
Abstract
Varicella zoster virus (VZV) is the cause of chickenpox (varicella) and shingles (zoster), and was once responsible for over 4 million infections in the United States annually. The development of a live attenuated VZV vaccine was initially viewed with extreme skepticism. Nonetheless, a VZV vaccine was developed in the 1970s by Takahashi and his colleagues in Japan and was eventually licensed in the US. It is now known to be one of the safest and most effective vaccines available and is administered worldwide. Here are described important factors that contributed to the successful research and licensure of the highly successful VZV vaccine.
Introduction
V
Live attenuated varicella vaccine was developed in the 1970s by Takahashi and his colleagues in Japan (21,55,56). The success of this vaccine there, tested in small numbers of children and adults, led to its eventual further exploration and licensure in the United States, where many more individuals were vaccinated in numerous clinical trials (22,59,63). It is now known to be one of the safest and most effective vaccines available and is administered worldwide. One aspect to its success in the United States is that the immunization rate in healthy children is now over 90%, which has likely led to a high degree of herd immunity. So far, it is the only herpesvirus for which a vaccine has been developed.
After primary infection, VZV establishes latency in sensory (dorsal root, cranial nerve, and autonomic including enteric) ganglia (3,24). Latency in ganglia can occur after infection with wild-type (WT) VZV or less frequently following vaccination due to the vaccine strain VZV (24,61). Reactivation of VZV infection leads to herpes zoster (HZ), a condition classically manifested by a vesicular unilateral dermatomal rash that may include itching or pain, paresthesias, and allodynia (8,28,46). HZ can also occur in the absence of rash, in which case it may be difficult to recognize (8,25). Recently, it was realized that HZ can occur in the gastrointestinal tract and cause diseases such as pseudo-obstruction and ulcers (25). HZ is also associated with strokes and various forms of arteritis (2,46). HZ occurs most commonly after primary varicella among naive individuals, but has been described among vaccinated people due to reactivation of wild and vaccine strain virus (61). Postherpetic neuralgia (PHN) is its most significant and debilitating complication and was the main reason for the development of vaccines against HZ (3). Reactivation of VZV occurs especially in aging individuals who lose cell-mediated immunity to VZV and in the immunocompromised (3).
Clinical Manifestations of Varicella
Before the widespread use of live attenuated varicella vaccine, varicella caused over 4 million annual infections in the United States (23), leading to 11,000–13,500 hospitalizations and 100–150 annual deaths (62). Varicella is typically a childhood illness and its severity is increased when it occurs in adulthood. The infection is highly contagious with household attack rates averaging 80%, making it somewhat less contagious than measles (23). The infection is transmitted from person to person via the airborne route. The source of infectious VZV is primarily from skin vesicles containing numerous virions (15). Common manifestations of varicella include a self-limited generalized pruritic vesicular rash in varying stages of development, predominately on the face and trunk, characteristic features helping to distinguish the rash from other exanthems. Systemic symptoms, that is, fever, are usually mild. Serious complications are uncommon and can affect any organ. Bacterial superinfections leading to bacteremia and sepsis, pneumonia, encephalitis, stroke, acute cerebellar ataxia, glomerulonephritis, arthritis, hepatitis, and thrombocytopenia are serious complications of VZV infection and are not limited to individuals with underlying medical conditions (3,23). The infection is often more severe among immunocompromised individuals in whom it may be fatal if untreated (3,23). To some extent, the burden of the disease is economic, due to a need for parents to take time off from work during their child's illness. The unpredictability of serious complications especially in otherwise healthy children poses yet an additional problem (13). A rare often serious congenital varicella syndrome follows ∼1–2% of pregnancies when varicella occurs in the first or second trimester (19).
Treatment
Varicella is usually a self-limited illness in otherwise healthy children. Treatment is especially recommended for patients at high risk to develop serious VZV infections such as those with conditions compromising their immune system (cancer, use of immunosuppressants, extremes of ages). Acyclovir or valacyclovir may also be given to otherwise healthy patients who develop varicella to facilitate recovery. In addition to antivirals, another therapeutic intervention includes varicella zoster immune globulin for postexposure prophylaxis. Acyclovir (or valacyclovir) is most commonly given for varicella due to reasons of safety and tolerability; foscarnet (which is more toxic) is reserved for VZV resistant to acyclovir. Antivirals are most effective when used early in the course of the disease (within 72 h of the onset of the rash) (1). Antivirals have a limited role once disease is established except among immunocompromised individuals where viral replication can be prolonged. Immune globulin is used in the prevention of VZV infection among high-risk patients who are susceptible to varicella but it has no role once infection is established (10,23). Varicella zoster immune globulin is currently available in the United States as VariZIG, which must be ordered from FFF Enterprises, Temecula, CA. If for some reason VariZIG is not available, intravenous immunoglobulin (IVIG) may be used instead. Further details on therapy and prophylaxis are given in the Report of the Committee on Infectious Diseases (The Red Book) of the American Academy of Pediatrics.
The diagnosis of varicella and HZ can usually be made clinically, due to the characteristic appearance of the rash. If laboratory diagnosis is indicated, it is best made by either polymerase chain reaction (PCR) or direct immunofluorescence on swabs of skin lesions. These results may be available within 1–2 days (23). The diagnosis may also be made by testing saliva specimens for VZV DNA by PCR (39). Viral culture is rarely used today because it is not only time-consuming, and expensive, but also less sensitive than PCR. Antibody testing on acute and convalescent sera is usually too time-consuming to be useful diagnostically (23).
Immune Responses to VZV
VZV virus induces robust humoral, secretory (nasopharyngeal), and cellular immune responses in healthy persons. Innate, humoral, and cellular immune responses are important in the control of VZV infection (26). Cellular immunity is important in the resolution of VZV infection, induction of immune memory, and prevention of symptomatic reactivation (23).
Humoral responses
Serologic tests may be used to assess immunity to varicella; persons who develop HZ invariably have detectable VZV antibodies at the time of onset, which also indicates that antibodies do not protect against this form of VZV infection. As mentioned, serologic tests are rarely useful for diagnosis of varicella or zoster. An exception is a scenario of a positive VZV IgM and a significant rise of VZV IgG consistent with varicella in a previously unvaccinated individual. Both serum VZV-specific immunoglobulin IgG (IgG) and IgM antibodies are detectable following varicella or zoster and hence are not useful in differentiating between primary infection and reactivation. IgM and IgA are detectable within a week after the onset of symptoms of varicella. Serum IgG was detected among 100% of healthy adults for years after clinical varicella using the highly sensitive method, VZV fluorescent antibody to membrane antigen (FAMA) assay (64). Following varicella, serum VZV IgG presumably plays a role in neutralizing virions at the site of inoculation to protect against new infections with VZV.
Historically, a variety of assays were used to measure immunity to VZV infection or seroconversion after vaccination. Those assays included FAMA, latex agglutination (LA) assay, and enzyme-linked immunosorbent assay (ELISA). FAMA is considered a gold standard, but it is now rarely performed. Kits for LA are no longer commercially available (23). Many commercial manufacturers market ELISAs, but none has been found to be as sensitive as FAMA for determining immunity to varicella, especially after vaccination. In one ELISA study, its sensitivity for VZV antibodies was less than that of FAMA and its specificity was fair, 74% and 89%, respectively (51). An assay known as gp ELISA was developed at Merck & Co. in the 1980s, and is currently being used in laboratories at the Centers for Disease Control and Prevention (CDC); its exact antigenic composition is proprietary and unpublished, and the test tends to over read immunity to varicella. For example, in the early years of study of varicella vaccine testing, vaccine-induced immunity was overestimated by this assay, supporting the idea that one dose of varicella vaccine would suffice for protective responses (45). Although a direct comparison of FAMA and gp ELISA was never published, it appeared that FAMA titers gave a more meaningful indication of immunity after vaccination than gp ELISA (45). It became clear that one dose of varicella vaccine resulted in only 85% protection from disease, which, in the late 1990s, was not being well controlled in schools where numerous outbreaks were occurring among vaccinated and unvaccinated children (23). At the same time, a study of FAMA titers in vaccinated children resulted in only 76% seroconversion (45). To address these problems, in 2006, two doses of vaccine were recommended for routine use in the United States (44), and varicella began to come under good control marked by decline in varicella-related outpatient visits and hospitalizations (see Vaccine Effectiveness and Postlicensure Vaccine Efficacy and Effectiveness sections).
Cell-mediated immunity
Varicella and vaccination induce long-term T lymphocyte-mediated immune responses, which participate in protection from further VZV clinical infection. Glycoprotein E (gE) of VZV is the most abundant and immunogenic viral glycoprotein. Both CD4+ and CD8+ T lymphocytes are engaged in responses to VZV, and gE-specific CD4+ T cells play a key role in the control of viral replication (43). Cell-mediated immunity is important in recovery from VZV infection and in controlling the balance between latent infection and reactivation. Lasting memory is likely furthered by endogenous re-exposure from subclinical (or clinical) VZV reactivation and from exogenous exposure to varicella or HZ (Fig. 1) (31). Immunity to varicella is commonly maintained for decades, aided by periodic boosting of the immune response, as varicella usually confers lifelong protection (23). Persistence of laboratory immunity to varicella for more than 20 years postvaccination has been demonstrated (4). Details regarding long-term protection against HZ are not well understood, but it is thought to be unusual for HZ to recur, although in some individuals it may do so (23).

Diagram of VZV infection illustrating time, immunity, and zoster following onset of varicella in childhood. Boosts in immunity occur after exogenous re-exposure to VZV and also after periodic reactivations (which are often asymptomatic) of the virus over time. With increasing age, immunity fails to control reactivating VZV, resulting in clinical zoster. Zoster then further boosts immunity. VZV, varicella zoster virus.
Varicella Vaccine
The development of live attenuated varicella vaccine was initially challenged by extreme skepticism on the part of some (11,12,49). The possibility that the incidence of zoster might increase following vaccination was feared. Possible long-term complications of vaccination with a virus that causes a latent infection were unknown. There was serious concern that young vaccinated adults would end up with severe varicella if they lost immunity some years following childhood vaccination, since varicella is known to be more severe in adults than in children. Unfortunately, there was no animal model in which to test the attenuation and behavior of the vaccine virus as was done previously for measles vaccine.
Live attenuated varicella vaccine was licensed in the United States in 1995, and endorsed by both Advisory Committee on Immunization Practice and American Academy of Pediatrics for single-dose, universal vaccination of all healthy children 1–13 years of age and healthy adults (13). Due to numerous varicella outbreaks among immunized school children in the 1990s, however, and the realization that one dose might not provide even 80% seroconversion rates, a routine two-dose schedule was adopted in 2006 (44). The United States was the first country to recommend universal VZV vaccination. Its use lead to a dramatic decline of varicella and its complications, hospitalizations, and deaths (5 –7,41) (Fig. 2). Although its use was initially highly controversial, it is now widely accepted as safe and effective and universal vaccination has been adopted by many other countries around the world. Two vaccines containing varicella virus are licensed for use in the United States: VARIVAX® the single-antigen varicella vaccine and ProQuad®, a combination measles, mumps, rubella, and varicella (MMRV) vaccine. Both vaccines contain live, attenuated, varicella zoster virus derived from the Oka strain. Varicella vaccine also continues to be produced in Japan, and it is also manufactured in China and South Korea (23).
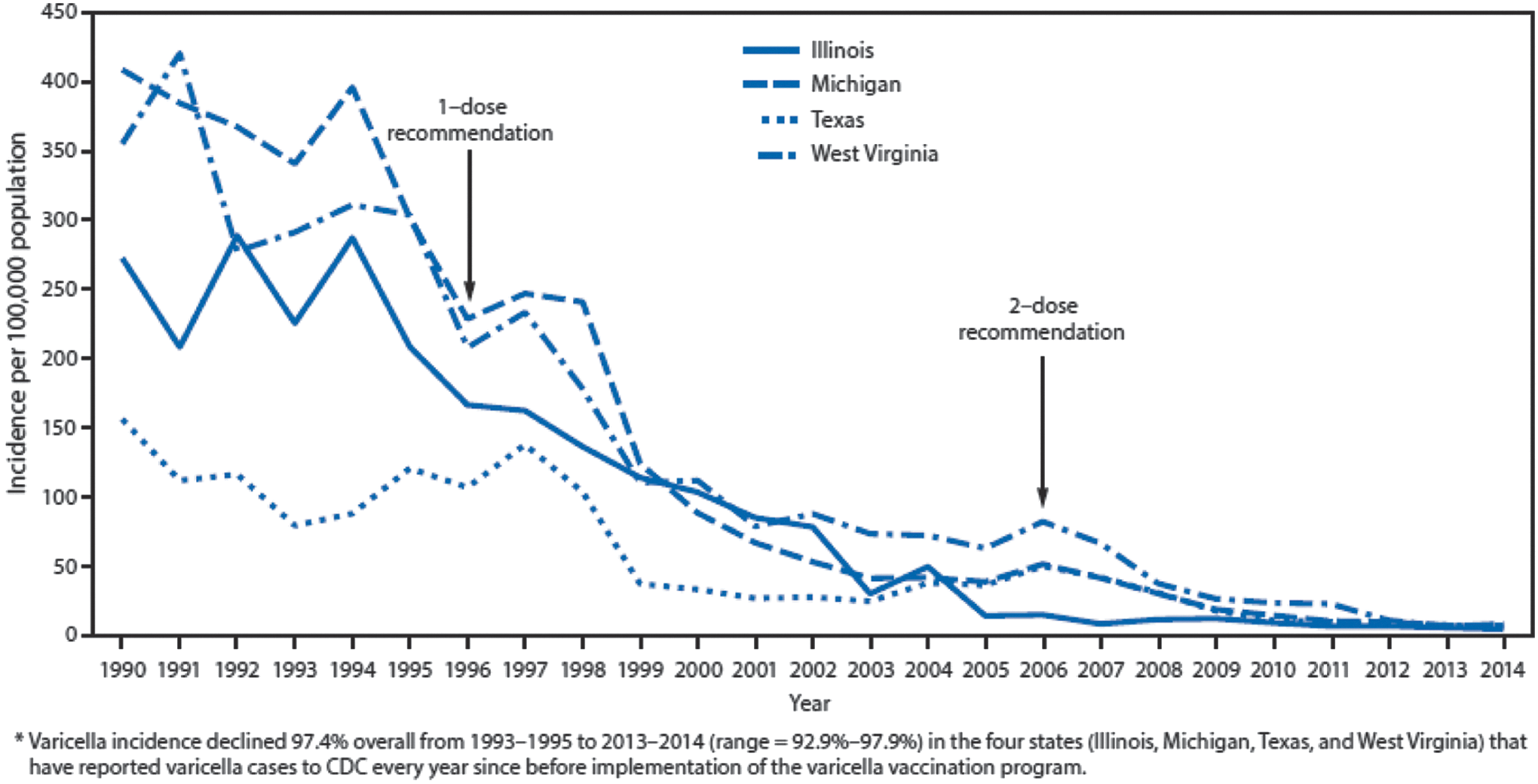
Varicella incidence per 100,000 population* in states that have reported varicella cases to CDC annually before implementation of the varicella vaccination program—Illinois, Michigan, Texas, and West Virginia, 1990–2014. Source: Lopez et al. (41).
The Oka vaccine strain
What became the first VZV vaccine strain was originally isolated from a Japanese patient with chickenpox, a 3-year-old otherwise healthy boy whose family name was Oka. The virus was attenuated through multiple passages (about 33) in human embryonic lung fibroblasts followed by a few passages in guinea pig fibroblast cells, and eventually final passages in WI-38 human diploid cells and MRC-5 human diploid cells (55,56). The Oka vaccine strain is the main strain used in single-antigen and combination varicella vaccines throughout the world. The Oka and WT VZV strains have been fully sequenced and differences have been identified, although the exact sequences responsible for attenuation have not yet been identified. Sequence differences, especially in the ORF62, are probably responsible for attenuation; identification of these sequences also assists in laboratory differentiation between WT and vaccine strains (23,65).
Reversion from vOka to WT VZV is a theoretical possibility but there is no clinical evidence that vOka reverts to WT VZV. It seems unlikely that reversion will occur because of the complicated and numerous simultaneous changes in the virus that are probably required to regain virulence. The VZV genome, which varies by no more than 0.1% between any two WT strains (40), is extremely stable. A study of a WT isolate showed that few changes occurred in tissue culture across 72 passages (48). Such changes are even less likely to occur within the infected host, to which environment the virus is ideally adapted. There is no evidence for reversion of these markers among isolates in the vaccine; although a small subset of the vaccine viruses may contain one of the Oka-specific WT markers in ORF62, there have been no isolates identified using thymine–adenine cloning and sequencing that contain all of the “fixed” vaccine markers as WT (50,57). Although recombination between WT VZV and vOKA was described in vitro (18), such virus has not been demonstrated in vivo.
Rationale for vaccine development
Burden of the disease
Before implementation of varicella immunization program in the United States, there were an estimated 4 million annual cases of varicella, leading to an annual average of 11,000–13,500 hospitalizations and 100–150 deaths (60). Most deaths occurred in otherwise healthy individuals. Natural infection usually confers lifelong immunity to varicella. The highest risk of death from varicella was among adults, which was 20–25 times higher compared to preschool aged children (20).
The live, attenuated varicella vaccine was developed in Japan by Takahashi (21,55). Initially tested in small groups of healthy Japanese adults and children, the vaccine appeared to be extremely safe and prevented transmission of varicella among household and hospitalized contacts. The vaccine was also safe when administered carefully to a small number of immunocompromised Japanese children, most of whom were in remission after undergoing treatment for leukemia (32). The results from Japan for this vaccine were truly compelling and could not be ignored, especially at a time when young American children were being successfully treated for leukemia only to risk dying from a disease felt to be as mundane as varicella (34).
Therefore, it was decided that varicella vaccine would first be tested in the United States among asymptomatic children with leukemia in remission and in healthy adults. It was felt that the risk/benefit ratio for varicella vaccine was more appropriate for these high-risk individuals than for healthy children; immunocompromised children and adults had more to gain and less to lose (if the vaccine proved unsafe) from vaccination than healthy children. The availability of the antiviral drug acyclovir made it possible to study the vaccine in immunocompromised children as they could be quickly treated if they developed fever or rash due to the vaccine strain or a severe breakthrough infection with WT varicella. In the collaborative study of varicella vaccine in children with leukemia in remission, there were no severe events necessitating intravenous acyclovir for such events (27). The encouraging findings from VZV vaccine trials in high-risk children led to exploration of vaccine safety and efficacy in healthy children (27).
One extremely important factor in the early studies of varicella vaccine in immunocompromised children was the availability of the FAMA test. Not only does the FAMA assay reflect neutralizing antibodies (29) but the test itself had been extensively evaluated clinically in individuals closely exposed to varicella as well. It was known that persons with detectable FAMA antibodies who were closely exposed to individuals with varicella had a less than 2% chance of developing very mild varicella (45). In contrast, those who lacked detectible VZV FAMA antibodies had approximately a 60% chance of developing varicella when exposed. Thus, in leukemic vaccinees with known positive FAMA titers and close exposures to their siblings, it was unnecessary to administer varicella zoster immune globulin (VZIG), because it could be predicted that the vaccine would protect them. From these studies in leukemic children, vaccine efficacy could be calculated and was shown to be about 85% after two doses (27). The few leukemic children who developed varicella despite vaccination had very mild cases that did not require antiviral therapy. The availability of therapy with acyclovir just in case a vaccinee developed a severe case of varicella was also critically important to the study of the vaccine in children with underlying leukemia. Importantly, the vaccine-induced immunity in these children lasted for years, for as long as they could be followed. In addition, the incidence of zoster in leukemic vaccinees was lower than that in leukemic children who had experienced natural varicella (30). These important findings led to great interest in exploring vaccination of healthy children on a routine basis.
Very rarely, leukemic children who were immunized less than a year after the diagnosis of leukemia (who were not in the above-described study) were reported to develop severe or fatal varicella from the Oka VZV strain (23). It was therefore realized that it would be safer to concentrate on universal vaccination of healthy children, with protection of immunocompromised children by herd immunity. That is the approach being used in the United States today. Varicella vaccine is not now recommended for immunization of immunocompromised persons, except possibly in carefully conducted research studies and in certain children with immunologically well-controlled HIV infection (23). Severe varicella in immunocompromised children is now a rarity, in large part, due to herd immunity.
Vaccine effectiveness
To measure seroconversion rates after vaccination of healthy children in early research studies, most investigators used primarily the gp ELISA, which, as mentioned, tended to overestimate the development of vaccine-induced immunity to varicella. In addition, protection against varicella disease was determined in vaccinees, and it was clear from many studies especially involving outbreaks that the vaccine was entirely protective in about 85% of vaccinees after one dose. One dose was highly protective against severe varicella. Little data are available using the highly sensitive and specific FAMA assay in healthy vaccinees from that era. In one later study, however, the FAMA seroconversion rate after one dose was a disappointing 76% (45). Significantly, after two doses of vaccine became standard, the rate of protection against varicella improved. Case–control studies involving healthy children indicated that protection from disease was 85% after one dose and 98% after two doses (52). In addition, and very importantly, these studies showed no evidence of loss of immunity to varicella with time (58). A more recent study confirmed that there was no evidence of waning of immunity following vaccination against varicella (5).
Postlicensure vaccine efficacy and effectiveness
Worldwide implementation of either a single- or two-dose VZV immunization program decreased the burden of VZV infection among both healthy and immunocompromised individuals. One dose of VZV vaccine lead to an 88% decline in varicella-related hospitalizations and a 59% decline in outpatient visits during 1994–2002 (38). The average annual incidence of varicella declined by almost 85% between 2005 and 2006 (just before two doses were recommended) compared with 2013–2014. The largest decreases in incidence rates were in children aged 5–9 and 10–14 years (41) (Fig. 2).
Although breakthrough infections sometimes occur in vaccinated individuals, the disease is usually mild and serious complications are extremely rare. A recent study documented 100% vaccine efficacy for one dose of VZV vaccine for prevention of moderate or severe varicella and 81% for prevention of all varicella (41). Not all of these children had received two doses. As the proportion of vaccinees who have had two doses increases with time, the protective effectiveness in the community is expected to increase.
The incidence of HZ among children with leukemia who received VZV vaccine was lower compared with those who had natural VZV infection (30). Recently, the incidence of HZ among healthy child vaccinees was also shown to be lower than that in similar children who had experienced chickenpox (61).
A question was raised by epidemiologists in the early years of the 21st century as to whether widespread use of varicella vaccine in a population would decrease the circulation of WT VZV, resulting in loss of immunity in middle-aged individuals, leading to an increase in the incidence of zoster (9). Fatal epidemics of zoster were projected by computer modeling (9). This unproven hypothesis has prohibited the licensure of varicella vaccine for children in the British Isles. Fortunately, however, this hypothesis has been largely rejected. There is no clinical evidence that universal use of varicella vaccine causes an increase in the incidence of HZ. There has been an increase in HZ incidence in the U.S. population, which began about 70 years ago, long before the development of varicella vaccine. Significantly, there was no uptick in the incidence noted after introduction of varicella vaccine in the United States. (33). The increase in zoster incidence is undoubtedly multifactorial and related to, for example, longer lifetimes, increasing numbers of immunocompromised individuals in our population, and stress, among other problems of modern society, but not to widespread use of varicella vaccine.
Postlicensure vaccine safety
Varicella vaccine is safe and well tolerated when administered to healthy persons. It has been marketed worldwide in 46 countries, with millions of doses distributed. Considering ∼48 million vaccine doses were distributed in the United States from 1995 to 2005, the most common adverse events reported included transient rash, fever, and injection site reactions, such as redness and/or discomfort. A small proportion (5.0%) of events were classified as serious such as transient meningitis (14). Given the large number of doses distributed worldwide, postmarketing adverse event surveillance systems can detect rare events. Serious adverse events that have been reported as temporally related to varicella vaccination, but not necessarily caused by the virus, include urticaria including some cases of recurrent papular urticaria, ataxia, thrombocytopenia, pneumonia, anaphylaxis, encephalitis, erythema multiforme, stroke, transverse myelitis, and death (14,23,53). VZV strain identification is critical in investigation of adverse events following vaccination (54). Rare complications that have been confirmed to be caused by VZV Oka strain include pneumonia, hepatitis, HZ meningitis, recurrent HZ, severe rash, and secondary transmission (14,23,53). Usually when serious adverse events were associated with inadvertent vaccination of immunocompromised individuals, these underlying problems were either inapparent or undiagnosed at the time of vaccination. Febrile seizures were reported with a slight increase in frequency after the use of MMRV vaccine (ProQuad) administered to children age 9 to 30 months compared with the group who received MMR and varicella vaccines separately with excess of one extra febrile seizure for every ∼2,700 children vaccinated with MMRV instead of separate MMR and varicella vaccines. The increased risk of febrile seizures was not observed among 4–6-year-old children receiving a second dose of combination MMRV vaccine (35,36).
An Institute of Medicine Report, Adverse Effects of Vaccines (2011), concluded that evidence supports causality in five adverse events: “(1) disseminated vaccine strain virus without organ involvement (e.g., varicella-like rash extending to dermatomes beyond the initial injection), (2) disseminated vaccine strain virus with organ involvement (e.g., pneumonia and meningitis) in individuals with demonstrated immunodeficiencies, (3) vaccine strain reactivation (HZ) without organ involvement, (4) vaccine strain reactivation (HZ) with organ involvement, and (5) anaphylaxis.” Adverse reactions to varicella in immunocompromised children who were vaccinated were also cited in an extensive review on vaccine safety in 2014 (42).
Zoster vaccines
The success of varicella vaccine led directly to the idea that the live attenuated vaccine might be used to increase cell-mediated immune responses in healthy elderly individuals and prevent HZ. Eventually, a formulation of the Oka strain 14 times as potent as varicella vaccine was developed, which safely and successfully prevented zoster in about 60% of healthy people older than 60 years (47). More recently, a noninfectious subunit vaccine composed of VZV glycoprotein E and an adjuvant that stimulates innate and adaptive immunity has been developed (17,37). This vaccine appears to have even greater efficacy in elderly people in preventing HZ and PHN, and is currently under consideration for licensure by the FDA.
The future
Complications of varicella that are less frequent today than before varicella vaccine was available are shown in Table 1. Reasons why it could be predicted that testing of varicella was likely to be successful and to result in a safe vaccine are listed in Table 2. Figure 1 diagrams immune responses to VZV following endogenous and exogenous exposure to VZV. It seems likely that a critical factor in maintaining immunity to VZV is due to latency of VZV, including the Oka virus, which periodically reactivates without symptoms to boost immunity to the virus. Latency of VZV may turn out to be to a great extent an advantage, and not the disadvantage that was initially feared. Figure 2 illustrates the decreasing incidence of varicella between 2000 and 2014.
Reference numbers are given in parenthesis.
VZV, varicella zoster virus.
Continued surveillance of the effects of varicella and zoster vaccines is warranted. Thomas Jefferson supposedly said that the price of liberty is constant vigilance. For VZV vaccines, the price of freedom from disease is a need to continue to monitor the behavior of the vaccines and the diseases caused by VZV as time goes on, to be certain that the success of these vaccines continues into the future.
Footnotes
Acknowledgments
Supported by the NIH grant R01DK093094 and the Biken Institute, Osaka, Japan.
Author Disclosure Statement
Dr. Gershon consults when invited for Merck and GSK. She has NIH funding to study VZV. No competing financial interests exist.