
Abstract
Over the years, dengue fever has become a significant infectious disease in different parts of the world. Medical and public health services have been unable to deal with infection as there is no vaccine available for the prevention of this infection. With dengue, effective treatments are not available due to which severe symptoms may develop. To deal with this challenge, a sensitive and specific technique is required for its early diagnosis along with the knowledge of dengue serotype to increase the specificity of diagnosis and treatment. This study was designed to check the usefulness of immunological and nucleic acid-based molecular determination of dengue virus. The study recommends polymerase chain reaction as a suitable method for the rapid detection of dengue virus as it was found more sensitive than other utilized techniques, including antibodies detection. Nucleic acid analysis may also help to define the common serotypes/genotypes of dengue virus circulating in any region.
Introduction
D
A total of 513 blood samples were collected during Dengue outbreak 2011–12 from patients admitted at different hospitals of Lahore such as Lahore General Hospital, Sheik Zaid Hospital, Mayo Hospital, and Ganga Ram Hospital. All the patients included in the study were informed about the objectives of the research. A signed consent was taken from them before collecting blood samples. This study was conducted in accordance with the 1964 Declaration of Helsinki and Guidelines for Good Clinical Research Practice in Pakistan. The study was approved by the Ethics Committee of University of the Punjab, Lahore, Punjab. Hundred microliters of samples was used to detect dengue IgG and IgM using kits from Calbiotech USA according to manufacture's protocol. Both positive and negative controls were run alongside the samples. Viral RNAs of these samples were isolated from 150 μL of serum sample using Viral RNA Extraction Kit (Favorgen Biotech Corp., Taiwan). Both the complementary DNA and amplification of C-prM gene junction were carried out by our routine methods employed in the laboratory as described (5).
Since these samples were collected during the epidemic of dengue virus in our region, 498 of these samples were positive for dengue virus through polymerase chain reaction (PCR) and/or enzyme-linked immunosorbent assay (ELISA)-based detection. Data of these 498 samples were further evaluated for this study. According to our study, prevalence of dengue infection was high in males (67%) than in females (33%), showing that males were at greater risk of acquiring DF. This keeps the ratio at 2:1 for male to female as already reported from Pakistan (4).
Among these 498 samples, 480 (96.38%) samples were positive with serotype-2 only whereas 18 (3.61%) samples were coinfected with serotype-3 as confirmed by PCR. Our samples had 100% prevalence of dengue serotype-2 infection as also reported by Idrees et al. (7). DF, the emerging vector-borne disease, is at its peak in different parts of world, mainly distressing tropical regions. Pakistan is no exception. Since 2006, Pakistan has also been severely affected by the dengue virus and many severe outbreaks have been seen during the past few years. Serotype-2 remains the main agent of dengue infection with serotype-3 also being detected in patients (5). We could not find any case of dengue infection by serotype 1 or 4 in our samples.
Out of these 498 samples, 18 samples (3.61%) were positive only by ELISA but negative by PCR. Upon inquiry we found out that these patients felt fever due to other causes after 10–48 days of initial dengue symptoms and visited hospitals. Their negative PCR and positive ELISA tests could be due to the presence of antidengue IgM which may stay in the blood 2–3 months after dengue infection. Viral RNA can be isolated from day 1 of postinfection till 7–8 days. A positive PCR test is always an indication of current dengue infection, so these 18 samples show that patients had dengue infection and the virus was cleared from the blood at the time of PCR test. The antigens used for ELISA were derived from the envelope protein of the virus. One of the limitations of this testing is the cross-reactivity between other circulating flaviviruses. This limitation must be considered when working in regions where multiple flaviviruses cocirculate. Antidengue IgM detection may not be 100% useful for dengue serotype determination due to cross-reactivity of the antibody (3). In contrast to this, we detected viral RNA from 37 samples through PCR but these samples were negative for anti-IgM or IgG. The viral RNA can be isolated from day 1 of postinfection till 7–8 days. Hence PCR result is definitive for detection of dengue virus in blood of a patient.
Two hundred and sixty-five samples were positive with both antidengue IgM and PCR. One hundred and one samples were antidengue IgG and viral RNA positive (Fig. 1). The result with negative antidengue IgM may be due to compromised or low sensitivity of the ELISA-based test, which was used to perform IgM tests. According to the Pan American Health Organization guidelines, 80% of all dengue cases have detectable IgM antibodies by day 5 of illness, and 93–99% of cases have detectable IgM antibodies by days 6–10 of illness, which may then remain detectable for >90 days (3). Seventy seven samples were positive with both, ELISA antidengue IgM/IgG and PCR.
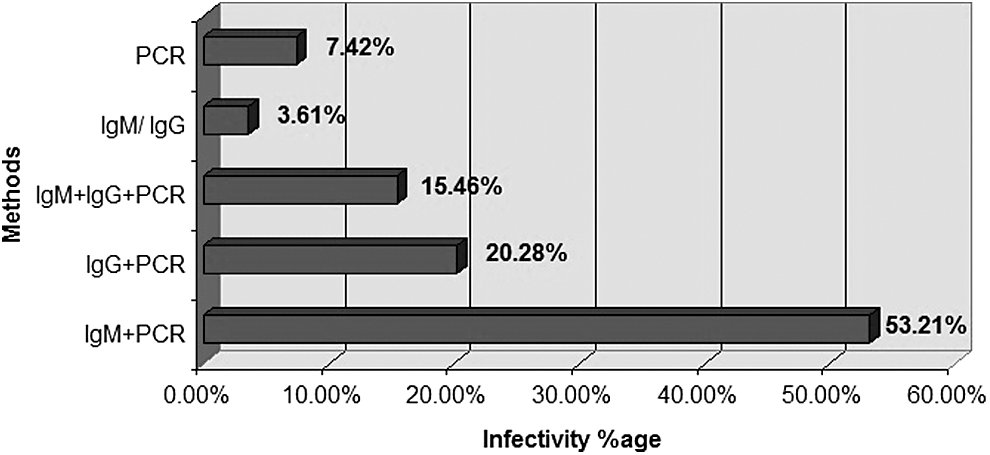
Infectivity percentage of dengue positive samples through enzyme-linked immunosorbent assay (antidengue IgM and antidengue IgG) and polymerase chain reaction (PCR).
Dengue virus was detected in more samples through PCR than through ELISA. Also, ELISA can give false positive results because it can detect antibodies that are generated in a 2- to 3-month-old infection. This false positive result can be misleading in treatment during epidemics. PCR always give positive results in current infection. A major concern in diagnosing dengue virus through the PCR-based method is the genetic variation in nucleotide sequences among the studied viruses. To solve this problem, degenerate primers that encompass all possible permutations are used to study same gene in different organisms. That is why we employed degenerate primers made for capsid-premembrane region of dengue virus (5). Evolutionary background of the sequenced serotypes and genotypes was studied by using dendograms that were drawn for these sequences (data not shown). These evolutionary studies can be performed only if the dengue gene is amplified through PCR. These results summarized together show that the PCR-based detection is a more reliable, sophisticated, suitable test with high sensitivity and specificity to detect dengue infection than ELISA.
Footnotes
Acknowledgments
The authors thank all the patients and clinicians who helped with sample collection.
Authors' Contributions
Z.F., M.I., and A.S.H. conceived the study. K.I. and Z.F. carried out the experiments. K.I., Z.F., and S.S. wrote the article and present the results. All authors approve the article.
Ethical Approval
The study was approved by the Ethics Committee of Molecular Virology Division of the University of Punjab. Informed consent was obtained from each participant (aged >18 years) or head of family (for patients aged <18 years) in accordance with the Declaration of Helsinki.
Author Disclosure Statement
No competing financial interests exist.