
Abstract
Peripheral blood mononuclear cells (PBMCs) play a critical role in clearing hepatitis C virus (HCV). PBMC defects have been linked with HCV infection; however, the underlying mechanisms remain obscure. We hypothesized that PBMCs of HCV-infected patients are more susceptible to programmed cell death (PCD), and are therefore unable to clear HCV. We compared spontaneous PBMC PCD and cytokine [interleukin (IL)-1, -6, -8, -10, and -12] secretion between untreated (naive) HCV+ and treated [sustained responder (SR)] patients with HCV, and HCV− healthy controls. Spontaneous PBMC PCD was assessed by annexin-V fluorescein isothiocyanate/propidium iodide staining, and cytokine levels were measured by cytometric bead array. Differences between groups were analyzed through paired and nonpaired t tests and Mann–Whitney U test. The rate of spontaneous PCD was higher in PBMCs of naive HCV+ patients (p < 0.0001) and SR-HCV patients (p < 0.002) than in HCV− controls. Significantly low levels of IL-8, -6, and -10 were detected in the supernatant of cell cultures of PBMCs from naive HCV+ (p < 0.05) and SR-HCV (p < 0.05) patients relative to HCV− controls. There was no difference between the naive HCV+ and SR-HCV groups in terms of PBMC PCD rate or cytokine levels. The present findings indicate that HCV infection is associated with increased PBMC susceptibility to PCD and decreased production of IL-8, -6, and -10.
Introduction
I
Programmed cell death (PCD) through apoptosis plays a key role in the maintenance of cellular homeostasis; dysregulation of apoptotic processes may lead to malignancies and/or immune dysfunction (1). Apoptosis is triggered either by cell surface death receptors (extrinsic pathway) or by disruption of the mitochondrial membrane potential (intrinsic pathway). During apoptosis, downstream effector caspases 3, 6, and 7 are activated, resulting in nuclear poly (ADP-ribose) polymerase cleavage, DNA fragmentation, and cell death (1). Several studies have demonstrated a role for PCD in HCV pathogenesis during liver inflammation and fibrosis, or its progression to hepatocellular carcinoma (6,8,10,18).
The phagocytic and cytolytic activities of PBMCs are critical for pathogen clearance. After activation, increased production of cytokines such as interleukin (IL)-1α and β, -2, -6, -10, -12, and -18 by PBMCs is crucial for induction of the adaptive immune response. We hypothesized that PBMCs of HCV-infected patients exhibit elevated susceptibility to PCD, and are therefore unable to clear HCV. In this work, we investigated whether PBMCs of chronic HCV patients are more susceptible to PCD than those of healthy controls by comparing spontaneous PCD and cytokine secretion between PBMCs from HCV+ patients and those from HCV− healthy controls.
Materials and Methods
Patient characteristics
This cross-sectional study was performed at King Khalid University Hospital (KKUH), Riyadh. A total of 27 HCV patients were included in the study (Table 1); of these, 19 patients were recruited before initiation of antiviral therapy (naive HCV+ group) and had a relatively high viral load (mean = 1.35 × 106 ± 1.72 × 106 IU/mL), whereas 8 patients had undergone successful antiviral treatment [sustained responder (SR)-HCV group] and had not displayed detectable HCV RNA for at least 6 months before enrollment in the study. Patients who were coinfected with hepatitis B virus (HBV) or the human immunodeficiency virus (HIV), or had detectable HCV viral loads after 6 months, were excluded from the study. In addition, 20 healthy volunteers with no evidence of current or past infection with HIV, human T-lymphotropic virus, or HBV and HCV were included as a control group. The antiviral treatment regimen was a combination of pegylated IFN and ribavirin for 12 months. All experiments were performed in compliance with relevant regulations and institutional guidelines, and in accordance with the ethical standards set by the Declaration of Helsinki. The protocol of the study was approved by the Institutional Review Board of the College of Medicine, King Saud University. All patients were enrolled in the study after providing written informed consent.
ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; HCV, hepatitis C virus; IFN, interferon; ND, not done; SD, standard deviation; SR, sustained responder.
Quantification of viral load
HCV load in serum samples was measured using the COBAS TaqMan analyzer and the AmpliPrep/COBAS TaqMan HCV Quantities test v 2.0 (Roche Diagnostics, Manheim, Germany) following the manufacturer's protocol.
PBMC isolation and cell viability assay
Whole blood was collected in 10-mL vacutainer tubes containing EDTA (BD Biosciences, Franklin Lakes, NJ). PBMCs were isolated from whole blood by density gradient centrifugation. The blood was layered on top of 4 mL of Ficoll-Paque Plus (GE Healthcare, Piscataway, NJ) in 15-mL tubes and centrifuged for 30 min at 400 × g with the brake set to off. PBMCs in the interphase layer were collected and washed twice with sterile phosphate-buffered saline (GIBCO Invitrogen), followed by complete culture medium [RPMI 1640 medium (GIBCO Life Technologies) supplemented with 10% fetal bovine serum (GIBCO Invitrogen)]. Equal number (4 × 105 cells) of PBMCs were left uncultured (designated as “0 h” sample) or cultured in complete medium for 24 h and counted after the culturing with no significant increase in the number of cells. Cells were then washed with annexin-binding buffer (ABB): 10 mM HEPES, 140 mM NaCl, 2.5 mM CaCl2, pH 7.4, and then resuspended in 100 μL of the same buffer. Annexin V-fluorescein isothiocyanate (FITC), 5/100 μL of cell suspension, and propidium iodide (PI), 0.1 μg/100 μL of cell suspension (Molecular Probes, Eugene, OR) were added to the cells, followed by incubation in the dark at 25°C for 15 min. After addition of ABB (300 μL/sample), samples were analyzed by flow cytometry on an FACSCalibur instrument (BD Biosciences, Great Lakes, NJ). Data were analyzed using CellQuest software (BD Biosciences). The percentage of cell death was calculated by adding the percentages of annexin V-FITC single-positive and annexin V-FITC/PI double-positive cells.
Cytometric bead array for human inflammatory cytokine detection
Supernatants from purified PBMCs (4 × 105 cells) cultured in complete medium for 24 h were collected and assayed with the cytometric bead array (CBA) human inflammatory cytokine kit (BD Biosciences) according to the manufacturer's instructions as previously described (2). Cytokine levels (pg/mL) were determined using the FCAP Array software (BD Biosciences).
Statistical analysis
Data were analyzed using GraphPad Prism 5 software (GraphPad, Inc., San Diego, CA). Paired t tests were used to assess the statistical significance between two different time points of the same patient, whereas nonpaired t test and Mann–Whitney U test were employed to evaluate the significance of differences between different groups; p ≤ 0.05 was considered statistically significant.
Results
Increased spontaneous PCD in PBMCs from HCV-infected patients
We hypothesized that PBMCs from HCV patients become sensitized by endogenous cytokines and are, therefore, more susceptible to cell death. We evaluated PCD in PBMCs (4 × 105 cells) that were freshly isolated (0 h) or cultured for 24 h by annexin V-FITC/PI staining and flow cytometry. The percentage of PBMCs undergoing spontaneous PCD was significantly higher in naive HCV+ patients (mean = 41.9% ± 13.1%) than in HCV− donors (mean = 20.6% ± 5.4%, p < 0.002) (Fig. 1A). Spontaneous PCD rate was also higher in PBMCs of the SR-HCV group (mean = 35.7% ± 19.3%) than those from HCV− donors (mean = 20.6% ± 5.4%), but the difference was not statistically significant. After 24 h of culture, the percentage of PBMC death further increased in the naive HCV+ group (mean = 54.5% ± 13.9%, p < 0.0001) and the SR-HCV group (mean = 45.7% ± 17.9%, p < 0.001), but not in the control group (mean = 22.5% ± 6.4%) (Fig. 1A). The rate of spontaneous PBMC death was the highest in naive HCV+ patients (mean = 53.6% ± 14.6%, p < 0.0001), followed by SR-HCV patients (mean = 41.2% ± 17.4%, p < 0.002) and HCV− controls (mean = 23.9% ± 5.1%) (Fig. 1B). The difference between PBMC spontaneous PCD rates in naive HCV+ patients and in SR-HCV patients was not statistically significant (Fig. 1B).

Spontaneous PCD in PBMCs from the patient study groups. Purified PBMCs (4 × 105 cells) were left uncultured or cultured in complete medium for 24 h. Subsequently, cells were stained with annexin-V-FITC and PI and analyzed by flow cytometry. The percentage cell death in PBMCs of each group was graphed.
Reduced levels of IL-8, -6, and -10 secretion in PBMCs of HCV-infected patients
Given the observed increase in spontaneous PBMC death rate in HCV+ patients, we investigated the effect of HCV on cytokine production by PBMCs. Purified PBMCs (4 × 105 cells) were cultured for 24 h, and the supernatant was collected for assessment of cytokines by CBA and flow cytometry. All proinflammatory cytokines, including IL-8, -6, -10, -1β, and -12p70, were detected in the supernatant of PBMC cultures from all groups. The levels of IL-8, -6, and -10 were significantly lower in the PBMC culture supernatants from naive HCV+ (mean values: 821.4 ± 629.9, 15.9 ± 13.8, and 4.1 ± 0.5, respectively) and SR-HCV patients (mean values: 1287.8 ± 1034.1, 14.5 ± 8.2, and 4.1 ± 0.7, respectively) than those from HCV− controls (mean values: = 2581.5 ± 1670.1, 30.2 ± 16.9, and 4.8 ± 0.7, respectively) (p < 0.05; Fig. 2). Cytokine levels of HCV+ and SR-HCV patients were similar. No statistically significant difference was observed in the concentrations of IL-1β and IL-12p70 among the three study groups.
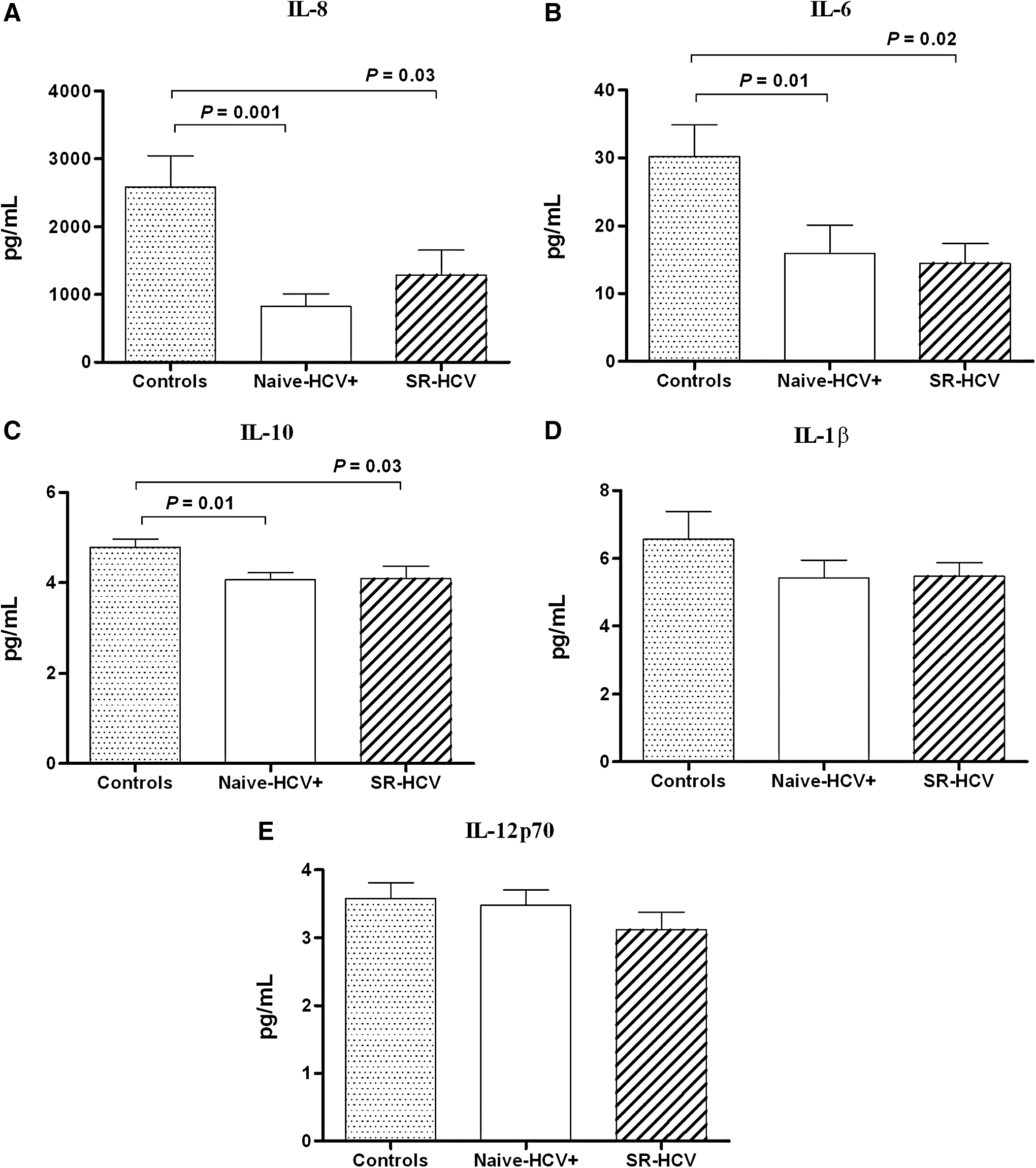
Human inflammatory cytokine levels in supernatant of PBMCs from patient study groups. Patient PBMCs (4 × 105 cells) were cultured in complete medium for 24 h. Supernatants were collected and analyzed using the CBA human inflammatory kit and flow cytometry.
Discussion
PBMCs from naive HCV+ and SR-HCV patients exhibited significantly higher rates of spontaneous PCD than those from HCV− controls. These observations were consistent with other studies (1,16,24). Upon starvation, monocytes and T lymphocytes from chronic HCV+ patients and HCV+ patients with liver cirrhosis or hepatocellular carcinoma have been reported to display higher death rates than controls (16). This increase in spontaneous PCD rates may be attributed to the upregulation of apoptotic genes in the PBMCs of HCV+ patients, such as Fas, CASP3, CASP8, and CASP9 (1).
We report here for the first time that increased susceptibility of PBMCs to spontaneous PCD was associated with decreased levels of IL-6, -8, and -10 in supernatants of PBMC cultures from HCV+ patients. These findings substantiate earlier observations suggesting that increased syntheses of IL-10 and IL-8 are predictors of unfavorable prognosis of IFN therapy (14). Moreover, increased production of IL-8 has been linked with histological evidence of progressed inflammation, and persistently elevated levels of IL-8 are believed to be a strong predictor of progression to cirrhosis (17). Even though low levels of supernatant proinflammatory cytokines could indicate a favorable outcome, they may have an adverse effect on the survival of PBMCs.
We have previously shown that plasma levels of IL-1, -6, -8, and -10 are higher in naive HCV+ patients than in HCV− donors (2). Several other studies have also reported increased blood levels of IL-6, -8, and -10 among patients infected with HCV (3,19,20,25,29). These cytokines appear to be critical for PBMC survival as recombinant IL-8 inhibits apoptosis of endothelial cells by enhancing the expression of antiapoptotic genes such as B cell lymphoma 2 (Bcl-2) and extra large Bcl-xL (12). Similarly, IL-10 has been shown to block spontaneous T cell apoptosis in infectious mononucleosis (23). IL-6 prevents cluster of differentiation 3-induced T cell death and hydrogen peroxide-induced apoptosis of alveolar epithelial cells (5,11). These data indicate that despite high blood levels of antiapoptotic cytokines such as IL-8, IL-10, and IL-6, PBMCs from HCV-infected patients are more prone to cell death. It is possible that factors related to the physical presence of HCV are critical for the enhanced susceptibility to cell death observed in this study. However, this was a cross-sectional study limited by the small number of patients studied. A large-scale longitudinal study is recommended to validate the current findings.
Conclusion
In this study, PBMCs from HCV+ patients were compared with those from HCV− healthy controls to determine whether the former exhibited increased susceptibility to PCD. Our findings revealed that PBMCs from HCV+ patients were more susceptible to spontaneous PCD than those from HCV− controls. This difference was associated with impaired IL-6, -8, and -10 secretion in HCV+ patients and may thus contribute to failure of HCV clearance.
Footnotes
Acknowledgments
This study was funded by King Abdulaziz City for Science and Technology (grant No.: P-C-11-0583). The authors thank the Faculty of Medicine, King Saud University, King Khalid University Hospital, and the Liver Center Research Institute for their collaboration and assistance in the recruitment of patients.
Author Disclosure Statement
No competing financial interests exist.