
Abstract
This longitudinal study focused on the relationship between lupus activity and the levels of intracellular proteins, phosphorylated interferon regulatory factor 7 (pIRF7), caspase-9 and -10, and mitochondrial antiviral signaling protein (MAVS) and melanoma differentiation-associated protein 5 (MDA5). Ten patients with systemic lupus erythematosus (SLE) were followed at clinics, and their disease activity indexes (SLEDAIs) were determined. Correlation analysis was used to test the influence of changes in intracellular markers on changes in SLEDAI score at two time points. All the patients were women with a median age of 43.5 years. Time to disease condition change varied from 30 to 283 days in this study (188.5 ± 74.31 days). The intracellular protein levels increased after regular follow-up and oral medication. Although there was a decreasing trend in SLEDAI scores in patients after regular follow-up and oral medication, the changes were not statistically significant. The statistical results were as follows: pIRF7 (r = −0.58, p = 0.04), MAVS (r = −0.587, p = 0.04), MDA5 (r = −0.914, p < 0.001), and caspase-10 (44 kDa) (r = 0.593, p = 0.04). The disease activity of SLE was inversely associated with levels of antiviral immunity. The antiviral immunity was represented with MDA5, MAVS, and pIRF7.
Introduction
S
Clinical studies showed that apoptosis of peripheral mononuclear cells is higher in active SLE patients than inactive SLE patients (15,27). On the contrary, overexpression of the BCL-2 gene was positively correlated with disease activity and inhibiting apoptosis (23). Furthermore, apoptosis can be initiated by either an extrinsic or an intrinsic process (10). The external apoptotic signal is executed through cell surface receptors with caspase-10 being the representative marker (10). Caspase-9 is known as an initiator caspase of the intrinsic apoptotic pathway (10,28).
Viruses have been shown to have a role in inducing lupus and lupus flares (3,8,11,26). It has been suggested that antiviral immunity could be defective in SLE patients (16,19). Clinically, viral infections can cause fever, oral ulcer, arthralgia, leukopenia, and even nephritis (12), which are similar to lupus disease flares. These symptoms in an SLE patient could then be a result of a viral infection or lupus disease flare. Nevertheless, the correlation between disease activity and antiviral immunity could be a hint of the relationship between viral infections and flares in lupus patients and could be used as a guide in clinical settings.
There are dozens of markers that could be activated during viral infection, and several of them are well-known antiviral immune pathways in humans (6), which all lead to interferon (IFN) activation and could be sorted into either RNA sensing or DNA sensing intracellular proteins, and all lead to mitochondrial antiviral signaling protein (MAVS) activation. According to Baños-Lara et al. (1), melanoma differentiation-associated protein 5 (MDA5) is critical in IFN response after viral infection in humans. Also in their study, the IFN regulatory factor 7 (IRF7) is critical in IFN activation in vivo. Combined altogether, along with our previous research (27), we condense our research into these few intracellular markers, especially MDA5 and IRF7.
The aim of this study was to evaluate the clinical correlation between SLE disease activity and antiviral immunity. To our knowledge, little is known about the relationship between apoptosis and antiviral immunity in patients with SLE. In this longitudinal study, we investigate the levels of phosphorylated IRF7 (pIRF7), caspase-9 and -10, and two intracellular proteins, MAVS and MDA5, to evaluate antiviral immunity and cellular apoptosis in lupus patients.
Patients and Methods
Study patients, clinical assessments, blood sampling, and timing
Ten female patients who had a definitive diagnosis of SLE and were treated at the Rheumatology Outpatient Clinic, Kaohsiung Chang-Gung Memorial Hospital for >6 months were prospectively evaluated and consecutively enrolled over a period of 30 months. The diagnostic criteria for SLE were based on the 1997 revision of the 1982 American College of Rheumatology classification criteria for SLE (25), whereas the clinical assessment of SLE disease activity was based on the SLE disease activity index (SLEDAI) (4). The SLE disease activity was assessed by a clinician, and a blood sample was taken whenever there was a significant change in the clinical disease activity, including deterioration or improvement in disease status. All SLE patients who completed the study were regularly followed up at the clinic for >6 months and their conditions were stable. The treatment is adjusted according to clinical condition with several medications, including hydroxychloroquine, sulfasalazine, azathioprine, prednisolone, and cyclosporine in the outpatient clinic. There was no pulse steroid or pulse cyclophosphamide treatment during the follow-up period.
The Institutional Review Committee on Human Research approved the study protocol, and all the participants provided informed consent. Patients were excluded if they had autoimmune diseases other than SLE.
All patients underwent complete medical examinations upon enrollment. Demography data, complement levels, and anti-ribosomal p autoantibody (a-rib p) and anti-double stranded DNA autoantibody levels were collected. All enrolled patients were monitored at outpatient clinics regularly.
Blood samples were collected twice by venipuncture of the forearm veins of the SLE patients. The first samples were obtained at study enrollment, and the second samples were obtained whenever the disease activity changed, either clinically or serologically. The study was approved by Chang Gung Memorial Hospital's Institutional Review Committee on Human Research, 102-4669B, and 103-7505B.
Western blot analysis
Intracellular protein levels of caspase-9, caspase-10, MAVS, MDA5, and pIRF7 in peripheral blood mononuclear cells were detected by western blotting as described in a previous study (27). MAVS is divided into 57 and 75 kDa (5), as demonstrated by Brubaker et al., who published their research about the two variants of MAVS in antiviral immunity. Caspase-9 was detected as a cleaved form of caspase-9 (37 kDa) or a lower molecular weight caspase-9 (47 kDa) (18). Caspase-10 is also cleaved, with the short caspase-10 (caspase-10, 44 kDa) and the long caspase-10 (caspase-10, 59 kDa) (19).
Statistical analysis
Data were expressed as mean ± standard deviation or median (interquartile range). Continuous variables between the baseline and the follow-up were logarithmically transformed to improve normality and compared using the paired t-test. The changes in SLEDAI scores and intracellular protein levels between the baseline and follow-up are represented by Δaverage SLEDAI score and Δintracellular protein levels, respectively. Correlation analysis was used to evaluate both the relationship between SLEDAI scores and intracellular protein levels, and the Δaverage SLEDAI score and Δintracellular protein levels using nonparametric analysis. All statistical calculations were performed using the SAS software package, version 9.1 (2002; SAS Statistical Institute, Cary, NC).
Results
Characteristics and clinical laboratory tests of the study patients
Patient data at baseline and follow-up are listed in Table 1. The median age of the 10 SLE patients was 43.5 years, and all patients were women. The leukocyte counts, hemoglobin levels, and platelet counts were comparable between enrollment and follow-up test. SLEDAI score decreased from 2.5 to 1 in average, and which is similar between the two indicated time points. Besides, biochemistry data, complement levels, and autoantibody levels were all comparable between the two time points (all p ≥ 0.05; Table 1).
Data presented as median (IQR).
Indicates p-value <0.05.
IQR, interquartile range; MAVS, mitochondrial antiviral signaling protein; MDA5, melanoma differentiation-associated protein 5; ND, not done; pIRF7, phosphorylated interferon regulator factor 7; SLE, systemic lupus erythematosus; SLEDAI, systemic lupus erythematosus disease activity index.
Intracellular protein levels at enrollment and follow-up examinations
The intracellular protein levels were determined by western blot, as given in Figure 1, with denstimetry references.
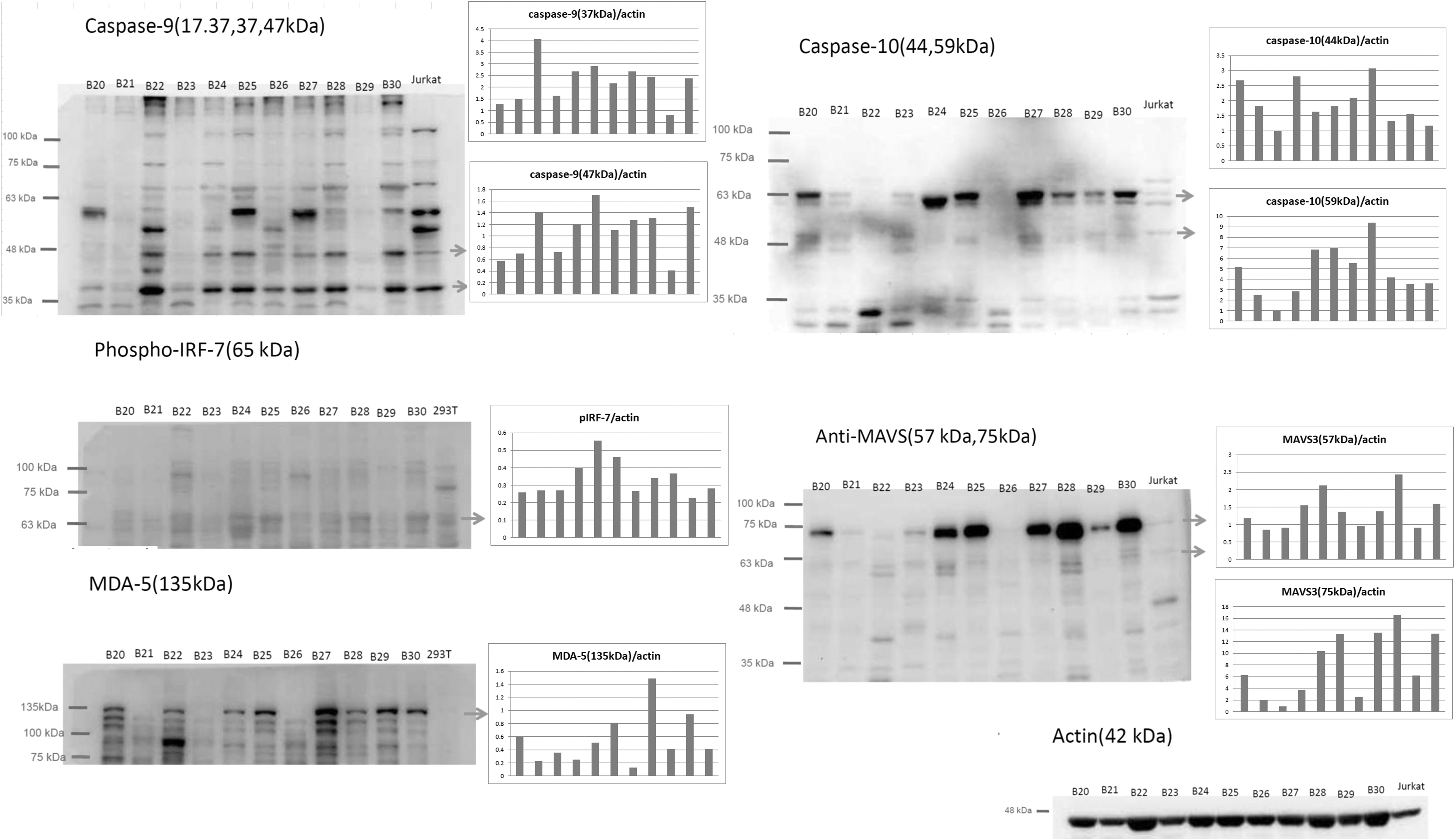
Western blot analysis of caspase-9, caspase-10, pIRF7, MDA5, and MAVS markers in systemic lupus erythematosus. Western blot analysis of caspase-9, caspase-10, pIRF7, MDA5, and MAVS markers in systemic lupus erythematosus (n = 11). The caspase-9 subunits were 37 and 47 kDa. The caspase-10 subunits were 44 and 59 kDa. The phosphorylated IRF-7 was 65 kDa, and its protein concentration was lower than that of other nonphosphorylated proteins. The MDA-5 was 135 kDa and the MAVS protein subunits were 57 and 75 kDa. The signal was quantified densitometrically by “Quantity One 1-D analysis” software (Bio-Rad USA, Life Science Research, Hercules, CA). Data were expressed as median (IQR). All samples were collected from patients with SLE (n = 11). The B23 sample was excluded from statistical analysis owing to missing baseline protein level data. IQR, interquartile range; MAVS, mitochondrial antiviral signaling protein; MDA5, melanoma differentiation associated protein 5; pIRF7, phosphorylated interferon regulator factor 7; SLE, systemic lupus erythematosus.
The changes in intracellular protein levels of patients between baseline and follow-up showed significant increases after regular follow-up and oral medication in caspase-9 (47 kDa)/actin (from 0.51 ± 0.44 to 1.28 ± 0.78), caspase-9 (37 kDa)/actin (from 0.66 ± 0.50 to 2.25 ± 0.96), caspase-10 (59 kDa)/actin (from 0.50 ± 0.70 to 3.90 ± 2.23), pIRF7/actin (from 0.04 ± 0.04 to 0.40 ± 0.18), MAVS (75 kDa)/actin (from 2.58 ± 2.61 to 7.95 ± 5.49), MAVS (57 kDa)/actin (from 0.67 ± 0.33 to 1.21 ± 0.60), and MDA5 (135 kDa)/actin (from 0.15 ± 0.24 to 0.83 ± 0.75). There was a trend, but no significant decrease in the SLEDAI scores in patients after regular follow-up and oral medication (p = 0.41; Table 1).
Correlations analysis between intracellular markers and disease activity
The interval of disease activity change varies from patient to patient, which was between 30 and 283 days in this study (188.5 ± 74.31 days). Correlation analysis was used to test the influence of Δintracellular markers on ΔSLEDAI score. The statistical results were as follows: Δcaspase-9 (47 kDa) (r = −0.24, p = 0.25), Δcaspase-9 (37 kDa) (r = 0.02, p = 0.48), Δcaspase-10 (59 kDa) (r = 0.01, p = 0.49), Δcaspase-10 (44 kDa) (r = 0.593, p = 0.04), ΔpIRF7 (r = −0.58, p = 0.04), ΔMAVS (75 kDa) (r = −0.587, p = 0.04), ΔMAVS (57 kDa) (r = 0.38, p = 0.14), and ΔMDA5 (135 kDa) (r = −0.914, p < 0.001). The correlations are listed in Table 2. The results demonstrated that the ΔSLEDAI score is negatively and significantly correlated with the antivirus marker concentration. In other words, antiviral immunity goes up when the disease activity goes down.
Indicates significant correlation; **Indicates p-value <0.05.
Δ, indicates changes between baseline and follow-up; p, p-value; r, correlation coefficient.
Discussion
In this study, we examined the changes in levels of antiviral immunity-associated proteins, including MDA5, MAVS, and pIRF7, as well as caspases, and their association with diseases activity in patients with SLE, producing two major findings. First, all the antiviral immunity-associated proteins tested, MDA5, MAVS, and pIRF7, showed significantly higher levels at follow-up. Second, these antiviral immunity-associated proteins were inversely correlated with diseases activity, whereas caspase-10 (44 kDa) was positively correlated with diseases activity during the follow-up study.
Our previous study demonstrated that MDA5 levels and those of MAVS and pIRF7 were significantly higher in SLE patients than other autoimmune patients (27), and it suggested that SLE patients are more frequently influenced by virus, similar to the results of an in vitro study with human islet cell cocultured with Coxsackievirus (7). The antiviral immunity cannot be represented totally by these five markers in this study; other markers such as AIM2 (absent in melanoma 2)-like receptors, cGAS (cyclic GMP-AMP synthase), and STING (stimulator of IFN genes) pathway proteins should also be involved in the SLE patients' antiviral immunity. The blood volume per test is set in this clinical study, so that only one pathway is studied in this project.
Mitochondrial dynamics influence the functions of MAVS that could also regulate its antiviral signaling (14). IRF7 is related to serum IFN-α activity triggered by endogenous nucleic acids in lupus patients, such as viral nucleic acids, that activate intracellular Toll-like receptors such as TLR7 or TLR9 (24,29). All these markers are significantly increased after clinical regular follow-up (Table 1). IRF7 levels increased after regular follow-up, which implies that antiviral immunity was also increased, and was inversely correlated with disease activity. MDA5 has been demonstrated to be associated with dermatomyositis (30) and lupus (9), and the MDA5 level was also inversely correlated with disease activity in SLE. One in vitro study also demonstrated that viral infections can induce expression and increased both MDA5 and IFN levels (7). Our study hints that subclinical viral infections that exist in SLE patients and antiviral immunity were inversely correlated with lupus disease activity (Table 2, right column). Thus, antiviral immunity is important to maintain the wellbeing of SLE patients.
The changes in caspase-10 (44 kDa) levels were positively correlated with the changes in SLEDAI (Table 2), which may be because of the extrinsic apoptosis pathway, such as tumor necrosis factor-α (17) and other stress signaling (22). Both caspase-9 and caspase-10 levels increased significantly after clinical regular follow-up and oral medication (Table 1), as did levels of the antiviral immunity proteins, MDA5, MAVS, and IRF7. These results may imply that the elevations in levels of these antiviral immunity proteins suppress the lupus activity. But, the viral infection/reactivation could persist, at least, subclinically, in lupus patients, and lead to increases in caspase-9 and caspase-10 levels. Overall, in our cohort, the viral infection is not obvious clinically. The antiviral immunity in lupus patients build up a defense against virus and it is inversely correlated with lupus activity.
The interval of disease activity change varies from patient to patient, which was between 30 and 283 days in this study (188.5 ± 74.31 days), the median interval of which was ∼6 months. This observation is consistent with the recent publication in a large lupus cohort that relapsing–remitting disease pattern is ∼53.8%, and chronic–active disease pattern is ∼15.5% in 1 year (13), and average annual flare rate was 23 per 100 patient-years in another study (18). The time interval between first blood test and the second blood test was dependent on the real disease fluctuations in each patient.
This study has two limitations. First, the mixture of intracellular proteins of lymphocyte and monocytes could be skewed as we focused on antiviral immunity. Hopefully, the major player of antiviral immunity, the lymphocytes, outnumbered the monocytes so that the effect was minimized. Despite no actual viral titers being available in this study, which is not our major concern, we would like to depict the concept that the antiviral immunity is generally important in lupus patients. The defensive immunity against the virus could be inversely associated with disease activity. Second, despite the longitudinal study, the patient number was small and the disease activity was relatively low. This simple assumption and study cannot reflect the actual unpredictable disease activity fluctuation in lupus. Nevertheless, we have a positive finding and prove our concept that the antiviral immunity has a role in tuning lupus activity. Large-scale prospective longitudinal studies with more active lupus patients are needed to evaluate the effect of antiviral immunity on clinical lupus disease activity.
Conclusion
This study provides some evidence for a link between antiviral immunity and the lupus disease activity clinically. The disease activity of SLE was inversely associated with levels of antiviral immunity-associated proteins, including MDA5, MAVS, and pIRF7. This suggests that evaluation of immunity against viral infection in patients with lupus may be worthwhile in certain circumstances.
Footnotes
Acknowledgments
The authors thank Special Interest Group of Lupus Research from Taiwan Rheumatology Association for comment and Dr. Ben-Chung Cheng for his help for English polishing. This work was supported by grants from Chang Gung Memorial Hospital-Kaohsiung Medical Center (CMRPG8G0271), and NMRPG8G6181, MOST-106-2314-B-182A-156-MY3.
Ethics Approval and Consent to Participate
The study was approved by Chang Gung Memorial Hospital's Institutional Review Committee on Human Research.
Availability of Data and Material
All the underlying research material related to our article can be accessed on demand by e-mail notification.
Authors' Contributions
Y.J.S. participated in the design of the study and drafted the article. Y.J.S. and W.C.C. conducted the sequence alignment and clinical evaluation of patients. H.C.K. and W.C.C. participated in its design and coordination, and H.C.K. helped draft the article. All authors read and approved the final article.
Author Disclosure Statement
The authors declare that they have no competing interests.