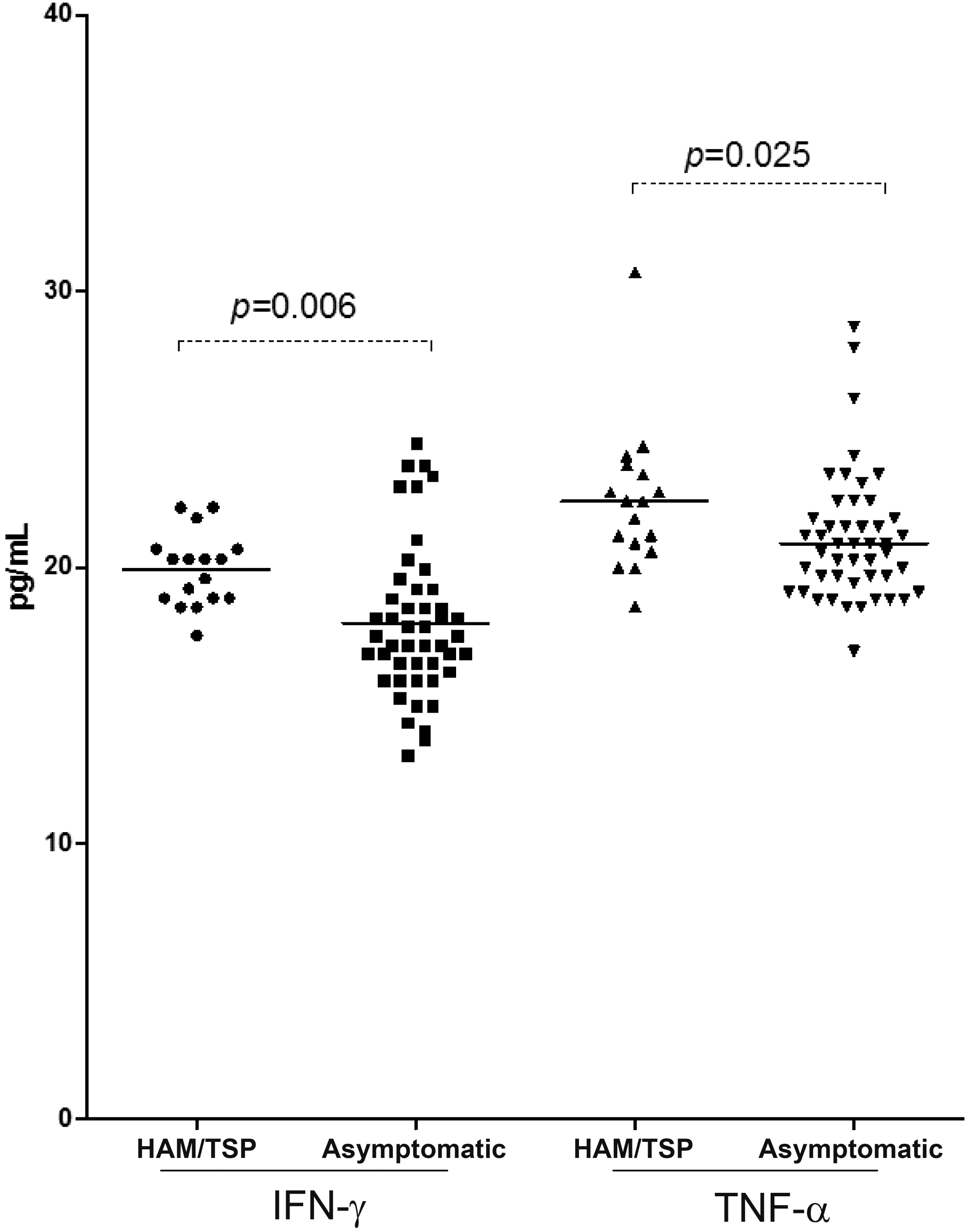
Serum level of IFN-γ and TNF-α in HAM/TSP and asymptomatic groups.
The values of p with statistically significant difference (0.0065 and 0.0253) are highlighted in bold.
Student's t-test or Mann–Whitney test as appropriate.
Discussion
The polymorphism G-197A, also known as rs2275913, is located in the binding domain for nuclear factor of activated Tcells, the central regulator of the IL-17 gene promoter. This SNP has been associated with the risk of childhood asthma, cervical cancer in women, stomach cancer, breast cancer, rheumatoid arthritis, ulcerative colitis, and other diseases. These studies rank A alelle (−197A) as the risk factor responsible for inflammatory conditions shown (5,15,22,25,31,34). Including a study involving in vitro stimulation observed that healthy T cells with the A allele produced more IL-17 compared with cells lacking this allele (9).
Several independent signals may thus be acting on the development of HAM/TSP, showing that this is a complex disease in which a number of factors are involved in the onset of symptoms. The viral protein Tax, for example, is capable of regulating the expression of the IL17 gene (8). Apart from the polymorphism investigated in the present study, other SNPs in the IL17A or other genes, in addition to the already mentioned viral and environmental factors, may therefore also be related to the disease.
The virus–host interaction is another factor responsible for causing changes in the immune response that may lead to pathogenesis of HAM/TSP, such as increased production of inflammatory cytokines and spontaneous proliferation of CD4+ T cells (11).
The present study found statistically significant differences between the IFN-γ and TNF-α levels of symptomatic and asymptomatic individuals, with high levels of these proinflammatory cytokines related to the HAM/TSP outcome. This result is in accordance with the literature, where it has been seen that Th1 cytokines such as IFN-γ and TNF-α are prominent in HAM/TSP patients, whereas Th2 cytokines such as IL-4 and IL-10 are reduced (1,19,33).
The chronic inflammatory process in HAM/TSP patients is maintained by the constant inflammatory response triggered by increased production of IFN-γ, TNF-α, and IL-2, initiated by the CD4+ T cell response (14,20).
IFN-γ has antiviral, antiparasitic, and immunomodulatory activity and is able to inhibit proliferation of cells producing cytokines (11,18,28,29). In accordance with other studies, this study found significant association between IFN-γ levels and HAM/TSP.
The production of TNF-α by T cells from HAM/TSP patients has been well described in several studies (13,21). More recent research has also found higher serum TNF-α in individuals with HAM/TSP compared with asymptomatic carriers (29). Some studies have even used anti-TNF-α agents to treat symptoms and diseases related to HTLV-1, such as arthropathy and other rheumatic conditions associated with the virus (4,10).
Curiously, the present study found no IL-17 protein in the samples. This cytokine may be released only locally and in small quantities, which would hinder its detection in certain sites.
However, HAM/TSP shares some similarities with chronic inflammatory diseases such as multiple sclerosis and rheumatoid arthritis, conditions that usually present high levels of IL-17. Additionally, it was already described that HAM/TSP patients have high levels of ROR, IL-17, and IL-22, compared with healthy individuals. Therefore, the presence of a Th17 response in HTLV-1 has occasionally been shown (11,27).
The immunogenetic profile of patients infected with HTLV-1 is important for identification of potential biomarkers of disease progression. However, the results of the present study suggest the lack of association between G-197A polymorphism and HAM/TSP. The sample size, however, was limited and population-scale genetic studies with larger samples may confirm or refute the results presented here. These results nevertheless contribute to the better understanding of the immune response present in HAM/TSP, a disease described 32 years ago, but whose immunopathogenesis has still not been fully elucidated, thereby hindering the development of effective therapies for the symptoms caused by the virus.
Footnotes
Acknowledgments
The authors thank the FACEPE (Pernambuco Research Foundation) and Oswaldo Cruz Foundation for financial support to this research and also to the individuals infected with Human T-Lymphotropic Virus 1 for agreeing to participate in this study.
Author Disclosure Statement
No competing financial interests exist.