
Abstract
To determine the association between BK polyomavirus (BKPyV) types 1 and 4 capsid antibody and natalizumab-associated progressive multifocal leukoencephalopathy (PML) in patients with multiple sclerosis (MS), serum samples were obtained from 10 natalizumab-associated PML cases and 130 control MS patients treated with natalizumab, and 82 control MS patients never exposed to natalizumab. In a sex- and age-adjusted regression model, BKPyV serotype 1 antibody levels were significantly higher in natalizumab-treated controls (p = 0.009) compared with cases, and were higher in controls never treated with natalizumab compared with cases, but the difference did not reach statistical significance (p = 0.158). There was no association between BKPyV serotype 4 antibody and PML. We hypothesize that a robust immune response to BKPyV may be protective against the development of PML.
Background
P
An old but as yet unexplained serological observation is an inverse correlation between levels of antibody to JCPyV and levels of antibody to another genetically closely related human virus, BK polyomavirus (BKPyV) (6,8,10). In a previous study (16) we demonstrated an association between low levels of antibody to BKPyV serotype 1 and 4 and risk for subsequent development of PML in HIV-infected patients. The goal of this study was to investigate the association between the level of antibody against BKPyV and the risk of natalizumab-associated PML in patients with MS.
Materials and Methods
Patient populations
We obtained serum samples from 10 natalizumab-associated PML patients from three MS care centers in Italy, Sant'Andrea University Hospital, Roma, San Raffaele Hospital, Milano, and Spedali Civili, Brescia. Patients were diagnosed with PML between 2011 and 2014. The diagnosis was made in all cases by demonstration of JC virus DNA by PCR in central spinal fluid (3). Collaborating investigators from the centers provided samples after they were deidentified.
As a control group we obtained serum samples from 212 MS patients followed in the MS care center of the Sant'Andrea University Hospital in Rome.
One hundred thirty serum samples from patients taking natalizumab were collected between October and November 2014; at the time the patients came to the Sant'Andrea MS clinic for monthly natalizumab infusion on Monday, Wednesday, or Friday. All the patients participating in the study gave their written consent and less than 5% of the invited patients refused to participate in the study.
Eighty-two serum samples from patients treated with other disease-modifying treatments were collected on a Friday between March and May 2015. These patients were seen in Dr. C.P. MS Clinic for regular check-up visit and therapy prescription. None of these patients had been exposed to natalizumab. Less than 5% of the invited patients refused to participate in the study.
The MS patients without prior exposure to natalizumab are representative of the demographic population with MS seen at Sant'Andrea Hospital. The natalizumab-treated MS patients are controls for drug use and disease severity, the main indication for treatment with natalizumab.
Informed consent was obtained from all patients participating in the study. The study was approved by the Sapienza University IRB.
Serological methods
The serum samples were tested in virus-like particles (VLPs)-based ELISA assays for antibodies to JCPyV and BKPyV serotype 1 and 4 capsid antibodies, as described previously (16). Briefly, serum samples were tested in wells of a microtiter plate coated with 50 ng of JCPyV, BKPyV serotype 1, or BKPyV serotype 4 virus-like particles. Virus-like particles were produced in the laboratory of Dr. R.V. as previously described (1,22). Serum samples were diluted 1:100 or 1:200 to measure JCPyV and BKPyV seroreactivity, respectively. The assay was performed in duplicate and the log-transformed geometric mean of the two measurements was used for statistical analysis. A cutoff value for seropositivity was defined as an optical density (OD) value greater than the mean plus 3 standard deviations (SD) of the reactivity of serum samples from a low-prevalence population, children 2–5 years of age, after excluding outliers. Previously tested, known seropositive and seronegative serum samples from our laboratory repository were used as internal standards in each run of the assay. If the reactivity of these samples fell outside an acceptable range (>2 SD from the established mean), the run was repeated. The JCPyV and BKPyV serotype 1 assays were previously validated (20,15).
Data analysis
The distributions of JCPyV and BKPyV serotype 1 and 4 antibody levels by case–control status were displayed by boxplots. Wilcoxon rank-sum test was used to assess differences in the distribution of age, expanded disability status scale (EDSS), and duration of MS between the two control groups. Fisher's exact test was used to examine gender difference in the two control groups. Linear regression models on log-transformed antibody levels (outcome) were used to examine the association between antibody levels and PML case–control status. Separate univariable and multivariable linear regression models (adjusted for age and sex) were performed for each antibody. Regression coefficients were exponentiated to get the ratio of the expected geometric mean of the original antibody levels comparing cases and controls. Pearson correlation was used to examine the correlation between JCPyV and BKPyV OD values, stratified by case–control status. All analyses were done using SAS 9.4 (SAS Institute, Cary, North Carolina). Boxplots were created using Splus software (TIBCO Spotfire S+® 8.2, TIBCO Software, Inc.).
Results
The case group was composed of 10 patients, including 6 females and 4 males, with an average age of 39.10 years (SD 8.198). The patients had received an average of 37.10 (SD 19.44) natalizumab infusions. Four of the 10 patients in the case group had used an immunomodulatory drug before starting therapy with natalizumab. The blood samples for antibody testing were taken at various times between 3 days before and 322 days after PML diagnosis based on the time that the patient was first seen at the referral hospital. Blood samples from control MS patients receiving natalizumab were obtained after the patient had initiated drug therapy. The number of infusions ranged from 1 to 95 (median, 34 infusions, interquartile range [IQR], 25–51 infusions), Among the control groups, the patients treated with natalizumab (drug control group) were significantly younger (median 37 vs. 40 years old, p = 0.049), had an higher EDSS (median 2.5 vs. 1.5, p = 0.033), and had been diagnosed with MS for a longer time (median 12.3 vs. 8.3 years, p = 0.002) than the patients never exposed to natalizumab (no drug control). No significant difference was found in the two control groups in the proportion of males and females (Table 1).
EDSS, expanded disability status scale.
MS, multiple sclerosis.
The distribution of antibody levels against viral capsids of JCPyV, BKPyV serotype 1, and BKPyV serotype 4 by case–control status is shown in Figure 1. Among the PML cases, the median JCPyV antibody level was 1.575 OD units (IQR, 1.131–1.937). In contrast, the median antibody level in the controls never treated with natalizumab was 0.330 OD units (IQR, 0.108–0.872) and that in the controls treated with natalizumab was 0.102 OD units (IQR, 0.053–0.479). The median level of antibodies against BKPyV serotype 1 was 0.346 OD units (IQR, 0.155–1.193) in the cases, whereas the level in the controls never treated with natalizumab was 0.786 OD units (IQR, 0.219–1.409) and that in the controls treated with natalizumab was 1.108 OD units (IQR, 0.544–1.420). The median level of antibody against BKPyV serotype 4 in the three groups was similar, 0.326 OD units (IQR, 0.136–0.736) in the case group, 0.333 OD units (IQR, 0.132–0.715) in controls never treated with natalizumab, and 0.397 OD units (IQR, 0.208–0.688) in the controls treated with natalizumab.
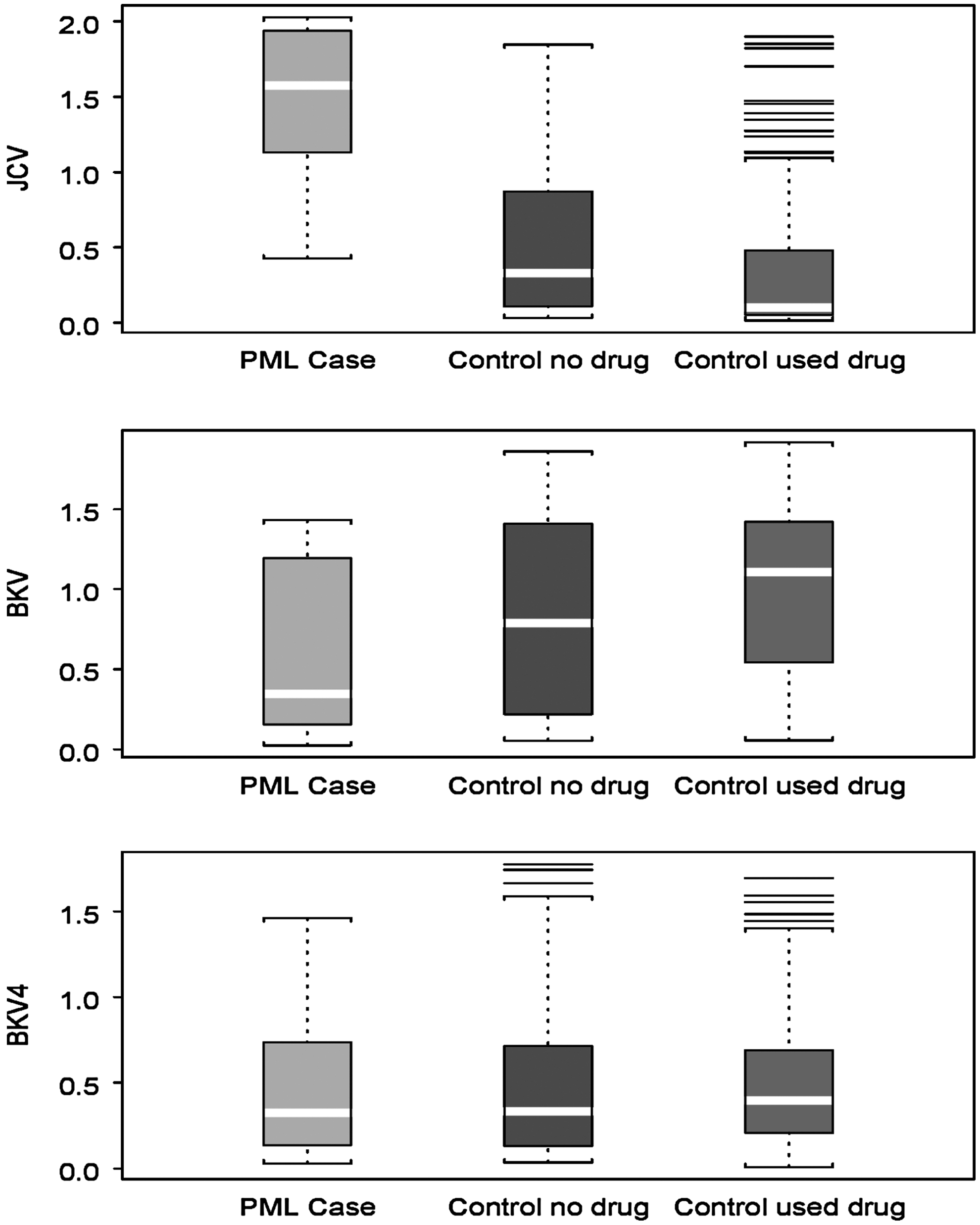
Boxplot of antibody level by PML case–control status. Distribution of optical density values to JCPyV, BKPyV serotype 1, and BKPyV serotype 4 virus-like particles. The upper boundary of the box represents the 75th quartile and the lower the 25th quartile. The central clear line represents the median value. The lines outside the boxes and within the bracketed area represent the 10th and 90th percentile, whereas the outside lines represent outlier values (<10th percentile or >90th percentile). PML, progressive multifocal leukoencephalopathy.
In a sex- and age-adjusted linear regression model, the JCPyV antibody level was significantly higher in cases compared with controls treated with natalizumab (expected ratio [95% confidence interval (CI)] = 9.1 [4.0–20.0], p < 0.001) and to controls never treated with natalizumab (expected ratio [95% CI] = 4.5 [2.0–10.0], p < 0.001), as expected given the robust JCPyV antibody response induced by PML. In a sex- and age-adjusted linear regression model, the BKPyV serotype 1 antibody level was significantly higher in the natalizumab-treated controls (expected ratio [95% CI] = 2.2 [1.2–3.9], p = 0.009) compared with the cases. The BKPyV serotype 1 antibody level was also higher in controls never treated with natalizumab compared with cases, but the difference did not reach statistical significance (expected ratio [95% CI] = 1.5 (0.9–2.8], p = 0.158). No significant differences were found between the control groups and cases for BKPyV serotype 4 antibody level.
Consistent with previous reports in the literature, we found a weak negative correlation between BKPyV serotype 1 and JCPyV log-antibody level among controls (Pearson's R = −0.1628, p = 0.018).
Discussion
PML is a rare disease even among patients with a predisposing condition. For patients treated with natalizumab, the risk is slightly increased by duration of therapy and by prior treatment with immunosuppressive drugs. Additionally, JCPyV seropositivity is a strong risk factor (7,14), consistent with exposure to the virus being a necessary, but not sufficient, cause of PML. However, JCPyV seropositivity is not simply a measure of exposure because JCPyV infections have been detected by PCR in seronegative individuals (5) and the level of antibody is a risk factor for PML (14). Because JCPyV and BKPyV seroreactivity are inversely correlated (6,8,10) and high JCPyV antibody levels are associated with an increased risk of PML, we reasoned that low BKPyV antibody levels may be associated with PML. In fact, our study demonstrates an association between low levels of capsid antibodies to BKPyV serotype 1 and a PML diagnosis and raises the intriguing possibility that high levels of BKPyV serotype I antibody may be associated with a reduced risk of PML, as we previously reported for HIV-associated PML.
If a high level of BKPyV antibody is a marker of reduced risk of PML, a primary antibody-mediated mechanism for the risk reduction seems unlikely because JCPyV and BKPyV are serologically distinct viruses (20). Additionally, since seropositivity to both JCPyV and BKPyV is very common in adults, it is unlikely that prior infection with one virus is protective against infection with the other virus (21). Conceptually an antibody-mediated mechanism is also unlikely because PML is caused by reactivation of a latent or persistent JCPyV infection. Classically, antibodies are believed to limit the spread of virus, but are not able to eliminate virally infected cells and clear an established infection. However, cross-reactive antibodies have been described (20), and low titers of JCPyV antibody are not specific, as demonstrated by failure of some low-titer sera to be competitively inhibited by preincubation of sera with JCPyV capsids (7). Thus, the presence of low levels of JCPyV cross-neutralizing antibodies in the sera of individuals with high BKPyV antibody titers cannot be entirely excluded.
An alternative explanation for an association of high BKPyV antibody levels with reduced risk of PML would be a cross-protective cellular immune response induced at the time of the primary infection that is correlated with the level of BKPyV antibodies. Although it remains to be formally demonstrated, individuals who mount a robust humoral immune response to a primary polyomavirus infection may also develop a robust cellular immune response. Thus, the antibody response would be a biomarker for a reduced risk of PML, but not the causal explanation for protective immunity. Cross-reactive T cell epitopes in the VP1 proteins of BKPyV and JCPyV have been experimentally demonstrated (11). Additionally, the viruses share ∼85% identity at the amino acid level, allowing for the possibility of many shared T cell epitopes. A bioinformatics analysis of putative HLA-A*02-restricted T cell epitopes shows that the majority of hits are epitopes with identical amino acids between the BKPyV and JCPyV proteome (data not shown). A cross-reactive cellular immune response induced by a BKPyV infection would not be expected to protect against acquisition of a JCPyV infection, but it could contribute to control of the spread of a JCPyV infection and the size of the reservoir of latent or persistent infection, and thus reduce the risk of reactivation. To test this hypothesis, future studies should measure antigen-specific T cell responses to BKPyV and JCPyV in prediagnostic blood samples from PML cases and controls, and perform fine mapping of epitopes to determine whether they are shared between the viruses.
As compared with previous studies of JCPyV capsid antibody responses in MS patients (18), in our cohort we found a lower JCPyV antibody level in natalizumab-treated patients compared with drug unexposed patients. These results may reflect selection for low responders in this group because some patients who chose to take natalizumab were seronegative in the commercial JCPyV ELISA, STRATIFY™.
In our previous study of HIV-associated PML and BKPyV capsid antibody responses, we observed an association of protection against PML and high levels of antibody to both BKPyV serotype 1 and 4, but in the current study there was no association with BKPyV serotype 4 antibody level (3,16). The explanation for this is unclear, but may reflect differences in population-based exposure to the different serotypes. BKPyV serotype 1 is the most prevalent serotype worldwide and BKPyV serotype 4 the second most prevalent serotype. While both are expected to be common in Italian populations, the serotypes can be further divided into subgroups. The VLP for the ELISA assay was constructed using the VP1 amino acid sequence of a subgroup c1 strain of BKPyV serotype 4 (MMR29), the predominant subgroup in Asia, whereas subgroup c2 is more prevalent in Europe, including in Rome, Italy (4,13). The VLP-based ELISA detects serotype-specific and cross-reactive epitopes, further complicating interpretation of differential responses to the two viruses. The family of BKPyV viruses is composed of multiple serotypes. A more detailed analysis of serotype-specific responses and the risk of PML may be informative.
In this study we confirm previous reports of a weakly negative correlation between BKPyV serotype 1 and JCPyV antibody levels (6,8,10). Cross-protective cellular immunity may provide an explanation for this correlation. Age seroprevalence studies suggest that exposure to BKPyV serotype 1 occurs before that to JCPyV (21). Individuals exposed to JCPyV following a BKPyV infection, which is associated with a robust BKPyV antibody response and by extension of a broad cellular immune response, would be expected to have a mild JCPyV infection, because cross-protective cellular immunity would limit the spread of the virus. Viral antigen load in these individuals would be low and consequently they would produce a low level of antibody to JCPyV, giving rise to a negative correlation between JCPyV and BKPyV antibody levels.
Our study has limitations. The sample size for PML cases is small and restricted to one geographic region. Because serum samples were obtained at various times after the diagnosis of PML, we cannot be certain that patients who developed PML had low BKPyV antibody titers before diagnosis. These limitations reflect the rarity of the disease, the variable clinical course of PML, and delays in referral to academic centers. The findings will need to be replicated in studies using prediagnostic serum samples as we previously did for HIV-associated PML. Although urinary secretion of JCPyV is not a risk factor for PML and BKPyV shedding is rare in healthy individuals, future studies should measure urinary viral load to examine correlations between antibody titers and viral shedding. We also note that because of the variability in seroreactivity to BKPyV capsids, antibody levels have low sensitivity and specificity for PML and are unlikely to be diagnostically useful in a clinical setting.
Footnotes
Acknowledgments
The research was supported in part by funding from Biogen Idec (RPV). Part of the information in this article has been presented at the Emerging Oncogenic Viruses Meeting in June 2016 at San Pietro in Bevagna, Italy and at ECTRIMS 2016 Meeting in September 2016 in London, United Kingdom.
Author Disclosure Statement
Dr. R.V. has a pending patent application for BKPyV serology as a predictor of risk of PML. Dr. R.V. received funding from Biogen Idec to supply the company with BKPyV capsids and to perform quality control ELISA testing for BKPyV antibody reactivity. Dr. C.P. has served on the Scientific Advisory Boards for Novartis, Merck, Biogen, Sanofi, Genzyme, Admiral, Teva, and Bayer, and has received funding for travel and speaker honoraria from Sanofi, Biogen, Bayer, Teva, Merck, Admiral, Genzyme, Actelion, and Novartis, and receives research support from Novartis, Merck, Biogen, and Sanofi. Dr. L.P. declares consulting fees from Biogen and Novartis; speaker honoraria from Biogen, Genzyme, Novartis, and Teva; travel grants from Biogen, Genzyme, Novartis, and Teva, and research grants from the Italian MS Society (Associazione Italiana Sclerosi Multipla) and Genzyme. Dr. L.P. also acts as member of the steering committee AIFA (Agenzia Italiana del Farmaco) on natalizumab. None of the other authors has financial associations that pose a conflict of interest.